Rural Hospitals Subject to Training
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Connected Members (Query-Based Exchange) As of 9/1/19
Connected Members (Query-Based Exchange) As of 9/1/19 State Georgia Department of Behavioral Health and Development Disabilities Agencies (DBHDD) – Shares patient discharge records Georgia Department of Juvenile Justice (DJJ) – Views patient health information for youth in their care Georgia Department of Public Health (DPH) – Bi-directional submission gateway for immunization data (GRITS), eLab and Syndromic Surveillance reporting; contributes immunization information Georgia Division of Family and Children Services (DFCS) – Views patient health information for youth in their care Georgia Medicaid/Department of Community Health (DCH) – Contributes Medicaid claims (health, dental, pharmacy) information. Medicaid providers using GAMMIS can view patient health information. Care Care Management Organizations facilitate care coordination for Medicare and Medicaid patients, Management including PeachCare for Kids(r), Georgia Families(r) and Planning for Healthy Babies (r) (P4HB(r)) Organizations Amerigroup – shares care plans and views patient health information CareSource – shares care plans and views patient health information Peach State – views patient health information WellCare – views patient health information Health Shares patient health information from their connected providers Systems Children’s Healthcare of Atlanta (CHOA) – Georgia’s largest children’s hospital Emory Healthcare – Georgia’s largest academic hospital Grady Health System – Georgia’s largest public hospital Gwinnett Health System – Serves one of the -

2019 HEART Annual Report
Engaging Enhancing Elevating Georgia rural patient taxpayers hospitals care 2019 HEART Annual Report Now, more than ever, Georgians — Take HEART! INSIDE THE REPORT A Letter from Georgia Governor Brian P. Kemp . .3 A Letter from Georgia Lt. Governor Geoff Duncan ...............4 Georgia HEART Hospitals ..................................5 HEART Contribution Results.................................6 Important Tax Developments ...............................7 Hospital Testimonials....................................8-9 2019 HEART Tax Credit Survey Results .......................10 Business Community Involvement ...........................11 THE HEART TEAM AVERY KATE ROSALYN LISA ALLISON PARKER SAYLOR MERRICK KELLY SAXBY RICE Director of Director of Executive Director of Director of Marketing & Stakeholder Director Operations Accounting Communications Engagement & Finance DIANNE MEGHAN JIM SHERRI NELSON- MEYER KELLY O’CONNOR WILLIAMS Client Services Accounting General Accounting Manager Manager Counsel Associate 2 Dear Supporters of the Georgia HEART Rural Hospital Tax Credit Program, A LETTER FROM As Georgians address the health challenges arising from the COVID-19 GEORGIA virus, I cannot overstate the key role played by our rural hospitals and GOVERNOR courageous service providers fighting on the front lines for those impacted by this pandemic. BRIAN P. KEMP Since 2017, many of you have donated to one or more of the Georgia HEART rural hospitals. As a result of your generosity, these hospitals were better able to provide critical care that, absent your thoughtful contributions, would not have been available to many of those infected by the coronavirus. Truly, these were life-saving contributions. As Georgia lawmakers consider the long-term effects of the COVID-19 pandemic and the steps that must be taken to promote related healthcare solutions in rural Georgia, it is reassuring to know that so many concerned citizens have embraced the Georgia HEART program. -
November 28, 2018 – December 4, 2018 Requests for Extended Implementation/Performance Period
Use the links below for easy navigation Letters of Intent Letters of Intent - Expired Letters of Intent – Fall Batching New CON Applications CON Applications/Projects Withdrawn Pending/Complete Applications Pending Review/Incomplete CON Applications Office of Health Planning Recently Approved CON Applications Recently Denied CON Applications Appealed CON Projects Letters of Determination Requests for Miscellaneous Letters of Determination Appealed Determinations DET Review LNR Conversion CERTIFICATE OF NEED Requests for LNR for Diagnostic or Therapeutic Equipment Requests for LNR for Establishment of Physician-Owned Ambulatory Surgery Facilities Appealed LNRs November 28, 2018 – December 4, 2018 Requests for Extended Implementation/Performance Period Batching Notifications - Fall Need Projection Analyses Georgia Department of Community Health New Batching Review Office of Health Planning Summer Cycle Fall Cycle 2 Peachtree Street 5th Floor Non-Filed or Incomplete Surveys Atlanta, Georgia 30303-3159 Indigent-Charity Shortfalls (404) 656-0409 (404) 656-0442 Fax CON Filing Requirements (effective July 18, 2017) www.dch.georgia.gov Contact Information Verification of Lawful Presence within U.S. Periodic Reporting Requirements CON Thresholds Open Record Request Form Web Links Certificate of Need Appeal Panel www.GaMap2Care.info Letters of Intent LOI2018083 Doctors Hospital of Augusta Acquire a Fixed-Based MRI to Replace Existing Mobile MRI Received: 11/15/2018 Application must be submitted on: 12/17/2018 Site: 3651 Wheeler Road, Augusta, GA -
FY 2020 Proposed Rule Impact File.Xlsx
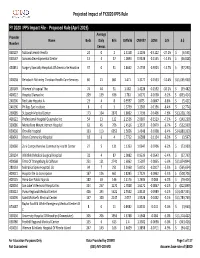
Projected Impact of FY2020 IPPS Rule FY 2020 IPPS Impact File ‐ Proposed Rule (April 2019) Average Provider Name Beds Daily Bills CMIV36 CMIV37 ∆CMI ∆ % ∆ $ Number Census 060107 National Jewish Health 24 0 2 1.5158 1.1036 ‐0.4122 ‐27.2%$ (6,595) 050547 Sonoma Developmental Center 13 4 37 1.0893 0.9338 ‐0.1555 ‐14.3% $ (46,028) 450831 Surgery Specialty Hospitals Of America Se Houston 37 0 31 2.8662 2.4739 ‐0.3923 ‐13.7%$ (97,290) 320038 Rehoboth Mckinley Christian Health Care Services 60 21 861 1.471 1.3177 ‐0.1533 ‐10.4%$ (1,055,930) 150149 Women's Hospital The 74 44 31 1.582 1.4228 ‐0.1592 ‐10.1%$ (39,482) 400022 Hospital Damas Inc 209 139 636 1.781 1.6172 ‐0.1638 ‐9.2%$ (833,414) 240206 Red Lake Hospital A 23 4 8 0.9597 0.875 ‐0.0847 ‐8.8%$ (5,421) 240196 Phillips Eye Institute 8 0 3 1.3739 1.2583 ‐0.1156 ‐8.4%$ (2,774) 260085 St Joseph Medical Center 173 104 2870 1.8602 1.7196 ‐0.1406 ‐7.6%$ (3,228,176) 400122 Professional Hospital Guaynabo Inc 54 13 122 2.1536 2.0007 ‐0.1529 ‐7.1%$ (149,230) 330086 Montefiore Mount Vernon Hospital 63 45 706 1.4516 1.3537 ‐0.0979 ‐6.7%$ (552,939) 050030 Oroville Hospital 133 113 6052 1.5656 1.4648 ‐0.1008 ‐6.4%$ (4,880,333) 460043 Orem Community Hospital 18 6 4 1.7712 1.6588 ‐0.1124 ‐6.3%$ (3,597) 320060 Zuni Comprehensive Community Health Center 27 5 131 1.1353 1.0647 ‐0.0706 ‐6.2%$ (73,989) 250134 Whitfield Medical Surgical Hospital 32 4 87 1.0082 0.9539 ‐0.0543 ‐5.4%$ (37,793) 420068 Trmc Of Orangeburg & Calhoun 251 121 2741 1.6062 1.5207 ‐0.0855 ‐5.3%$ (1,874,844) 280133 Nebraska Spine Hospital, -

HS&R Q3 Report, 2016
MEDICAIDDEPARTMENT CARE MANAGEMENT OF ORGANIZATIONS COMMUNITY ACT HEALTH COMPLIANCEGEORGIA MONITORING FAMILIES MEDICAID CARE MANAGEMENT ORGANIZATIONS ACT COMPLIANCE MONITORING ANALYSES OF HOSPITAL STATISTICAL AND REIMBURSEMENT (HS&R) REPORT SUBMISSIONS QUARTER 3: JULY THROUGH SEPTEMBER 2016 JANUARY 6, 2017 TABLE OF CONTENTS Project Background .......................................................................................................................... 3 Objective........................................................................................................................................... 4 Methodology .................................................................................................................................... 5 Assumptions and Limitations ........................................................................................................... 6 Analytical Findings ............................................................................................................................ 7 Summary........................................................................................................................................... 8 Exhibits ........................................................................................................................................... 10 Page 2 PROJECT BACKGROUND The Medicaid Care Management Organizations Act (the “Act”) requires the Care Management Organizations (CMOs) to provide a Hospital Statistical and Reimbursement (HS&R) report within -

GA ARES Hospital Emergency Operations Plan
Georgia Amateur Radio Emergency Service HOSPITAL EMERGENCY OPERATIONS PLAN for Hospital Emergency Radio Operators Approved 07-20-2017 Updated 7-6-2021 1 Table of Contents 1. Definitions 2. Organization 3. Responsibilities 4. Membership & Training 5. Activation 6. Utilization 7. Supported Agencies 8. Communication Modes 9. Net Operations 10. Appendix A: Recommended Hospital Equipment 11. Appendix B: Personal Equipment 12. Appendix C: Primary Frequencies 13. Appendix D: Regional Hospitals by Region 14. Appendix E: Healthcare Essential Elements of Information (EEI) 15.Appendix F: Required Items for Hospital Radio Rooms 16.Appendix G: Radio Room Standard Operating Procedures 2 Definitions 1. Amateur Radio Emergency Service— The group of licensed amateur radio operators who provide emergency communications as part of the Amateur Radio Relay League (ARRL) Field Organization. 2. Hospital Operators— The group of emergency communicators trained in the National Incident Command System (NIMS) who operate under the authority of the Georgia Section Amateur Radio Emergency Service (GAARES). 3. Section Emergency Coordinator (SEC)— The appointed leader of all ARES operations within the State of Georgia. 4. Assistant Section Emergency Coordinator (ASEC)— The appointed leader of each designated GAARES Branch. Hospital operations falls under the oversight of the ASEC for the Department of Human Resources/Public Health. 5. District Emergency Coordinator (DEC)— The appointed leader who coordinates with multiple local ARES groups. There is a DEC for each of the nine (9) districts under GAARES. 6. Emergency Coordinator (EC)— The appointed leader of the ARES group at the local or county level. 7. Regional Coordinating Hospital (RCH)— In each of the 14 regions throughout the State the largest hospital is designated as the RCH. -
Manager and Executive Compensation in Hospitals and Health Systems Survey Report
2019 Manager and Executive Compensation in Hospitals and Health Systems Survey Report Survey data effective January 1, 2019 © 2019 SullivanCotter, Inc. All rights reserved. 200 W. Madison Street, Suite 2450 Chicago, IL 60606-3416 2019 MANAGER AND EXECUTIVE COMPENSATION IN HOSPITALS AND HEALTH SYSTEMS SURVEY REPORT Survey data effective January 1, 2019 LICENSE AGREEMENT LICENSE AGREEMENT By accessing or downloading the Survey Report files online or by opening the packaging for this Survey Report, you agree to the terms of this License Agreement (this “Agreement”). If you do not agree to these terms and have not yet accessed or downloaded the Survey Report files or opened the packaging for this Survey Report, you may cancel your online purchase or download at this time or you may return this Survey Report to SullivanCotter, Inc. for a full refund within thirty (30) days of receipt, but you may not access or download the Survey Report files or open the packaging for, or otherwise use, this Survey Report. Accessing or downloading the Survey Report files or opening the packaging, or otherwise using, this Survey Report binds you to this Agreement. This Agreement is entered into by and between SullivanCotter, Inc. ("SullivanCotter") and the purchaser or participant of this Survey Report (the “Licensee”). In consideration of the mutual covenants in this Agreement, SullivanCotter and the Licensee agree as follows: Grant of License. This Survey Report contains the aggregation of compensation data and other data provided to SullivanCotter by its survey participants, statistics, tables, reports, research, aggregations, calculations, data analysis, formulas, summaries, content, text and other information and materials provided to the Licensee by SullivanCotter through any other means, whether digital or hard copy, related thereto (the “Aggregated Data”). -

Health-Careers-Manual-2016.Pdf
30417 Health Career Booklet Cvr_r1.indd 1 3/15/16 12:42 PM Table of Contents Acknowledgments Foothills Area Health Education Center (AHEC) is pleased to present the 10th edition of Health Careers in Georgia. This publication is produced through the partnership of the Georgia Statewide AHEC Network consisting of six centers with support from the Georgia legislature and the US Department of Title Page ........................................................................3 Health and Human Services Health Resources and Services Administration. Many community and academic partners contributed time, expertise, and resources in producing this resource for the current and future healthcare workforce. Some content, photos, and/or layout ideas were provided by Pam What is AHEC? ....................................................................4 Reynolds and SOWEGA AHEC, staff from other Georgia AHECs, Jeremy Whigham Design, the Georgia Department of Labor, Phyllis Johnson with the Georgia Department of Education, Ralph Morrison and the Georgia Health Information & Management Association Board of Directors, the American AHEC Spotlight ....................................................................5 Society for Cytotechnology, Sheri Porter with American Academy of Family Physicians News, and Dru Nadler Photography. We appreciate all of the Healthcare Trends ...............................................................6-7 expert readers listed below for reviewing and editing the content of each career page thereby enabling us to produce -

Episiotomy Rates from the 2015 Leapfrog Hospital Survey
Episiotomy Rates from the 2015 Leapfrog Hospital Survey Results reflect submissions received by December 31, 2015 Hospital City State Rate Performance Alaska Regional Hospital Anchorage AK 7.00% Substantial Progress Bartlett Regional Hospital Juneau AK Declined to Respond Central Peninsula General Hospital Soldotna AK Declined to Respond Fairbanks Memorial Hospital Fairbanks AK 3.30% Fully Meets Standard Mat‐Su Regional Medical Center Palmer AK Declined to Respond Providence Alaska Medical Center Anchorage AK 6.60% Substantial Progress Andalusia Regional Hospital Andalusia AL 10.10% Some Progress Athens‐Limestone Hospital Athens AL Declined to Respond Atmore Community Hospital Atmore AL Declined to Respond Baptist Medical Center East Montgomery AL Declined to Respond Baptist Medical Center South Montgomery AL Declined to Respond Bibb Medical Center Centreville AL Declined to Respond Brookwood Medical Center Birmingham AL 21.50% Willing to Report Bryan W. Whitfield Memorial Hospital Demopolis AL Declined to Respond Bullock County Hospital Union Springs AL Declined to Respond Cherokee Medical Center Centre AL Declined to Respond Citizens Baptist Medical Center Talladega AL Declined to Respond Clay County Hospital Ashland AL Declined to Respond Community Hospital of Tallassee Tallassee AL Declined to Respond Coosa Valley Medical Center Sylacauga AL Declined to Respond Crenshaw Community Hospital Luverne AL Declined to Respond Crestwood Medical Center Huntsville AL Declined to Respond Cullman Regional Medical Center Cullman AL Declined to -

2017 Home Health Survey Part A
2017 Home Health Survey Part A : General Information 1. Identification UID:HHA053 Facility Name: Encompass Home Health of Georgia County: Muscogee Street Address: 6001 River Road, Suite 220 City: Columbus Zip: 31904 Mailing Address: 6688 N Central Expressway, Suite 1300 Mailing City: Dallas Mailing Zip: 75206 Medicaid Provider? Check the box to the right if the agency is a medicaid provider If you indicated yes above, please report the medicaid number below. 000696407A Medicare Provider? Check the box to the right if the agency is a medicare provider If you indicated yes above, please report the medicare number below. 11-7306 2. Report Period Report Data for the full twelve month period, January 1,2017 - December 31, 2017 (365 days). Do not use a different report period. Check the box to the right if your facility was not operational for the entire year. If your facility was not operational for the entire year, provide the dates the facility was operational. Part B : Survey Contact Information Person authorized to respond to inquiries about the responses to this survey. Contact Name: Tracey Kruse Contact Title: Chief Operating Officer Page 1 Phone: 214-239-6500 Fax: 214-239-6581 E-mail: [email protected] Part C : Ownership, Operation and Management 1. Ownership, Operation and Management As of the last day of the report period, indicate the operation/management status of the facility and provide the effective date. Using the drop-down menus, select the organization type. If the category is not applicable, the form requires you only to enter Not Applicable in the legal name field. -

2019 Ambetter and Bluecross Hospital List.Xlsx
Ambetter and BlueCross Hospital List Most doctors that practice at an in‐network hospital will also be in‐network. One exception we know is Piedmont Atlanta Hospital. Piedmont Hospital is in the Ambetter netwok, but very few Piedmont Doctors are. It's always best to check with the insurance company's Search Tool or with the Provider directly. Hospital Name City Zip Ambetter BlueCross Emory University Hospital Atlanta 30322 X Emory University Hospital Midtown Atlanta 30308 X Emory Saint Joseph Atlanta 30342 X Emory Johns Creek Duluth 30097 X Emory Wesley Woods Hospital Atlanta 30329 X Northside Hospital Atlanta 30342 X Northside Hospital Cherokee Canton 30115 X Northside Hospital Forsyth Cumming 30041 X WellStar Atlanta Medical Center Atlanta 30312 X X WellStar Windy Hill Marietta 30067 X X WellStar Cobb Austell 30106 X X WellStar North Fulton Hospital Roswell 30076 X X WellStar Douglas Douglasville 30134 X Wellstar Kennestone Hospital Marietta 30060 X X WellStar Paulding Hiram 30141 X X WellStar Spalding Griffin 30224 X X WellStar Sylvan Grove Jackson 30233 X X WellStar Atlanta Medical Center South East Point 30344 X X Wellstar West Georgia Medical Center Lagrange 30240 X X DeKalb Medical Center Decatur 30033 X X Dekalb Medical Center at Hillendale Lithonia 30058 X X Shepherd Center Atlanta 30305 X X Gwinnett Medical Center Duluth Lawrenceville 30096 X X Gwinnett Medical Center Lawrenceville 30046 X X Childrens Healthcare of Atlanta Scottish Rite Atlanta 30342 X X Children Healthcare of Atl Hughes Spaulding Atlanta 30303 X X Childrens -

March 20, 2018 Implementation/Performance Period
Use the links below for easy navigation Letters of Intent Letters of Intent - Expired New CON Applications Withdrawn CON Applications Pending Review/Complete CON Applications Pending Review/Incomplete CON Applications Recently Approved CON Applications Office of Health Planning Recently Denied CON Applications Appealed CON Projects Letters of Determination Requests for Miscellaneous Letters of Determination Appealed Determinations LNR Conversion Requests for LNR for Diagnostic or CERTIFICATE OF NEED Therapeutic Equipment Requests for LNR for Establishment of Physician-Owned Ambulatory Surgery Facilities Appealed LNRs Requests for Extended March 14, 2018 – March 20, 2018 Implementation/Performance Period Batching Notifications - Winter Need Projection Analyses Georgia Department of Community Health Office of Health Planning New Batching Review Fall Cycle 2 Peachtree Street Winter Cycle 5th Floor Atlanta, Georgia 30303-3159 Non-Filed or Incomplete Surveys Indigent-Charity Shortfalls (404) 656-0409 (404) 656-0442 Fax CON Filing Requirements www.dch.georgia.gov (effective July 18, 2017) Contact Information Verification of Lawful Presence within U.S. Periodic Reporting Requirements CON Thresholds Open Record Request Form Web Links www.GaMap2Care.info Certificate of Need Appeal Panel Letters of Intent LOI2018013 Union General Affiliated Services, LLC Develop Outpatient Imaging Center Received: 2/21/2018 Application must be submitted on: 3/23/2018 Site: Deep South Farm Road, Blairsville, GA 30512 (Union County) Estimated Cost: $6,500,000 LOI2018014