Functional Human Anatomy Lab #7 Upper Extremity Musculature
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Isolated Avulsion Fracture of the Lesser Tuberosity of The
(aspects of trauma) Isolated Avulsion Fracture of the Lesser Tuberosity of the Humerus in an Adult: Case Report and Literature Review Aman Dhawan, MD, Kevin Kirk, DO, Thomas Dowd, MD, and William Doukas, MD solated avulsion fractures of also describe our operative technique, comminuted 3-cm lesser tuberosity the lesser tuberosity of the including use of heavy, nonabsorb- fracture fragment retracted approxi- proximal humerus are rare. able suture. mately 2 cm from the donor site We report the case of a right- (Figures 1B–1D). No biceps tendon Ihand–dominant woman in her early ASE EPORT subluxation or injury and no intra- C R 30s who sustained such an injury, A right-hand–dominant woman in articular pathology were noted. with an intact subscapularis tendon her early 30s presented with right The lesser tuberosity fracture was attached to the lesser tuberosity frag- shoulder pain 1 day after a fall down surgically repaired less than 2 weeks ment. Treatment included surgery to a flight of stairs. During the acci- after injury. Through a deltopectoral restore tension to the subscapularis dent, as her feet slipped out from approach, the rotator interval and muscle and maintain the force couple underneath her and her torso fell the 3×2-cm fracture fragment were about the shoulder joint. One year after injury, the patient reported no pain, excellent range of motion, and “[To be diagnosed] this injury...requires... return to activities. This case demonstrates the diag- careful review of orthogonal radiographs nostic challenge of this injury, which requires a high index of suspicion and and advanced imaging.” careful review of orthogonal radio- graphs and advanced imaging. -

Body Mechanics As the Rotator Cuff Gether in a Cuff-Shape Across the Greater and Lesser Tubercles the on Head of the Humerus
EXPerT CONTENT Body Mechanics by Joseph E. Muscolino | Artwork Giovanni Rimasti | Photography Yanik Chauvin Rotator Cuff Injury www.amtamassage.org/mtj WORKING WITH CLieNTS AFFecTED BY THIS COmmON CONDITION ROTATOR CUFF GROUP as the rotator cuff group because their distal tendons blend and attach to- The four rotator cuff muscles are gether in a cuff-shape across the greater and lesser tubercles on the head of the supraspinatus, infraspinatus, the humerus. Although all four rotator cuff muscles have specific concen- teres minor, and subscapularis (Fig- tric mover actions at the glenohumeral (GH) joint, their primary functional ure 1). These muscles are described importance is to contract isometrically for GH joint stabilization. Because 17 Before practicing any new modality or technique, check with your state’s or province’s massage therapy regulatory authority to ensure that it is within the defined scope of practice for massage therapy. the rotator cuff group has both mover and stabilization roles, it is extremely functionally active and therefore often physically stressed and injured. In fact, after neck and low back conditions, the shoulder is the most com- Supraspinatus monly injured joint of the human body. ROTATOR CUFF PATHOLOGY The three most common types of rotator cuff pathology are tendinitis, tendinosus, and tearing. Excessive physi- cal stress placed on the rotator cuff tendon can cause ir- ritation and inflammation of the tendon, in other words, tendinitis. If the physical stress is chronic, the inflam- matory process often subsides and degeneration of the fascial tendinous tissue occurs; this is referred to as tendinosus. The degeneration of tendinosus results in weakness of the tendon’s structure, and with continued Teres minor physical stress, whether it is overuse microtrauma or a macrotrauma, a rotator cuff tendon tear might occur. -

Intrinsic Hand Muscles of the Japanese Monkey, Macaca Fuscata
Anthropol.Sci. 102(Suppl.), 85-95,1994 Intrinsic Hand Muscles of the Japanese Monkey, Macaca fuscata TOSHIHIKO HOMMA AND TATSUO SAKAI Department of Anatomy, School of Medicine, Juntendo University, Hongo 2-1-1, Bunkyo-ku, Tokyo 113, Japan Received December 24, 1993 •ôGH•ô Abstract•ôGS•ô Anatomy of the intrinsic hand muscles in the Japanese monkeys was studied with an improved method to dissect the muscles and nerves in water after removal of the skeletal framework. The thenar eminence contained four muscles, namely m. abductor pollicis brevis, m. opponens pollicis, m, flexor pollicis brevis, and m. adductor pollicis. The hypothenar eminence contained four muscles, namely m. palmaris brevis, m. abductor digiti minimi, m. flexor digiti minimi brevis, and m. opponens digiti minimi. Majority of the thenar muscles are fused more or less with each other, so that clear separation of these muscles was difficult. The lumbrical muscles arose from the palmar parts of four main tendons of the deep flexor muscle to the second, third, fourth, and fifth digits. The mm, contrahentes arose mainly from a medial tendinous septum attached on the palmar surface to the third metacarpus, and included three muscles destined to the second, fourth and fifth digits. The interossei were found on the radial side of the second, third, fourth and fifth finger as well as on the ulnar side of the second, third and fourth finger. The intrinsic hand muscles in the Japanese monkey received innervation either from the median or the ulnar nerve. Branching pattern of these nerves to the individual muscles was fundamentally similar to those in man except for the fact that the median and the ulnar nerve in the Japanese monkey do not communi cateto make a loop in the thenar muscles. -

Should Joint Presentation File
6/5/2017 The Shoulder Joint Bones of the shoulder joint • Scapula – Glenoid Fossa Infraspinatus fossa – Supraspinatus fossa Subscapular fossa – Spine Coracoid process – Acromion process • Clavicle • Humerus – Greater tubercle Lesser tubercle – Intertubercular goove Deltoid tuberosity – Head of Humerus Shoulder Joint • Bones: – humerus – scapula Shoulder Girdle – clavicle • Articulation – glenohumeral joint • Glenoid fossa of the scapula (less curved) • head of the humerus • enarthrodial (ball and socket) 1 6/5/2017 Shoulder Joint • Connective tissue – glenoid labrum: cartilaginous ring, surrounds glenoid fossa • increases contact area between head of humerus and glenoid fossa. • increases joint stability – Glenohumeral ligaments: reinforce the glenohumeral joint capsule • superior, middle, inferior (anterior side of joint) – coracohumeral ligament (superior) • Muscles play a crucial role in maintaining glenohumeral joint stability. Movements of the Shoulder Joint • Arm abduction, adduction about the shoulder • Arm flexion, extension • Arm hyperflexion, hyperextension • Arm horizontal adduction (flexion) • Arm horizontal abduction (extension) • Arm external and internal rotation – medial and lateral rotation • Arm circumduction – flexion, abduction, extension, hyperextension, adduction Scapulohumeral rhythm • Shoulder Joint • Shoulder Girdle – abduction – upward rotation – adduction – downward rotation – flexion – elevation/upward rot. – extension – Depression/downward rot. – internal rotation – Abduction (protraction) – external rotation -

Pronator Syndrome: Clinical and Electrophysiological Features in Seven Cases
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.39.5.461 on 1 May 1976. Downloaded from Journal ofNeurology, Neurosurgery, and Psychiatry, 1976, 39, 461-464 Pronator syndrome: clinical and electrophysiological features in seven cases HAROLD H. MORRIS AND BRUCE H. PETERS From the Department ofNeurology, University of Texas Medical Branch, Galveston, Texas, USA SYNOPSIS The clinical and electrophysiological picture of seven patients with the pronator syndrome is contrasted with other causes ofmedian nerve neuropathy. In general, these patients have tenderness over the pronator teres and weakness of flexor pollicis longus as well as abductor pollicis brevis. Conduction velocity of the median nerve in the proximal forearm is usually slow but the distal latency and sensory nerve action potential at the wrist are normal. Injection of corticosteroids into the pronator teres has produced relief of symptoms in a majority of patients. Protected by copyright. In the majority of isolated median nerve dys- period 101 cases of the carpal tunnel syndrome functions the carpal tunnel syndrome is appropri- and the seven cases of the pronator syndrome ately first suspected. The median nerve can also reported here were identified. Median nerve be entrapped in the forearm giving rise to a conduction velocity determinations were made on similar picture and an erroneous diagnosis. all of these patients. The purpose of this report is to draw full attention to the pronator syndrome and to the REPORT OF CASES features which allow it to be distinguished from Table 1 provides clinical details of seven cases of the median nerve entrapment at other sites. -

Wrist and Hand Examina[On
Wrist and Hand Examinaon Daniel Lueders, MD Assistant Professor Physical Medicine and Rehabilitaon Objecves • Understand the osseous, ligamentous, tendinous, and neural anatomy of the wrist and hand • Outline palpable superficial landmarks in the wrist and hand • Outline evaluaon of and differen.aon between nerves to the wrist and hand • Describe special tes.ng of wrist and hand Wrist Anatomy • Radius • Ulna • Carpal bones Wrist Anatomy • Radius • Ulna • Carpal bones Wrist Anatomy • Radius • Ulna • Carpal bones Wrist Anatomy • Radius • Ulna • Carpal bones Inspec.on • Ecchymosis • Erythema • Deformity • Laceraon Inspec.on • Common Finger Deformies • Swan Neck Deformity • Boutonniere Deformity • Hypertrophic nodules • Heberden’s, Bouchard’s Inspec.on • Swan Neck Deformity • PIP hyperextension, DIP flexion • Pathology is at PIP joint • Insufficiency of volar/palmar plate and suppor.ng structures • Distally, the FDP tendon .ghtens from PIP extension causing secondary DIP flexion • Alternavely, extensor tendon rupture produces similar deformity Inspec.on • Boutonniere Deformity • PIP flexion, DIP hyperextension • Pathology is at PIP joint • Commonly occurs from insufficiency of dorsal and lateral suppor.ng structures at PIP joint • Lateral bands migrate volar/palmar, creang increased flexion moment • Results in PIP “buTon hole” effect dorsally Inspec.on • Nodules • Osteoarthri.c • Hypertrophic changes of OA • PIP - Bouchard’s nodule • DIP - Heberden’s nodule • Rheumatoid Arthri.s • MCP joints affected most • Distal radioulnar joint can also be affected -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Analysis on the Acromial Curvature and Its Relationships with The
r e v b r a s o r t o p . 2 0 1 4;4 9(6):636–641 www.rbo.org.br Original article Analysis on the acromial curvature and its relationships with the subacromial space and ଝ,ଝଝ types of acromion a,b,∗ c José Aderval Aragão , Leonardo Passos Silva , b a Francisco Prado Reis , Camilla Sá dos Santos Menezes a Department of Morphology, Universidade Federal de Sergipe (UFS), Aracaju, SE, Brazil b Medical School, Universidade Tiradentes (UNIT), Aracaju, SE, Brazil c Orthopedics and Traumatology Service, Hospital Santa Casa de Belo Horizonte, Belo Horizonte, MG, Brazil a r t i c l e i n f o a b s t r a c t Article history: Objective: To correlate the acromial curvature, using the angles proposed, with the subacro- Received 13 September 2013 mial space and types of acromion. Accepted 24 October 2013 Methods: Ninety scapulas were studied. The acromia were classified as types I, II or III. The Available online 31 October 2014 acromial curvature was analyzed by means of the alpha, beta and theta angles. We also measured the distance between the anteroinferior extremity of the acromion and the supra- Keywords: glenoid tubercle (DA). The scapulas were grouped in relation to sex and age. The angles proposed were analyzed in relation to each type of acromion and also in relation to the Acromion/anatomy & histology Shoulder collision syndrome measurements of the distance DA. Rotator cuff Results: Out of the total number of acromia, 39 (43.3%) were type I, 43 (47.7%) type II and eight (9%) type III. -

Nerve Transfer Techniques in Injuries from the Upper Limb
THIEME Update Article | Artículo de Actualización 57 Nerve Transfer Techniques in Injuries from the Upper Limb Técnicas de transferencia nerviosa en lesiones del miembro superior Francisco Martínez Martínez1 B. Ñíguez Sevilla2 J. García García2 A. García López3 1 FEA (field medcial expert), Orthopaedics and Traumatology Surgery, Address for correspondence Francisco Martínez Martínez, C/ Canovas Hospital Clínico Universitario Virgen de la Arrixaca. Murcia, Spain del Castillo n°7- 4°a. 30003-Murcia, Spain 2 Resident, Orthopaedics and Traumatology Surgery, Hospital Clínico (e-mail: [email protected]). Universitario Virgen de la Arrixaca, Murcia, Spain 3 FEA (field medcial expert), Orthopaedics and Traumatology Surgery, Hospital General de Alicante, Alicante, Spain Rev Iberam Cir Mano 2017;45:57–67. Abstract Proximal nerve injuries from the upper limb or the braquial plexus are associated with a poor prognosis, even with prompt repair. In the last few decades an increase in nerve transfer techniques has occurred, by which a denervated peripheral nerve is reinner- vated by a healthy donor nerve. Nerve transfers are indicated in proximal brachial plexus injuries where grafting is not possible or in proximal injuries of peripheral nerves with long reinnervation distances. Nerve transfers represent a revolution in peripheral nerve surgery and offer the potential for superior functional recovery in severe nerve injuries. In complete brachial plexus injuries, there are being studied the existence of nerve roots (intraplexual transfers). If they do not exist, the transference of nerves out of the plexus are used Keywords (extraplexual transfers) as the spinal accessory nerve, the phrenic nerve, the intercostal ► nerve transfers nerves, etc. ► brachial plexus In this update paper, the different motor intra and extraplexual nerve transfer ► nerve injury techniques are going to be reviewed. -
Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair
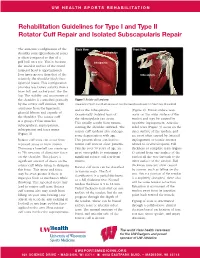
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair The anatomic configuration of the Back View Front View shoulder joint (glenohumeral joint) Supraspinatus is often compared to that of a golf ball on a tee. This is because Infraspinatus the articular surface of the round humeral head is approximately Teres four times greater than that of the Minor Subscapularis relatively flat shoulder blade face (glenoid fossa). This configuration provides less boney stability than a truer ball and socket joint, like the hip. The stability and movement of the shoulder is controlled primarily Figure 1 Rotator cuff anatomy by the rotator cuff muscles, with Image property of Primal Pictures, Ltd., primalpictures.com. Use of this image without authorization from Primal Pictures, Ltd. is prohibited. assistance from the ligaments, and/or the infraspinatus. (Figure 2). Bursal surface tears glenoid labrum and capsule of Occasionally isolated tears of occur on the outer surface of the the shoulder. The rotator cuff the subscapularis can occur. tendon and may be caused by is a group of four muscles: This usually results from trauma repetitive impingement. Articular subscapularis, supraspinatus, rotating the shoulder outward. The sided tears (Figure 3) occur on the infraspinatus and teres minor rotator cuff tendons also undergo inner surface of the tendon, and (Figure 1). some degeneration with age. are most often caused by internal Rotator cuff tears can occur from This process alone can lead to impingement or tensile stresses repeated stress or from trauma. rotator cuff tears in older patients. related to overhead sports. -

The Muscles That Act on the Upper Limb Fall Into Four Groups
MUSCLES OF THE APPENDICULAR SKELETON UPPER LIMB The muscles that act on the upper limb fall into four groups: those that stabilize the pectoral girdle, those that move the arm, those that move the forearm, and those that move the wrist, hand, and fingers. Muscles Stabilizing Pectoral Girdle (Marieb / Hoehn – Chapter 10; Pgs. 346 – 349; Figure 1) MUSCLE: ORIGIN: INSERTION: INNERVATION: ACTION: ANTERIOR THORAX: anterior surface coracoid process protracts & depresses Pectoralis minor* pectoral nerves of ribs 3 – 5 of scapula scapula medial border rotates scapula Serratus anterior* ribs 1 – 8 long thoracic nerve of scapula laterally inferior surface stabilizes / depresses Subclavius* rib 1 --------------- of clavicle pectoral girdle POSTERIOR THORAX: occipital bone / acromion / spine of stabilizes / elevates / accessory nerve Trapezius* spinous processes scapula; lateral third retracts / rotates (cranial nerve XI) of C7 – T12 of clavicle scapula transverse processes upper medial border elevates / adducts Levator scapulae* dorsal scapular nerve of C1 – C4 of scapula scapula Rhomboids* spinous processes medial border adducts / rotates dorsal scapular nerve (major / minor) of C7 – T5 of scapula scapula * Need to be familiar with on both ADAM and the human cadaver Figure 1: Muscles stabilizing pectoral girdle, posterior and anterior views 2 BI 334 – Advanced Human Anatomy and Physiology Western Oregon University Muscles Moving Arm (Marieb / Hoehn – Chapter 10; Pgs. 350 – 352; Figure 2) MUSCLE: ORIGIN: INSERTION: INNERVATION: ACTION: intertubercular