The Yellow Flag of Quarantine: an Analysis of the Historical And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

North American Journal of Psychology, 1999. PUB DATE 1999-00-00 NOTE 346P.; Published Semi-Annually
DOCUMENT RESUME ED 449 388 CG 029 765 AUTHOR McCutcheon, Lynn E., Ed. TITLE North American Journal of Psychology, 1999. PUB DATE 1999-00-00 NOTE 346p.; Published semi-annually. AVAILABLE FROM NAJP, 240 Harbor Dr., Winter Garden, FL 34787 ($35 per annual subscription). Tel: 407-877-8364. PUB TYPE Collected Works Serials (022) JOURNAL CIT North American Journal of Psychology; vl n1-2 1999 EDRS PRICE MF01/PC14 Plus Postage. DESCRIPTORS *Psychology; *Research Tools; *Scholarly Journals; *Social Science Research ABSTRACT "North American Journal of Psychology" publishes scientific papers of general interest to psychologists and other social scientists. Articles included in volume 1 issue 1 (June 1999) are: "Generalist Looks at His Career in Teaching: Interview with Dr. Phil Zimbardo"; "Affective Information in Videos"; "Infant Communication"; "Defining Projective Techniques"; "Date Selection Choices in College Students"; "Study of the Personality of Violent Children"; "Behavioral and Institutional Theories of Human Resource Practices"; "Self-Estimates of Intelligence:"; "When the Going Gets Tough, the Tough Get Going"; "Behaviorism and Cognitivism in Learning Theory"; "On the Distinction between Behavioral Contagion, Conversion Conformity, and Compliance Conformity"; "Promoting Altruism in Troubled Youth"; The Influence of insecurity on Exchange and Communal Intimates"; "Height as Power in Women"; "Moderator Effects of Managerial Activity Inhibition on the Relation between Power versus Affiliation Motive Dominance and Econdmic Efficiency"; -

American Behavioral Scientist
American Behavioral Scientist http://abs.sagepub.com/ Social Network Influence on Online Behavioral Choices: Exploring Group Formation on Social Network Sites K. Hazel Kwon, Michael A. Stefanone and George A. Barnett American Behavioral Scientist published online 28 March 2014 DOI: 10.1177/0002764214527092 The online version of this article can be found at: http://abs.sagepub.com/content/early/2014/03/28/0002764214527092 Published by: http://www.sagepublications.com Additional services and information for American Behavioral Scientist can be found at: Email Alerts: http://abs.sagepub.com/cgi/alerts Subscriptions: http://abs.sagepub.com/subscriptions Reprints: http://www.sagepub.com/journalsReprints.nav Permissions: http://www.sagepub.com/journalsPermissions.nav Citations: http://abs.sagepub.com/content/early/2014/03/28/0002764214527092.refs.html >> OnlineFirst Version of Record - Mar 28, 2014 What is This? Downloaded from abs.sagepub.com at ARIZONA STATE UNIV on April 3, 2014 ABSXXX10.1177/0002764214527092American Behavioral ScientistKwon et al. 527092research-article2014 Article American Behavioral Scientist 1 –16 Social Network Influence on © 2014 SAGE Publications Reprints and permissions: Online Behavioral Choices: sagepub.com/journalsPermissions.nav DOI: 10.1177/0002764214527092 Exploring Group Formation abs.sagepub.com on Social Network Sites K. Hazel Kwon1, Michael A. Stefanone2, and George A. Barnett3 Abstract Social media communication is characterized by reduced anonymity and off-to-online social interactions. These characteristics require scholars to revisit social influence mechanisms online. The current study builds on social influence literature to explore social network and gender effects on online behavior. Findings from a quasi- experiment suggest that both network-related variables and gender are significantly associated with online behavior. -

It's Contagious: Rethinking a Metaphor Dialogically
Article Culture & Psychology 2015, Vol. 21(3) 359–379 It’s contagious: ! The Author(s) 2015 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav Rethinking a metaphor DOI: 10.1177/1354067X15601190 dialogically cap.sagepub.com Zachary J Warren Georgetown University, Washington, DC, USA Se´amus A Power University of Chicago, Chicago, IL, USA Abstract ‘‘Contagion’’ appears frequently in peer-reviewed articles and in popular media to explain the spread of ideas, feelings, and behaviors. In the context of social science, however, we argue that this metaphor leads to magical thinking and should be described as a simile, rather than a metaphor. We review literature on ‘‘social contagion’’ using the dialogical paradigm and conclude that peer-reviewed claims tend to correspond with imagined realities from epidemiology rather than social science, including assumptions of passive and linear microbial spread, as well as pathology. We explore case studies on the spread of laughter, riot behavior, and ‘‘mass psychogenic illness,’’ and find that social contagion involves social meanings negotiated at the level of persons and groups that are uncharacteristic to the spread of diseases. Dialogism is presented as a correction to the epidemiological paradigm. Keywords Dialogical theory, contagion theory, psychogenic illness, spread, metaphor, riot behavior, laughter, Bakhtin, Afghanistan, dialogism Introduction In February 2012, the Le Roy School District in Le Roy, New York, reported a ‘‘twitching disease’’ that affected over a dozen teen girls and at least one adult. The New York Department of Health launched an investigation in search of envir- onmental causes, and environmental activist Erin Brochovich sent a team Corresponding author: Se´amus A Power, Department of Comparative Human Development, Social Sciences Research Building, Office 103, 1126 East 59th St, University of Chicago, Chicago, IL 60637, USA. -
NEW SERVICE CENTRES ADDED! Tradelink Extends Its Paper Trade Declaration Service to 22 Fotomax Shops from 10 December 2018
NEW SERVICE CENTRES ADDED! Tradelink extends its Paper Trade Declaration Service to 22 Fotomax shops from 10 December 2018 Tradelink is pleased to announce extension of its Service Centre network at Fotomax to 22 shops with effect from 10 December 2018. Provide convenient paper Conveniently located in business and industry districts around trade declaration service network Hong Kong Island, Kowloon and the New Territories, all these 22 designated Fotomax shops will provide Tradelink paper Trade Declaration service for customers who are unable to submit trade declarations to Government electronically. Customers can submit their paper trade declaration forms at these Tradelink Service Centres and after conversion of the paper trade declarations into electronic format, the electronic declarations will be submitted to the Government through the Tradelink platform. 22 Fotomax Shops Providing Tradelink’s Paper Trade Declaration Service Hong Kong Kowloon Wing Lok Street Cheung Sha Wan Plaza Shop 6, G/F.,Teda Bldg., Wing Lok Street, Unit 104A, Cheung Sha Wan Plaza, Sheung Wan, Hong Kong 833 Cheung Sha Wan Road, Kowloon Hong Kong MTR Station Langham Place MTR Station Concession HOK 71 at Shop No.43 on Level 1, Langham Place, Hong Kong Station (Unpaid Area) 8 Argyle Street, Kowloon Shun Tak Centre Pioneer Centre Shop Unit No. 218, 2/F., Shun Tak Centre, Shop No 250 A & B, 2/F., Pioneer Centre, 200 Connaught Road, Central, Hong Kong 750 Nathan Road, Mongkok, Kowloon. Sun Hung Kai Centre Harbour City Shop No. 109-110 & 110A, Shop 4008, L4, Gateway Arcade, Harbour City, First Floor Sun Hung Kai Centre, Wanchai, Hong Kong 7-23 Canton Road, Tsim Sha Tsui, Kln Hopewell Centre Kowloon Station MTR Shop 311, Hopewell Centre, 183 Queen's Road East, MTR Station Concession KOW 70, Wanchai, Hong Kong Kowloon Station (Unpaid Area), Kowloon FujiFilm Studio 館 - Windsor House Whampoa Garden Shop No. -
The Relationship Between Conformity, Independence
THE RELATIONSHIP BETWEEN CONFORMITY, INDEPENDENCE, ANTICONFORMITY, AND CERTAIN PERSONALITY CHARACTERISTICS APPROVED: Major Professor A/ Minor Processor SVUL~> Dean of the Schoo Education Deancof the Graduate School THE RELATIONSHIP BETWEEN CONFORMITY, INDEPENDENCE, ANTICONFORMITY, AND CERTAIN PERSONALITY CHARACTERISTICS THESIS Presented to the Graduate Council of the North Texas State University in Partial Fulfillment of the Requirements For the Degree of MASTER OF SCIENCE By Patricia S. Mantheiy, B. S. Denton, Texas August, 1969 TABLE OF CONTENTS Page LIST OF TABLES iv Chapter I. INTRODUCTION ....... 1 Related Research Purpose of the Study Statement of the Problem Hypotheses Chapter Bibliography II. METHOD . 42 Subjects Description of Instruments Design Procedure Chapter Bibliography III. ANALYSIS AND DISCUSSION OF RESULTS 54 IV. SUMMARY AND CONCLUSIONS 66 APPENDIX 70 BIBLIOGRAPHY . 75 XXX LIST OF TABLES Table Page I. Means and Standard Deviations of Dependent Variable Scores for Conformers, Independents, and Anticonformers. 54 II. Summary of Analysis of Variance of Conformers Independents, and Anticonformers on Need for Affiliation 55 III. Summary of Analysis of Variance of Conformers Independents and Anticonformers on Dependency Needs 57 IV. Summary of Analysis of Variance of Conformers Independents, and Anticonformers on Overt Anxiety . 58 V. Summary of Analysis of Variance of Conformers Independents, and Anticonformers on Covert Anxiety 60 IV CHAPTER I INTRODUCTION An understanding of conformity and nonconformity is particularly important in these days of social unrest. Most of the research has emphasized understanding the process of conformity, with nonconformity either being ignored or considered the opposite of conformity. This unidimensional approach with conformity on one end and nonconformity on the *« other was conceptualized by Allport (1) in his J curve hypothesis of conformity. -

Behavioral Economics and the SEC
Law & Economics Working Papers Law & Economics Working Papers Archive: 2003-2009 University of Michigan Law School Year 2003 Behavioral Economics and the SEC Stephen Choi∗ Adam C. Pritchardy ∗University of California, Berkeley, [email protected] yUniversity of Michigan Law School, [email protected] This paper is posted at University of Michigan Law School Scholarship Repository. http://repository.law.umich.edu/law econ archive/art12 Choi and Pritchard: UNIVERSITY OF MICHIGAN JOHN M. OLIN CENTER FOR LAW & ECONOMICS BEHAVIORAL ECONOMICS AND THE SEC ADAM C. PRITCHARD WORKING PAPER #03-002 THIS PAPER CAN BE DOW NLOADED WITHOUT CHARGE AT : MICHIGAN JOHN M. OLIN CENTER WEBSITE HTTP://WWW.LAW .UMICH.EDU/CENTERSANDPROGRAMS/OLIN/PAPERS.HTM Published by University of Michigan Law School Scholarship Repository, 2003 1 Law & Economics Working Papers Archive: 2003-2009, Art. 12 [2003] Behavioral Economics and the SEC Behavioral24.doc: 3/20/03 12:22 PM Stephen J. Choi* & A.C. Pritchard** Abstract. Investors face myriad investment alternatives and seemingly limitless information concerning those alternatives. Not surprisingly, many commentators contend that investors frequently fall short of the ideal investor posited by the rational actor model. Investors are plagued with a variety of behavioral biases (such as, among others, the hindsight bias, the availability bias, loss aversion, and overconfidence). Even securities market institutions and intermediaries may suffer from biases, led astray by groupthink and overconfidence. The question remains whether regulators should focus on such biases in formulating policy. An omnipotent regulatory decisionmaker would certainly improve on flawed investor decisionmaking. The alternative we face, however, is a behaviorally-flawed regulator, the Securities and Exchange Commission (SEC). -
Amoy Gardens at the End of the Outbreak, a Total of 329 3.67 Amidst the Outbreak in Prince of Residents Had Been Infected, with 42 Deaths
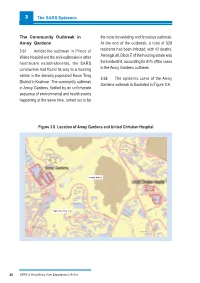
3 The SARS Epidemic The Community Outbreak in the most devastating and ferocious outbreak. Amoy Gardens At the end of the outbreak, a total of 329 3.67 Amidst the outbreak in Prince of residents had been infected, with 42 deaths. Wales Hospital and the mini-outbreaks in other Amongst all, Block E of the housing estate was healthcare establishments, the SARS the hardest hit, accounting for 41% of the cases coronavirus had found its way to a housing in the Amoy Gardens outbreak. estate in the densely populated Kwun Tong 3.68 The epidemic curve of the Amoy District in Kowloon. The community outbreak Gardens outbreak is illustrated in Figure 3.9. in Amoy Gardens, fuelled by an unfortunate sequence of environmental and health events happening at the same time, turned out to be Figure 3.8 Location of Amoy Gardens and United Christian Hospital Jordan Valley Ngau Tau Kok 40 SARS in Hong Kong: from Experience to Action The SARS Epidemic 3 FigureAmoyGardens 3.9 Amoy Gardens Outbreak Outbreak EpidemicEpidemic curve curve by bydate date of ofonset onset 80 70 60 50 40 30 Number of Cases 20 10 0 1/4 2/4 3/4 4/4 5/4 6/4 7/4 8/4 9/4 12/3 13/3 14/3 15/3 16/3 17/3 18/3 19/3 20/3 21/3 22/3 23/3 24/3 25/3 26/3 27/3 28/3 29/3 30/3 31/3 10/4 11/4 12/4 13/4 14/4 15/4 16/4 17/4 18/4 19/4 Date of Onset (2003) The housing estate metres. -

List of Buildings with Confirmed / Probable Cases of COVID-19
List of Buildings With Confirmed / Probable Cases of COVID-19 List of Residential Buildings in Which Confirmed / Probable Cases Have Resided (Note: The buildings will remain on the list for 14 days since the reported date.) Related Confirmed / District Building Name Probable Case(s) Wan Chai Block C, Fontana Garden 5868 Yau Tsim Mong Cam Key Mansion, 495 Shanghai Street 5869 Kowloon City Crystal Mansion 5870 Central & Western Best Western Plus Hotel Hong Kong 5871 Central & Western Tower 1, Kong Chian Tower 5872 Wan Chai 11 Broom Road 5873 Kwai Tsing Wah Shun Court 5874 Kowloon City Sunderland Estate 5875 Islands Headland Hotel 5877 Eastern Block A, Yen Lok Building 5879 Sha Tin Hin Kwai House, Hin Keng Estate 5880 Tai Po Po Sam Pai Village 5881 Sha Tin Mei Chi House, Mei Tin Estate 5882 Tsuen Wan Block 2, Waterside Plaza 5882 Sha Tin Jubilee Court, Jubilee Garden 5883 Kwun Tong Lee Ming House, Shun Lee Estate 5884 Southern Tower 9, Bel-Air On The Peak 5885 Central & Western Block 3, Garden Terrace 5886 Sai Kung Tower 5, The Mediterranean 5887 Sai Kung Tower 5, The Mediterranean 5888 Kowloon City Block 1, Kiu Wang Mansion 5889 Islands Heung Yat House, Yat Tung Estate 5890 Sha Tin Cypress House, Kwong Yuen Estate 5891 Kwai Tsing Block 6, Mayfair Gardens 5892 Eastern Tower 1, Harbour Glory 5893 Sai Kung Kap Pin Long 5894 Wan Chai Hawthorn Garden 5895 Tai Po Villa Castell 5896 Kwun Tong Ping Shun House, Ping Tin Estate 5897 Sai Kung Tak Fu House, Hau Tak Estate 5898 Kwai Tsing Ying Kwai House, Kwai Chung Estate 5899 1 Related Confirmed / -

Restaurant List
Restaurant List (updated 1 July 2020) Island Cafeholic Shop No.23, Ground Floor, Fu Tung Plaza, Fu Tung Estate, 6 Fu Tung Street, Tung Chung First Korean Restaurant Shop 102B, 1/F, Block A, D’Deck, Discovery Bay, Lantau Island Grand Kitchen Shop G10-101, G/F, JoysMark Shopping Centre, Mung Tung Estate, Tung Chung Gyu-Kaku Jinan-Bou Shop 706, 7th Floor, Citygate Outlets, Tung Chung HANNOSUKE (Tung Chung Citygate Outlets) Shop 101A, 1st Floor, Citygate, 18-20 Tat Tung Road, Tung Chung, Lantau Hung Fook Tong Shop No. 32, Ground Floor, Yat Tung Shopping Centre, Yat Tung Estate, 8 Yat Tung Street, Tung Chung Island Café Shop 105A, 1/F, Block A, D’Deck, Discovery Bay, Lantau Island Itamomo Shop No.2, G/F, Ying Tung Shopping Centre, Ying Tung Estate, 1 Ying Tung Road, Lantau Island, Tung Chung KYO WATAMI (Tung Chung Citygate Outlets) Shop B13, B1/F, Citygate Outlets, 20 Tat Tung Road, Tung Chung, Lantau Island Moon Lok Chiu Chow Unit G22, G/F, Citygate, 20 Tat Tung Road, Tung Chung, Lantau Island Mun Tung Café Shop 11, G/F, JoysMark Shopping Centre, Mun Tung Estate, Tung Chung Paradise Dynasty Shop 326A, 3/F, Citygate, 18-20 Tat Tung Road, Tung Chung, Lantau Island Shanghai Breeze Shop 104A, 1/F, Block A, D’Deck, Discovery Bay, Lantau Island The Sixties Restaurant No. 34, Ground Floor, Commercial Centre 2, Yat Tung Estate, 8 Yat Tung Street, Tung Chung 十足風味 Shop N, G/F, Seaview Crescent, Tung Chung Waterfront Road, Tung Chung Kowloon City Yu Mai SHOP 6B G/F, Amazing World, 121 Baker Street, Site 1, Whampoa Garden, Hung Hom CAFÉ ABERDEEN Shop Nos. -

The Human Choice: Individuation, Reason, and Impulse, and Chaos
nebraska symposium on motivation 1969 The Human Choice: WILLIAM J. ARNOLD and DAVID LEVINE, Editors Individuation, Reason, and Order versus Deindividuation, Dalbir Bindra Professor of Psychology- McGill b'liiversily Impulse, and Chaos Professor of Psychology Edward L. Wike PHILIP G. ZIMBARDO University of Kansas Stanjord University Roger W. Black Professor of Psychology University oj South Carolina Omtrol. That’s what current psychology is all about. The use ol powerful schedules of reinforcement, probing neurophysiological techniques, computer simulation, and the new behavior therapies Elliot Aronson Professor of Psychology University of Texas at Austin (among other advances) enable psychologists to manipulate the responses of a wide range of research subjects in order to improve learning and discrimination; to arouse, rechannel, and satisfy Stuart W. Cook Professor of Psyi hology drives; and to redirect abnormal or deviant behavior. It has, in fact, Univernty of Colorado become the all-consuming task of most psychologists to learn how to bring behavior under stimulus control. Philip G. Zimbardo Prolessor of Psychology It is especially impressive to note (in any volume of the Nebraska Stanford University Symposium on Motivation) the relative case with which laboratory researchers can induce motives which have an immediate and often demonstrably pervasive effect on a vast array of response measures. On the other hand, one must reconcile this with the observation ’ that in the “real world” people often.show considerable tolerance university -

Buildings Energy Efficiency Funding Schemes Under the Environment and Conservation Fund
ECPVSC Paper 18/2011-12 For Discussion Buildings Energy Efficiency Funding Schemes under the Environment and Conservation Fund Purpose This paper seeks – (a) Members’ agreement to approve 90 funding applications and not to accept eight funding applications for the Energy Efficiency Projects (EEP) of the Buildings Energy Efficiency Funding Schemes (BEEFS) under the Environment and Conservation Fund (ECF). (b) Members’ support to seek approval from the ECF Committee for three funding applications of values exceeding HK$2.0 million for the EEP of the BEEFS under the ECF. Summary 2. As at 3 January 2012, a total of 220 and 1,329 applications were received for Energy-cum-carbon Audit Projects (ECA) and EEP respectively. Since the Energy Conservation Projects Vetting Sub-committee (ECPVSC) meeting on 17 August 2011, 98 funding applications have been vetted. Out of these 98 applications, 90 funding applications are recommended for approval, six funding applications are recommended not to accept due to inadequate information received for assessment, one funding application is recommended not to accept due to ineligible applicant and one funding application is recommended not to accept due to works commenced before Energy Conservation Projects Vetting Subcommittee (ECPVSC) approval. 3. In addition to the above, 12 funding applications were withdrawn by the applicants which are listed below. Projects withdrawn by the Applicants Project No. Applicant Funding Sought Energy Efficiency Project - The Incorporated Owners of $45,340.00 Cheong Ming Building Cheong Ming Building (Ref. EEP-0236) - 1 - ECPVSC Paper 18/2011-12 For Discussion Project No. Applicant Funding Sought Energy Efficiency Project - Residence Oasis Residential $210,623.00 Residence Oasis Owners Sub-committee (Ref. -

List of Buildings with Confirmed / Probable Cases of COVID-19
List of Buildings With Confirmed / Probable Cases of COVID-19 List of Residential Buildings in Which Confirmed / Probable Cases Have Resided (Note: The buildings will remain on the list for 14 days since the reported date.) Related Confirmed / District Building Name Probable Case(s) Wong Tai Sin Lok Cheung House, Tsz Lok Estate 1779 Kowloon City Yee Man House, Ho Man Tin Estate 1780 Kwun Tong Lung Pak House, Hong Pak Court 1781 Yau Tsim Mong Chong Tak Building 1783 Sha Tin Chung Kwan House, Chung On Estate 1784 Sha Tin Foo Wo House, Wo Che Estate 1785 Wong Tai Sin Oi Ning House, Tsz Oi Court 1786 Kwun Tong Man Wah House, Lok Wah (South) Estate 1787 Kwun Tong Choi Sin House, Choi Fook Estate 1792 Yuen Long Yan Sui House, Tin Yan Estate 1795 Tuen Mun Tip Chui House, Butterfly Estate 1797 Wong Tai Sin Lok Yan House, Tsz Lok Estate 1798 Yau Tsim Mong Yuet Yuen Building 1799 Kwun Tong Yin Chee Lau, Kwun Tong Garden Estate 1802 Wong Tai Sin Kam Wan House, Choi Hung Estate 1804 Kwun Tong Tak Shing House, Tak Tin Estate 1805 Tai Po Block 1, Phase 1, Tai Po Centre 1806 Sha Tin Shing Chung House, Mei Chung Court 1807 Kowloon City Tak Cheung House, Tak Long Estate 1808 Kwun Tong Kai Lok House, Kai Yip Estate 1809 Yau Tsim Mong Sheraton Hong Kong Hotel & Towers 1811 Sai Kung Ma Yau Tong 1812 Sham Shui Po Mei Sang House, Shek Kip Mei Estate 1813 Kwai Tsing Block 2, Greenview Villa 1814 Kwai Tsing Block 2, Greenview Villa 1815 Sham Shui Po Lotus House, So Uk Estate 1817 Kwai Tsing Shek Cheung House, Shek Lei (II) Estate 1818 Wong Tai Sin Ching On House,