Distribution of Substance P and the Calcitonin Gene-Related Peptide in the Human Tensor Tympani Muscle
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Initial Stage of Fetal Development of the Pharyngotympanic Tube Cartilage with Special Reference to Muscle Attachments to the Tube
Original Article http://dx.doi.org/10.5115/acb.2012.45.3.185 pISSN 2093-3665 eISSN 2093-3673 Initial stage of fetal development of the pharyngotympanic tube cartilage with special reference to muscle attachments to the tube Yukio Katori1, Jose Francisco Rodríguez-Vázquez2, Samuel Verdugo-López2, Gen Murakami3, Tetsuaki Kawase4,5, Toshimitsu Kobayashi5 1Division of Otorhinolaryngology, Sendai Municipal Hospital, Sendai, Japan, 2Department of Anatomy and Embryology II, Faculty of Medicine, Complutense University, Madrid, Spain, 3Division of Internal Medicine, Iwamizawa Kojin-kai Hospital, Iwamizawa, 4Laboratory of Rehabilitative Auditory Science, Tohoku University Graduate School of Biomedical Engineering, 5Department of Otolaryngology-Head and Neck Surgery, Tohoku University Graduate School of Medicine, Sendai, Japan Abstract: Fetal development of the cartilage of the pharyngotympanic tube (PTT) is characterized by its late start. We examined semiserial histological sections of 20 human fetuses at 14-18 weeks of gestation. As controls, we also observed sections of 5 large fetuses at around 30 weeks. At and around 14 weeks, the tubal cartilage first appeared in the posterior side of the pharyngeal opening of the PTT. The levator veli palatini muscle used a mucosal fold containing the initial cartilage for its downward path to the palate. Moreover, the cartilage is a limited hard attachment for the muscle. Therefore, the PTT and its cartilage seemed to play a critical role in early development of levator veli muscle. In contrast, the cartilage developed so that it extended laterally, along a fascia-like structure that connected with the tensor tympani muscle. This muscle appeared to exert mechanical stress on the initial cartilage. -

Tonic Tensor Tympani Syndrome (TTTS)
Tonic Tensor Tympani Syndrome (TTTS) http://www.dineenandwestcott.com.au/hyperacusis.php?fid=1 Retrieved 15ththth May 2009 In the middle ear, the tensor tympani muscle and the stapedial muscle contract to tighten the middle ear bones (the ossicles) as a reaction to loud, potentially damaging sound. This provides protection to the inner ear from these loud sounds. In many people with hyperacusis, an increased, involuntary activity can develop in the tensor tympani muscle in the middle ear as part of a protective and startle response to some sounds. This lowered reflex threshold for tensor tympani contraction is activated by the perception/anticipation of sudden, unexpected, loud sound, and is called tonic tensor tympani syndrome (TTTS). In some people with hyperacusis, it appears that the tensor tympani muscle can contract just by thinking about a loud sound. Following exposure to intolerable sounds, this heightened contraction of the tensor tympani muscle: • tightens the ear drum • stiffens the middle ear bones (ossicles) • can lead to irritability of the trigeminal nerve, which innervates the tensor tympani muscle; and to other nerves supplying the ear drum • can affect the airflow into the middle ear. The tensor tympani muscle functions in coordination with the tensor veli palatini muscle. When we yawn or swallow, these muscles work together to open the Eustachian tube. This keeps the ears healthy by clearing the middle ear of any accumulated fluid and allows the ears to “pop” by equalising pressure caused by altitude changes. TTTS can lead to a range of symptoms in and around the ear(s): ear pain; pain in the jaw joint and down the neck; a fluttering sensation in the ear; a sensation of fullness in the ear; burning/numbness/tingling in and around the ear; unsteadiness; distorted hearing. -

ANATOMY of EAR Basic Ear Anatomy
ANATOMY OF EAR Basic Ear Anatomy • Expected outcomes • To understand the hearing mechanism • To be able to identify the structures of the ear Development of Ear 1. Pinna develops from 1st & 2nd Branchial arch (Hillocks of His). Starts at 6 Weeks & is complete by 20 weeks. 2. E.A.M. develops from dorsal end of 1st branchial arch starting at 6-8 weeks and is complete by 28 weeks. 3. Middle Ear development —Malleus & Incus develop between 6-8 weeks from 1st & 2nd branchial arch. Branchial arches & Development of Ear Dev. contd---- • T.M at 28 weeks from all 3 germinal layers . • Foot plate of stapes develops from otic capsule b/w 6- 8 weeks. • Inner ear develops from otic capsule starting at 5 weeks & is complete by 25 weeks. • Development of external/middle/inner ear is independent of each other. Development of ear External Ear • It consists of - Pinna and External auditory meatus. Pinna • It is made up of fibro elastic cartilage covered by skin and connected to the surrounding parts by ligaments and muscles. • Various landmarks on the pinna are helix, antihelix, lobule, tragus, concha, scaphoid fossa and triangular fossa • Pinna has two surfaces i.e. medial or cranial surface and a lateral surface . • Cymba concha lies between crus helix and crus antihelix. It is an important landmark for mastoid antrum. Anatomy of external ear • Landmarks of pinna Anatomy of external ear • Bat-Ear is the most common congenital anomaly of pinna in which antihelix has not developed and excessive conchal cartilage is present. • Corrections of Pinna defects are done at 6 years of age. -

Yagenich L.V., Kirillova I.I., Siritsa Ye.A. Latin and Main Principals Of
Yagenich L.V., Kirillova I.I., Siritsa Ye.A. Latin and main principals of anatomical, pharmaceutical and clinical terminology (Student's book) Simferopol, 2017 Contents No. Topics Page 1. UNIT I. Latin language history. Phonetics. Alphabet. Vowels and consonants classification. Diphthongs. Digraphs. Letter combinations. 4-13 Syllable shortness and longitude. Stress rules. 2. UNIT II. Grammatical noun categories, declension characteristics, noun 14-25 dictionary forms, determination of the noun stems, nominative and genitive cases and their significance in terms formation. I-st noun declension. 3. UNIT III. Adjectives and its grammatical categories. Classes of adjectives. Adjective entries in dictionaries. Adjectives of the I-st group. Gender 26-36 endings, stem-determining. 4. UNIT IV. Adjectives of the 2-nd group. Morphological characteristics of two- and multi-word anatomical terms. Syntax of two- and multi-word 37-49 anatomical terms. Nouns of the 2nd declension 5. UNIT V. General characteristic of the nouns of the 3rd declension. Parisyllabic and imparisyllabic nouns. Types of stems of the nouns of the 50-58 3rd declension and their peculiarities. 3rd declension nouns in combination with agreed and non-agreed attributes 6. UNIT VI. Peculiarities of 3rd declension nouns of masculine, feminine and neuter genders. Muscle names referring to their functions. Exceptions to the 59-71 gender rule of 3rd declension nouns for all three genders 7. UNIT VII. 1st, 2nd and 3rd declension nouns in combination with II class adjectives. Present Participle and its declension. Anatomical terms 72-81 consisting of nouns and participles 8. UNIT VIII. Nouns of the 4th and 5th declensions and their combination with 82-89 adjectives 9. -
Audiometric Findings with Voluntary Tensor Tympani Contraction Brandon Wickens1 , Duncan Floyd2 and Manohar Bance3*
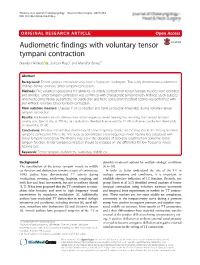
Wickens et al. Journal of Otolaryngology - Head and Neck Surgery (2017) 46:2 DOI 10.1186/s40463-016-0182-y ORIGINALRESEARCHARTICLE Open Access Audiometric findings with voluntary tensor tympani contraction Brandon Wickens1 , Duncan Floyd2 and Manohar Bance3* Abstract Background: Tensor tympani contraction may have a "signature" audiogram. This study demonstrates audiometric findings during voluntary tensor tympani contraction. Methods: Five volunteers possessing the ability to voluntarily contract their tensor tympani muscles were identified and enrolled. Tensor tympani contraction was confirmed with characteristic tympanometry findings. Study subjects underwent conventional audiometry. Air conduction and bone conduction threshold testing was performed with and without voluntary tensor tympani contraction. Main outcome measure: Changes in air conduction and bone conduction thresholds during voluntary tensor tympani contraction. Results: Audiometric results demonstrate a low frequency mixed hearing loss resulting from tensor tympani contraction. Specifically, at 250 Hz, air conduction thresholds increased by 22 dB and bone conduction thresholds increased by 10 dB. Conclusions: Previous research has demonstrated a low frequency conductive hearing loss in the setting of tensor tympanic contraction. This is the first study to demonstrate a low frequency mixed hearing loss associated with tensor tympani contraction. This finding may aid in the diagnosis of disorders resulting from abnormal tensor tympani function. Tensor tympani contraction -
Endoscopic Treatment of Middle Ear Myoclonus with Stapedius and Tensor Tympani Section: a New Minimally-Invasive Approach
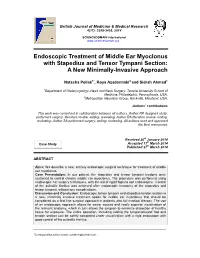
British Journal of Medicine & Medical Research 4(17): 3398-3405, 2014 SCIENCEDOMAIN international www.sciencedomain.org Endoscopic Treatment of Middle Ear Myoclonus with Stapedius and Tensor Tympani Section: A New Minimally-Invasive Approach Natasha Pollak1*, Roya Azadarmaki2 and Sidrah Ahmad1 1Department of Otolaryngology–Head and Neck Surgery, Temple University School of Medicine, Philadelphia, Pennsylvania, USA. 2Metropolitan NeuroEar Group, Rockville, Maryland, USA. Authors’ contributions This work was carried out in collaboration between all authors. Author NP designed study, performed surgery, literature review, writing, reviewing. Author RA literature review, writing, reviewing. Author SA performed surgery, writing, reviewing. All authors read and approved the final manuscript. Received 26th January 2014 th Case Study Accepted 11 March 2014 Published 27th March 2014 ABSTRACT Aims: We describe a new, entirely endoscopic surgical technique for treatment of middle ear myoclonus. Case Presentation: In our patient, the stapedius and tensor tympani tendons were sectioned to control chronic middle ear myoclonus. The procedure was performed using endoscopic ear surgery techniques, with the aid of rigid Hopkins rod endoscopes. Control of the pulsatile tinnitus was achieved after endoscopic tenotomy of the stapedius and tensor tympani, without any complications. Discussion and Conclusion: Endoscopic tensor tympani and stapedius tendon section is a new, minimally invasive treatment option for middle ear myoclonus that should be considered as a first line surgical approach in patients who fail medical therapy. The use of an endoscopic approach allows for easier access and vastly superior visualization of the relevant anatomy, which in turn allows the surgeon to minimize dissection of healthy tissue for exposure. The entire operation, including raising the tympanomeatal flap and tendon section can be safely completed under visualization with a rigid endoscope with good control of the pulsatile tinnitus. -

FIPAT-TA2-Part-2.Pdf
TERMINOLOGIA ANATOMICA Second Edition (2.06) International Anatomical Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TA2, PART II Contents: Systemata musculoskeletalia Musculoskeletal systems Caput II: Ossa Chapter 2: Bones Caput III: Juncturae Chapter 3: Joints Caput IV: Systema musculare Chapter 4: Muscular system Bibliographic Reference Citation: FIPAT. Terminologia Anatomica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, 2019 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Anatomica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput II: OSSA Chapter 2: BONES Latin term Latin synonym UK English US English English synonym Other 351 Systemata Musculoskeletal Musculoskeletal musculoskeletalia systems systems -

THE EFFECTS of ETHYL ALCOHOL on CONTRALATERAL and IPSILATERAL ACOUSTIC REFLEX THRESHOLDS Edward N. Cohill a Dissertation Submitt
THE EFFECTS OF ETHYL ALCOHOL ON CONTRALATERAL AND IPSILATERAL ACOUSTIC REFLEX THRESHOLDS Edward N. Cohill A Dissertation Submitted to the Graduate College of Bowling Green State University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY June 1978 XI ABSTRACT Acoustic reflex thresholds were measured at intervals in response to 500, 1000 and 2000Hz pure tones after the ingestion of a 50% solution of 100 proof vodka. These measurements were conducted to determine: 1. the effects of ethyl alcohol on the contralateral and ipsilateral acoustic reflex; 2. the relationship between acoustic reflex thresholds and blood alcohol concentration, and; 3. the relationship between acoustic reflex threshold shift following alcohol ingestion and the frequency of the elicit ing stimulus. Sight male and eight female normal-hearing adults served as subjects. Acoustic reflex threshold mea surements were obtained pre-ingestion and at blood alcohol concentrations of 0.02 to 0.10% in 0.01% increments. Blood alcohol measurements were made by the use of an electronic a 1c ohol-in-breath analyzer. Acoustic reflex measurements continued until blood alcohol concentrations were reduced to 0.02%. The greatest acoustic reflex threshold shifts occurred at 0.10% blood alcohol concentration. The shifts were approximately 11dB for contralateral stimulation and 7dB for ipsilateral acoustic reflexes for all frequencies. Thus, the effects of ethyl alcohol were more pronounced on contralateral than on ipsilateral reflexes. These effects iil were linear, and the rate of increase in acoustic reflex thresholds was only significantly different at the extremes of the measured blood alcohol concentration levels. Acoust ic reflex threshold shifts which resulted from the ingestion of ethyl alcohol did not show significant differences as a function of the frequency of the reflex eliciting stimuli. -

Evaluation of Human Ear Anatomy and Functionality by Axiomatic Design
biomimetics Article Evaluation of Human Ear Anatomy and Functionality by Axiomatic Design Pratap Sriram Sundar 1, Chandan Chowdhury 2 and Sagar Kamarthi 3,* 1 Indian School of Business, Mohali 160062, India; [email protected] 2 Indian School of Business, Gachibowli, Hyderabad 500111, India; [email protected] 3 Department of Mechanical and Industrial Engineering, Northeastern University, Boston, MA 02115, USA * Correspondence: [email protected]; Tel.: +1-617-373-3070 Abstract: The design of the human ear is one of nature’s engineering marvels. This paper examines the merit of ear design using axiomatic design principles. The ear is the organ of both hearing and balance. A sensitive ear can hear frequencies ranging from 20 Hz to 20,000 Hz. The vestibular apparatus of the inner ear is responsible for the static and dynamic equilibrium of the human body. The ear is divided into the outer ear, middle ear, and inner ear, which play their respective functional roles in transforming sound energy into nerve impulses interpreted in the brain. The human ear has many modules, such as the pinna, auditory canal, eardrum, ossicles, eustachian tube, cochlea, semicircular canals, cochlear nerve, and vestibular nerve. Each of these modules has several subparts. This paper tabulates and maps the functional requirements (FRs) of these modules onto design parameters (DPs) that nature has already chosen. The “independence axiom” of the axiomatic design methodology is applied to analyze couplings and to evaluate if human ear design is a good design (i.e., uncoupled design) or a bad design (i.e., coupled design). The analysis revealed that the human ear is a perfect design because it is an uncoupled structure. -

How Do Middle Ear Muscles Protect the Cochlea? Reconsideration of the Intralabyrinthine Pressure Theory
HOW DO MIDDLE EAR MUSCLES PROTECT THE COCHLEA? RECONSIDERATION OF THE INTRALABYRINTHINE PRESSURE THEORY Andrew Bell Research School of Biology, College of Medicine, Biology and Environment, The Australian National University, Canberra, ACT 0200, Australia Abstract The middle ear muscles are part of a control system for regulating the acoustic input to a supersensitive detector, the cochlea, preventing overload and damage. Yet there is a long-standing paradox. When Békésy measured sound transmission through the middle ear of cadavers, he found that acoustic transmission was not affected when the annular ligament was stretched by pressure. Similarly, reflex activation experiments often show only a few decibels of attenuation, assumed to be due to stiffen- ing of middle ear joints and ligaments. In contrast, psychophysical experiments reveal attenuations of 30 dB or more when the middle ear muscles are voluntarily contracted. How can the difference be explained? This synthesis paper shows how the paradox can be resolved by reconsidering a theory put forward by Gellé in the 19th century. According to Gellé’s intralabyrin- thine pressure theory, which has long been dismissed, the purpose of the middle ear muscles is to press the stapes inwards and raise the hydraulic pressure in the labyrinthine fluids, thereby regulating cochlear sensitivity. The focus of this review is to re- visit the theory and show how it can explain a range of audiological findings. The theory is updated and the hypothesis made that static pressure in the cochlear fluids is sensed by the outer hair cells, which are in continuous hydraulic connection with the stapes. It is this factor which reduces the gain of the cochlear amplifier and provides rapid and effective overload protec- tion. -

An Integrative Model Accounting for the Symptom Cluster Triggered After an Acoustic Shock
An Integrative Model Accounting for the Symptom Cluster Triggered After an Acoustic Shock Arnaud Noreña, Philippe Fournier, Alain Londero, Damien Ponsot, Nicolas Charpentier To cite this version: Arnaud Noreña, Philippe Fournier, Alain Londero, Damien Ponsot, Nicolas Charpentier. An Integra- tive Model Accounting for the Symptom Cluster Triggered After an Acoustic Shock. Trends in Hearing, SAGE Publications, 2018, 22, pp.233121651880172. 10.1177/2331216518801725. hal-02138904 HAL Id: hal-02138904 https://hal.archives-ouvertes.fr/hal-02138904 Submitted on 4 Mar 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Innovations in Tinnitus Research: Review Trends in Hearing Volume 22: 1–18 ! The Author(s) 2018 An Integrative Model Accounting Article reuse guidelines: sagepub.com/journals-permissions for the Symptom Cluster Triggered DOI: 10.1177/2331216518801725 After an Acoustic Shock journals.sagepub.com/home/tia Arnaud J. Noren˜a1, Philippe Fournier1, Alain Londero2, Damien Ponsot3, and Nicolas Charpentier4 Abstract Acoustic shocks and traumas sometimes result in a cluster of debilitating symptoms, including tinnitus, hyperacusis, ear fullness and tension, dizziness, and pain in and outside the ear. The mechanisms underlying this large variety of symptoms remain elusive. -

Acoustic Reflex: Middle Ear Muscles Physically Sense Eardrum Vibration
View metadata, citation and similar papers at core.ac.uk brought to you by CORE © J Hear Sci, 2017; 7(4): 33–44 provided by The Australian National University DOI: 10.17430/1002944 A FAST, “ZERO SYNAPSE” ACOUSTIC REFLEX: MIDDLE EAR MUSCLES PHYSICALLY SENSE Contributions: EARDRUM VIBRATION A Study design/planning B Data collection/entry ADEF C Data analysis/statistics Andrew Bell D Data interpretation E Preparation of manuscript F Literature analysis/search John Curtin School of Medical Research, The Australian National University, Canberra, G Funds collection Australia Corresponding author : Andrew Bell, JCSMR, 131 Garran Road, Australian National University, Canberra, ACT 2601, Australia, email: [email protected] Abstract The middle ear muscles may be inconspicuous, but they are special. Silently standing guard at the entrance to the inner ear, their role is to spring into action whenever sound input rises, protecting the highly sensitive cochlea from overload. Such a task requires the utmost speed, for sounds can reach damaging levels within milliseconds. Neural-mediated mechanisms are slow, with the acoustic reflex arc taking up to a hundred milliseconds or more. Here, evidence is assembled that the middle ear muscles have recruited an additional, faster mechanism. The proposal is made that these muscles have developed a preflex mechanism – a zero-synapse system inherent to muscle fibres which, in response to vibration, rapidly stiffens the muscles. Preflexes are a developed form of sensitivity to perturbation common to all muscles, and have recent- ly been identified in leg muscles, for example. However, the advantages that preflexes confer to an animal’s auditory system have not yet been recognized.