Is There a VA Advantage? Evidence from Dually Eligible Veterans
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fifth Report Data: January 2009 to December 2015
Fifth Report Data: January 2009 to December 2015 ‘Our daughter Helen is a statistic in these pages. Understanding why, has saved others.’ David White Ngā mate aituā o tātou Ka tangihia e tātou i tēnei wā Haere, haere, haere. The dead, the afflicted, both yours and ours We lament for them at this time Farewell, farewell, farewell. Citation: Family Violence Death Review Committee. 2017. Fifth Report Data: January 2009 to December 2015. Wellington: Family Violence Death Review Committee. Published in June 2017 by the Health Quality & Safety Commission, PO Box 25496, Wellington 6146, New Zealand ISBN 978-0-908345-60-1 (Print) ISBN 978-0-908345-61-8 (Online) This document is available on the Health Quality & Safety Commission’s website: www.hqsc.govt.nz For information on this report, please contact [email protected] ACKNOWLEDGEMENTS The Family Violence Death Review Committee is grateful to: • the Mortality Review Committee Secretariat based at the Health Quality & Safety Commission, particularly: – Rachel Smith, Specialist, Family Violence Death Review Committee – Joanna Minster, Senior Policy Analyst, Family Violence Death Review Committee – Kiri Rikihana, Acting Group Manager Mortality Review Committee Secretariat and Kaiwhakahaere Te Whai Oranga – Nikolai Minko, Principal Data Scientist, Health Quality Evaluation • Pauline Gulliver, Research Fellow, School of Population Health, University of Auckland • Dr John Little, Consultant Psychiatrist, Capital & Coast District Health Board • the advisors to the Family Violence Death Review Committee. The Family Violence Death Review Committee also thanks the people who have reviewed and provided feedback on drafts of this report. FAMILY VIOLENCE DEATH REVIEW COMMITTEE FIFTH REPORT DATA: JANUARY 2009 TO DECEMBER 2015 1 FOREWORD The Health Quality & Safety Commission (the Commission) welcomes the Fifth Report Data: January 2009 to December 2015 from the Family Violence Death Review Committee (the Committee). -

National Letter in Support of Federal All-Payer Claims Database
National Letter in Support of Federal All-Payer Claims Database As health scholars, leaders of health organizations, and funders of health research, we are writing in support of establishing a federal all-payer claims database (APCD). APCDs regularly collect data on health insurance claims from all of the payers in a given area (typically a state). Because they include demographic and diagnostic data on patients as well as any treatment or drug paid for by insurance (private or public), APCDs can be immensely valuable for research. APCDs have been used by health scholars to study numerous issues about quality and cost, including the extent of long-term opioid use after surgery, the ability of Medicaid patients to access physicians, the amount of wasted medical spending ending on low-value care, the performance of new models to reduce health spending (such as patient-centered medical home programs), the rate of complications after routine surgeries, and the characteristics of the highest-cost Medicaid patients. In 2016, however, the Supreme Court rendered it all but impossible for states to establish comprehensive APCDs, on the grounds that the Employee Retirement Income Security Act (ERISA) preempted states from requiring reporting by self-insured health plans. As noted in the Journal of the American Medical Association, this Supreme Court decision has “far-reaching implications for the ability of states to access comprehensive health information to inform policy making.” In May 2019, the Senate Health, Education, Labor and Pensions Committee released a draft of the Lower Health Care Costs Act. Among other things, that Act would amend ERISA to create a federal APCD whose data would be available to “researchers and policymakers.” While we are not all able to take a position on specific federal legislation, we can all agree that a national APCD would be an enormous leap forward for the ability of health researchers to study the cost and quality of medical care across the U.S. -

Environmental Health Biomed Central
Environmental Health BioMed Central Review Open Access Ancillary human health benefits of improved air quality resulting from climate change mitigation Michelle L Bell*1, Devra L Davis2, Luis A Cifuentes3, Alan J Krupnick4, Richard D Morgenstern4 and George D Thurston5 Address: 1School of Forestry and Environmental Studies, Yale University, New Haven, CT 06511, USA, 2Graduate School of Public Health, University of Pittsburgh, CNPAV 435, Pittsburgh, PA 15260, USA, 3Industrial and Systems Engineering Department, P. Catholic University of Chile, Engineering School, Santiago, Chile, 4Resources for the Future, Washington, DC 20036, USA and 5School of Medicine, New York University, Tuxedo, NY 10987, USA Email: Michelle L Bell* - [email protected]; Devra L Davis - [email protected]; Luis A Cifuentes - [email protected]; Alan J Krupnick - [email protected]; Richard D Morgenstern - [email protected]; George D Thurston - [email protected] * Corresponding author Published: 31 July 2008 Received: 4 April 2008 Accepted: 31 July 2008 Environmental Health 2008, 7:41 doi:10.1186/1476-069X-7-41 This article is available from: http://www.ehjournal.net/content/7/1/41 © 2008 Bell et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: Greenhouse gas (GHG) mitigation policies can provide ancillary benefits in terms of short-term improvements in air quality and associated health benefits. Several studies have analyzed the ancillary impacts of GHG policies for a variety of locations, pollutants, and policies. -

Reporter NATIONAL BUREAU of ECONOMIC RESEARCH
NBER Reporter NATIONAL BUREAU OF ECONOMIC RESEARCH A quarterly summary of NBER research No. 4, December 2017 Program Report ALSO IN THIS ISSUE Employment Changes for Cognitive Occupations, 2000–2012 Industrial Organization Percentage change in STEM and other managerial or professional occupations -20 0 20 40 60 * Teachers (K-12) Liran Einav and Jonathan Levin Managers (All) Nurses Health Technicians Health Therapists Comp. Sci./Programming/Tech. Support Accounting And Finance Economists & Survey Researchers Social Workers, Counselors & Clergy Physicians College Instructors Researchers in the Program on Industrial Organization (IO) study Lawyers and Judges Other Business Support consumer and firm behavior, competition, innovation, and govern- Operations Researchers Physicians' Assistants Medical Scientists ment regulation. This report begins with a brief summary of general Legal Assistants and Paralegals Pharmacists developments in the last three decades in the range and focus of pro- Dental Hygienists Mathematicians/Statisticians/Actuaries gram members’ research, then discusses specific examples of recent Dentists Social Scientists And Urban Planners Artists, Entertainers, and Athletes work. Marketing, Advertising and PR Pilots/Air Traic Control When the program was launched in the early 1990s, two devel- Biological Scientists Physical Scientists Architects opments had profoundly shaped IO research. One was development Writers, Editors, and Reporters Engineering And Science Technicians of game-theoretic models of strategic behavior by firms with market Draers And Surveyors 1 Engineers (All) power, summarized in Jean Tirole’s classic textbook. The initial wave -20 0 20 40 60 of research in this vein was focused on applying new insights from eco- Source: D. Deming, NBER Working Paper No. 21473 nomic theory; empirical applications came later. -

Assessing the Influence of Weather in 5 U.S. Cities During Wintertime High Mortality Days
ASSESSING THE INFLUENCE OF WEATHER IN 5 U.S. CITIES DURING WINTERTIME HIGH MORTALITY DAYS A thesis submitted to Kent State University in partial fulfillment of the requirements for the degree of Master of Arts by Michael James Allen December, 2010 Thesis written by Michael James Allen B.S., California University of Pennsylvania, 2008 M.A., Kent State University, 2010 Approved by ______________________, Dr. Scott Sheridan, Advisor ______________________, Dr. Mandy Munro-Stasiuk, Chair, Department of Geography ______________________, Dr. Timothy Moerland, Dean, College of Arts and Sciences ii TABLE OF CONTENTS Page LIST OF FIGURES........................................................................................................ vii LIST OF TABLES.......................................................................................................... ix ACKNOWLEDGEMENTS............................................................................................. xii CHAPTER 1 INTRODUCTION.................................................................................................... 1 CHAPTER 2 BACKGROUND...................................................................................................... 5 2.1 Weather Mortality..................................................................................... 5 2.1.1 Biological Causes................................................................................ 5 2.1.2 Socio-Economic, Demographic, and Behavioral Factors.................... 7 2.1.3 The Lag Effect and Mortality -

We, the Undersigned Economists, Represent a Broad Variety of Areas of Expertise and Are United in Our Opposition to Donald Trump
We, the undersigned economists, represent a broad variety of areas of expertise and are united in our opposition to Donald Trump. We recommend that voters choose a different candidate on the following grounds: . He degrades trust in vital public institutions that collect and disseminate information about the economy, such as the Bureau of Labor Statistics, by spreading disinformation about the integrity of their work. He has misled voters in states like Ohio and Michigan by asserting that the renegotiation of NAFTA or the imposition of tariffs on China would substantially increase employment in manufacturing. In fact, manufacturing’s share of employment has been declining since the 1970s and is mostly related to automation, not trade. He claims to champion former manufacturing workers, but has no plan to assist their transition to well-compensated service sector positions. Instead, he has diverted the policy discussion to options that ignore both the reality of technological progress and the benefits of international trade. He has misled the public by asserting that U.S. manufacturing has declined. The location and product composition of manufacturing has changed, but the level of output has more than doubled in the U.S. since the 1980s. He has falsely suggested that trade is zero-sum and that the “toughness” of negotiators primarily drives trade deficits. He has misled the public with false statements about trade agreements eroding national income and wealth. Although the gains have not been equally distributed—and this is an important discussion in itself—both mean income and mean wealth have risen substantially in the U.S. -

INAUGURAL CARIBBEAN HEALTH ECONOMICS SYMPOSIUM Bitter
INAUGURAL CARIBBEAN HEALTH ECONOMICS SYMPOSIUM Bitter End Yacht Club Virgin Gorda, British Virgin Islands Agenda – As of December 8, 2015 Sunday, December 13, 2015 Pre-Symposium Necker Island Tour Tour of Richard Branson’s personal island and nature park: 1:00pm to 3:30pm Personal invite from the Richard with opportunity to meet him personally at end of tour. Space is limited. Will leave from BEYC dock on symposia boats or motor launch to Necker Island. Welcome reception, 6:00pm, BEYC Town & Gown Exchange, 7:00pm, BEYC “Publications, Patents and Privacy: Holy Trinity or Bermuda Triangle of Health Economics Research”: Informal forum between policy makers, academics and industry Monday, December 14, 2014 Breakfast at BEYC 7:00 to 8:30 Paper - 8:30 to 9:30: Switching Costs and Plan Loyalty in Medicare Part C. Adam Atherly, University of Colorado, Denver Roger Feldman, University of Minnesota Bryan Dowd, University of Minnesota E. Van den Broek, University of Colorado, Denver Paper - 9:30 to 10:30: Insurer Competition in Health Care Markets Kate Ho, Columbia University Robin S. Lee, Harvard University Coffee and electronic catch-up 10:30 to 11:00 Paper - 11:00 to Noon: Marginal Treatment Effects and the External Validity of the Oregon Health Insurance Experiment Amanda Kowalski, Yale University Afternoon choices and preferences o Afternoon Activities arranged independently by BEYC staff - OR - o Sail excursion to The Baths on Virgin Gorda (with a possible race back) Happy Hour Town & Gown Exchange, 7:00pm, BEYC Has pharmacoeconomics lost its way? Panel discussion featuring work from Andrew Briggs (Glasgow, UK), Adrian Levy (Dalhousie, Canada) and David Henry (Toronto, Canada) paper. -
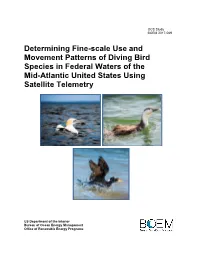
Determining Fine-Scale Use and Movement Patterns of Diving Bird Species in Federal Waters of the Mid-Atlantic United States Using Satellite Telemetry
OCS Study BOEM 2017-069 Determining Fine-scale Use and Movement Patterns of Diving Bird Species in Federal Waters of the Mid-Atlantic United States Using Satellite Telemetry US Department of the Interior Bureau of Ocean Energy Management Office of Renewable Energy Programs OCS Study BOEM 2017-069 Determining Fine-scale Use and Movement Patterns of Diving Bird Species in Federal Waters of the Mid-Atlantic United States Using Satellite Telemetry Authors Caleb S. Spiegel, USFWS Division of Migratory Birds (Project Manager, Editor) Alicia M. Berlin, USGS Patuxent Wildlife Research Center Andrew T. Gilbert, Biodiversity Research Institute Carrie O. Gray, Biodiversity Research Institute William A. Montevecchi, Memorial University of Newfoundland Iain J. Stenhouse, Biodiversity Research Institute Scott L. Ford, Avian Specialty Veterinary Services Glenn H. Olsen, USGS Patuxent Wildlife Research Center Jonathan L. Fiely, USGS Patuxent Wildlife Research Center Lucas Savoy, Biodiversity Research Institute M. Wing Goodale, Biodiversity Research Institute Chantelle M. Burke, Memorial University of Newfoundland Prepared under BOEM Intra-agency Agreement #M12PG00005 by U.S. Department of Interior U.S. Fish and Wildlife Service Division of Migratory Birds 300 Westgate Center Dr. Hadley, MA 01035 Published by U.S. Department of the Interior Bureau of Ocean Energy Management Office of Renewable Energy Programs 2017-069 DISCLAIMER This study was funded by the US Department of the Interior, Bureau of Ocean Energy Management (BOEM), Environmental Studies Program, Washington, DC, through Intra-agency Agreement Number M12PG00005 with the US Department of Interior, US Fish and Wildlife Service, Division of Migratory Birds, Hadley, MA. This report has been technically reviewed by BOEM and it has been approved for publication. -

Download This
25th Annual Health Economics Conference (A H E C) Thursday ± F riday, October 16-17, 2014 Dore Commons, Baker Institute for Public Policy Agenda General Presentation Timeline: Sessions will last approximately 50 minutes. Speakers will present for 35 minutes, followed by 10 minutes of questions from the discussant and 5 minutes for general questions. Thursday, October 16, 2014 Session 1: Medicare Reform Moderator: Vivian Ho 5LFH8QLYHUVLW\¶V%DNHU,QVWLWXWH 8:15 a.m. BREAKFAST 9:15 a.m. Welcome & Introduction 9LYLDQ+R 5LFH8QLYHUVLW\¶V%DNHUInstitute) 9:30 a.m. ³Does Privatized Health Insurance Benefit Patients or Producers? Evidence from Medicare Advantage´ Authors: Marika Cabral (University of Texas at Austin, presenting), Michael Geruso (University of Texas at Austin), and Neale Mahoney (University of Chicago) Discussant: Jason Abaluck (Yale University) 10:20 a.m. ´7KH,PSDFWRI&RQVXPHU,QDWWHQWLRQRQ,QVXUHU3ULFLng in the Medicare Part D 3URJUDP´ Authors: Kate Ho (Columbia University, presenting), Joseph Hogan (Columbia University), and Fiona Scott Morton (Yale University) Discussant: John Romley (University of Southern California) Paper not available online. 11:10 a.m. BREAK 11:30 a.m. ³Upcoding or Selection? Evidence from Medicare on Squishy Risk Adjustment´ Authors: Michael Geruso (Harvard University, University of Texas at Austin) and Timothy Layton (Harvard Medical School, presenting) Discussant: Colleen Carey (University of Michigan) 12:20 p.m. LUNCH Session 2: Improving Health Outcomes Moderator: Aimee Chin (University of Houston) 1:30 -

NBER WORKING PAPER SERIES DO INCREASING MARKUPS MATTER? LESSONS from EMPIRICAL INDUSTRIAL ORGANIZATION Steven T. Berry Martin Ga
NBER WORKING PAPER SERIES DO INCREASING MARKUPS MATTER? LESSONS FROM EMPIRICAL INDUSTRIAL ORGANIZATION Steven T. Berry Martin Gaynor Fiona Scott Morton Working Paper 26007 http://www.nber.org/papers/w26007 NATIONAL BUREAU OF ECONOMIC RESEARCH 1050 Massachusetts Avenue Cambridge, MA 02138 June 2019 We wish to thank Al Klevorick and editors at the Journal of Economics Perspectives—Enrico Moretti, Gordon Hanson, and managing editor Tim Taylor—for helpful comments and suggestions that substantially improved the paper. The usual caveat applies. The views expressed herein are those of the authors and do not necessarily reflect the views of the National Bureau of Economic Research. At least one co-author has disclosed a financial relationship of potential relevance for this research. Further information is available online at http://www.nber.org/papers/w26007.ack NBER working papers are circulated for discussion and comment purposes. They have not been peer-reviewed or been subject to the review by the NBER Board of Directors that accompanies official NBER publications. © 2019 by Steven T. Berry, Martin Gaynor, and Fiona Scott Morton. All rights reserved. Short sections of text, not to exceed two paragraphs, may be quoted without explicit permission provided that full credit, including © notice, is given to the source. Do Increasing Markups Matter? Lessons from Empirical Industrial Organization Steven T. Berry, Martin Gaynor, and Fiona Scott Morton NBER Working Paper No. 26007 June 2019 JEL No. L0,L1,L4 ABSTRACT This paper considers the recent literature on firm markups in light of both new and classic work in the field of Industrial Organization. We detail the shortcomings of papers that rely on discredited approaches from the “structure-conduct-performance” literature. -
Regulatory Impact Analysis for the Proposed Revised Cross-State Air Pollution Rule (CSAPR) Update for the 2008 Ozone NAAQS ERRATA SHEET
Regulatory Impact Analysis for the Proposed Revised Cross-State Air Pollution Rule (CSAPR) Update for the 2008 Ozone NAAQS ERRATA SHEET After completion of the RIA, EPA received revised production cost projections for the proposed rule IPM run, which reduced the projected cost of the proposed rule. This Errata presents these technical corrections. The first table presents the changes in the text and is followed by sets of tables each showing the current table and corrected table. Page numbers Current Value Corrected Value (Highlighted in yellow) ES-15 The estimated social costs to The estimated social costs to implement the proposal, as implement the proposal, as described in this document, described in this document, are approximately $21 are approximately $20 million in 2021 and $6 million in 2021 and $1 million in 2025 million in 2025 (2016$). (2016$). ES-16 The annual net benefits of the The annual net benefits of the proposal in 2021 (in 2016$) proposal in 2021 (in 2016$) are approximately -$21 are approximately -$20 million using a 3 percent million using a 3 percent discount rate and a 7 percent discount rate and a 7 percent real discount rate. The annual real discount rate. The annual net benefits of the proposal in net benefits of the proposal in 2025 are approximately $27 2025 are approximately $31 million using a 3 percent real million using a 3 percent real discount rate and discount rate and approximately -$0.9 million approximately $4 million using a 7 percent real using a 7 percent real discount rate. discount rate. ES-17 The present value The present value (PV) of the net benefits, in (PV) of the net benefits, in 2016$ and discounted to 2016$ and discounted to 2021, is -$68 million when 2021, is -$59 million when using a 7 percent using a 7 percent discount rate and $14 million discount rate and $23 million when using a 3 percent when using a 3 percent discount rate. -

Overton Power District No. 5 Power Transmission Expansion Project Environmental Assessment
DOI-BLM-NV-S010-2009-1020-EA Overton Power District No. 5 Power Transmission Expansion Project Environmental Assessment Clark County, Nevada March 2014 U.S. Department of the Interior Bureau of Land Management Las Vegas Field Office 4701 North Torrey Pines Las Vegas, NV 89130 Phone: 702-515-5000 Table of Contents 1.0 INTRODUCTION ............................................................................................................ 1 1.1 Background .................................................................................................................... 1 1.2 Purpose of and Need for the Proposed Action ............................................................... 8 1.3 Relationship to Statutes, Regulations, Plans or Other Environmental Analyses ............ 8 1.3.1 Conformance With Land Use Plan ........................................................................... 8 1.3.2 Local Land Use Plans ..................................................................................................... 8 1.3.3 Authorizing Actions ................................................................................................... 8 1.4 Scoping, Public Involvement, and Issues ....................................................................... 8 2.0 PROPOSED ACTION AND ALTERNATIVES .............................................................. 10 2.1 Alternative I – No Action Alternative ............................................................................. 10 2.2 Alternative II – Proposed Action ..................................................................................