PDL)/Non-Preferred Drug List (NPDL
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Endothelin System and Therapeutic Application of Endothelin Receptor
xperim ACCESS Freely available online & E en OPEN l ta a l ic P in h l a C r m f o a c l a o n l o r g u y o J Journal of ISSN: 2161-1459 Clinical & Experimental Pharmacology Research Article Endothelin System and Therapeutic Application of Endothelin Receptor Antagonists Abebe Basazn Mekuria, Zemene Demelash Kifle*, Mohammedbrhan Abdelwuhab Department of Pharmacology, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia ABSTRACT Endothelin is a 21 amino acid molecule endogenous potent vasoconstrictor peptide. Endothelin is synthesized in vascular endothelial and smooth muscle cells, as well as in neural, renal, pulmonic, and inflammatory cells. It acts through a seven transmembrane endothelin receptor A (ETA) and endothelin receptor B (ETB) receptors belongs to G protein-coupled rhodopsin-type receptor superfamily. This peptide involved in pathogenesis of cardiovascular disorder like (heart failure, arterial hypertension, myocardial infraction and atherosclerosis), renal failure, pulmonary arterial hypertension and it also involved in pathogenesis of cancer. Potentially endothelin receptor antagonist helps the treatment of the above disorder. Currently, there are a lot of trails both per-clinical and clinical on endothelin antagonist for various cardiovascular, pulmonary and cancer disorder. Some are approved by FAD for the treatment. These agents are including both selective and non-selective endothelin receptor antagonist (ETA/B). Currently, Bosentan, Ambrisentan, and Macitentan approved -

2020 Prior Authorization Criteria
2020 PRIOR AUTHORIZATION CRITERIA TABLE OF CONTENTS abiraterone tablet ...................................................................................................................... 217 ABRAXANE .............................................................................................................................. 131 ACTIMMUNE .............................................................................................................................. 14 ADASUVE ................................................................................................................................... 27 ADEMPAS ................................................................................................................................ 197 AFINITOR ................................................................................................................................. 217 AFINITOR DISPERZ ................................................................................................................. 217 AIMOVIG ..................................................................................................................................... 15 ALECENSA ............................................................................................................................... 217 ALIMTA ..................................................................................................................................... 131 ALIQOPA ................................................................................................................................. -

Resistance Mechanisms to Targeted Therapies in ROS1+ and ALK+ Non−Small Cell Lung Cancer
Published OnlineFirst April 10, 2018; DOI: 10.1158/1078-0432.CCR-17-2452 Cancer Therapy: Clinical Clinical Cancer Research Resistance Mechanisms to Targeted Therapies in ROS1þ and ALKþ Non–small Cell Lung Cancer Caroline E. McCoach1, Anh T. Le2, Katherine Gowan3, Kenneth Jones3, Laura Schubert2, Andrea Doak2, Adriana Estrada-Bernal2, Kurtis D. Davies4, Daniel T. Merrick4, Paul A. BunnJr2, W. Tom Purcell2, Rafal Dziadziuszko5, Marileila Varella-Garcia2, Dara L. Aisner4, D. Ross Camidge2, and Robert C. Doebele2 Abstract Purpose: Despite initial benefit from tyrosine kinase inhibitors and b-catenin mutations and HER2-mediated bypass signaling as þ (TKIs), patients with advanced non–smallcelllungcancer(NSCLC) non-ROS1–dominant resistance mechanisms. In the ALK þ þ harboring ALK (ALK )andROS1 (ROS1 ) gene fusions ultimately cohort, we identified a novel NRG1 gene fusion, a RET fusion, progress. Here, we report on the potential resistance mechanisms 2 EGFR, and 3 KRAS mutations, as well as mutations in IDH1, þ þ in a series of patients with ALK and ROS1 NSCLC progressing RIT1, NOTCH, and NF1. In addition, we identified CNV in on different types and/or lines of ROS1/ALK–targeted therapy. multiple proto-oncogenes genes including PDGFRA, KIT, KDR, Experimental Design: We used a combination of next-gener- GNAS, K/HRAS, RET, NTRK1, MAP2K1, and others. ation sequencing (NGS), multiplex mutation assay, direct DNA Conclusions: We identified a putative TKI resistance mech- þ sequencing, RT-PCR, and FISH to identify fusion variants/partners anism in six of 12 (50%) ROS1 patients and 37 of 43 (86%) þ and copy-number gain (CNG), kinase domain mutations (KDM), ALK patients. -

S41598-018-33190-8.Pdf
www.nature.com/scientificreports OPEN Ankyrin Repeat Domain 1 Overexpression is Associated with Common Resistance to Afatinib and Received: 20 February 2018 Accepted: 25 September 2018 Osimertinib in EGFR-mutant Lung Published: xx xx xxxx Cancer Akiko Takahashi1, Masahiro Seike1, Mika Chiba1, Satoshi Takahashi1, Shinji Nakamichi1, Masaru Matsumoto1, Susumu Takeuchi1, Yuji Minegishi1, Rintaro Noro1, Shinobu Kunugi2, Kaoru Kubota1 & Akihiko Gemma1 Overcoming acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) is critical in combating EGFR-mutant non-small cell lung cancer (NSCLC). We tried to construct a novel therapeutic strategy to conquer the resistance to second-and third-generation EGFR-TKIs in EGFR-positive NSCLC patients. We established afatinib- and osimertinib-resistant lung adenocarcinoma cell lines. Exome sequencing, cDNA array and miRNA microarray were performed using the established cell lines to discover novel therapeutic targets associated with the resistance to second-and third-generation EGFR-TKIs. We found that ANKRD1 which is associated with the epithelial- mesenchymal transition (EMT) phenomenon and anti-apoptosis, was overexpressed in the second-and third-generation EGFR-TKIs-resistant cells at the mRNA and protein expression levels. When ANKRD1 was silenced in the EGFR-TKIs-resistant cell lines, afatinib and osimertinib could induce apoptosis of the cell lines. Imatinib could inhibit ANKRD1 expression, resulting in restoration of the sensitivity to afatinib and osimertinib of EGFR-TKI-resistant cells. In EGFR-mutant NSCLC patients, ANKRD1 was overexpressed in the tumor after the failure of EGFR-TKI therapy, especially after long-duration EGFR- TKI treatments. ANKRD1 overexpression which was associated with EMT features and anti-apoptosis, was commonly involved in resistance to second-and third-generation EGFR-TKIs. -

Adrenal Disorders
Adrenal Disorders Dual-release Hydrocortisone in Addison’s Disease— A Review of the Literature Roberta Giordano, MD,1 Federica Guaraldi, MD,2 Rita Berardelli, MD,2 Ioannis Karamouzis, MD,2 Valentina D’Angelo, MD,2 Clizia Zichi, MD,2 Silvia Grottoli, MD,2 Ezio Ghigo, PhD2 and Emanuela Arvat, PhD3 1. Department of Clinical and Biological Sciences; 2. Division of Endocrinology, Diabetology and Metabolism, Department of Medical Sciences; 3. Division of Oncological Endocrinology, Department of Medical Sciences, University of Turin, Turin, Italy Abstract In patients with adrenal insufficiency, glucocorticoids (GCs) are insufficiently secreted and GC replacement is essential for health and, indeed, life. Despite GC-replacement therapy, patients with adrenal insufficiency have a greater cardiovascular risk than the general population, and suffer from impaired health-related quality of life. Although the aim of the replacement GC therapy is to reproduce as much as possible the physiologic pattern of cortisol secretion by the normal adrenal gland, the pharmacokinetics of available oral immediate-release hydrocortisone or cortisone make it impossible to fully mimic the cortisol rhythm. Therefore, there is an unmet clinical need for the development of novel pharmaceutical preparations of hydrocortisone, in order to guarantee a more physiologic serum cortisol concentration time-profile, and to improve the long-term outcome in patients under GC substitution therapy. Keywords Addison’s disease, glucocorticoids, hydrocortisone, Plenadren®, limits, advantages Disclosure: The authors have no conflicts of interest to declare. Received: June 28, 2013 Accepted: August 9, 2013 Citation: US Endocrinology 2013;9(2):177–80 DOI: 10.17925/USE.2013.09.02.177 Correspondence: Roberta Giordano, MD, Division of Endocrinology, Diabetology and Metabolism, Department of Medical Sciences, Azienda Ospedaliera Città della Salute e della Scienza di Torino, C so Dogliotti 14, 10126 Turin, Italy. -
Pricing Sheet
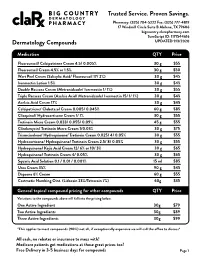
Trusted Service. Proven Savings. Pharmacy: (325) 704-5222 Fax: (325) 777-4819 17 Windmill Circle Suite B Abilene, TX 79606 bigcountry.clarxpharmacy.com SureScript ID: 1171544616 Dermatology Compounds UPDATED 9/3/2020 Medication QTY Price Fluorouracil/ Calcipotriene Cream 4.5/ 0.005% 30 g $55 Fluorouracil Cream 4.5% or 1.5% 30 g $50 Wart Peel Cream (Salicylic Acid/ Fluorouracil 17/ 2%) 30 g $45 Ivermectin Lotion 1.5% 30 g $45 Double Rosacea Cream (Metronidazole/ Ivermectin 1/ 1%) 30 g $55 Triple Rosacea Cream (Azelaic Acid/ Metronidazole/ Ivermectin 15/ 1/ 1%) 30 g $45 Azelaic Acid Cream 17% 30 g $45 Calcipotriene/ Clobetasol Cream 0.005/ 0.045% 60 g $85 Clioquinol/ Hydrocortisone Cream 1/ 1% 30 g $55 Tretinoin Micro Cream 0.033/ 0.055/ 0.09% 45 g $55 Clindamycin/ Tretinoin Micro Cream 1/0.03% 30 g $75 Triamcinolone/ Hydroquinone/ Tretinoin Cream 0.025/ 4/ 0.05% 30 g $55 Hydrocortisone/ Hydroquinone/ Tretinoin Cream 2.5/ 8/ 0.05% 30 g $55 Hydroquinone/ Kojic Acid Cream 12/ 6% or 10/ 3% 30 g $65 Hydroquinone/ Tretinoin Cream 4/ 0.05% 30 g $65 Squaric Acid Solution 0.1 / 0.01 / 0.001% 15 ml $85 Urea Cream 35% 90 g $45 Dapsone 6% Cream 60 g $55 Costmetic Numbing Oint. (Lidocain 23%/Tetracain 7%) 60g $35 General topical compound pricing for other compounds QTY Price Variations to the compounds above will fall into the pricing below. One Active Ingredient 30g $79 Two Active Ingredients 30g $89 Three Active Ingredients 30g $99 *This applies to most compounds (90%) not all, if exceptionally expensive we will call the office to discuss* All cash, no rebates or insurance to mess with! Medicare patients get medications at these great prices too! Free Delivery in 3-5 business days for compounds Page 1 Trusted Service. -

Pharmacokinetics, Pharmacodynamics and Drug
pharmaceutics Review Pharmacokinetics, Pharmacodynamics and Drug–Drug Interactions of New Anti-Migraine Drugs—Lasmiditan, Gepants, and Calcitonin-Gene-Related Peptide (CGRP) Receptor Monoclonal Antibodies Danuta Szkutnik-Fiedler Department of Clinical Pharmacy and Biopharmacy, Pozna´nUniversity of Medical Sciences, Sw.´ Marii Magdaleny 14 St., 61-861 Pozna´n,Poland; [email protected] Received: 28 October 2020; Accepted: 30 November 2020; Published: 3 December 2020 Abstract: In the last few years, there have been significant advances in migraine management and prevention. Lasmiditan, ubrogepant, rimegepant and monoclonal antibodies (erenumab, fremanezumab, galcanezumab, and eptinezumab) are new drugs that were launched on the US pharmaceutical market; some of them also in Europe. This publication reviews the available worldwide references on the safety of these anti-migraine drugs with a focus on the possible drug–drug (DDI) or drug–food interactions. As is known, bioavailability of a drug and, hence, its pharmacological efficacy depend on its pharmacokinetics and pharmacodynamics, which may be altered by drug interactions. This paper discusses the interactions of gepants and lasmiditan with, i.a., serotonergic drugs, CYP3A4 inhibitors, and inducers or breast cancer resistant protein (BCRP) and P-glycoprotein (P-gp) inhibitors. In the case of monoclonal antibodies, the issue of pharmacodynamic interactions related to the modulation of the immune system functions was addressed. It also focuses on the effect of monoclonal antibodies on expression of class Fc gamma receptors (FcγR). Keywords: migraine; lasmiditan; gepants; monoclonal antibodies; drug–drug interactions 1. Introduction Migraine is a chronic neurological disorder characterized by a repetitive, usually unilateral, pulsating headache with attacks typically lasting from 4 to 72 h. -
Xifaxan® (Rifaximin)
Wednesday, October 14, 2015 4 p.m. Oklahoma Health Care Authority 4345 N. Lincoln Blvd. Oklahoma City, OK 73105 The University of Oklahoma Health Sciences Center COLLEGE OF PHARMACY PHARMACY MANAGEMENT CONSULTANTS MEMORANDUM TO: Drug Utilization Review Board Members FROM: Bethany Holderread, Pharm.D. SUBJECT: Packet Contents for Board Meeting – October 14, 2015 DATE: October 1, 2015 NOTE: The DUR Board will meet at 4:00 p.m. The meeting will be held at 4345 N Lincoln Blvd. Enclosed are the following items related to the October meeting. Material is arranged in order of the agenda. Call to Order Public Comment Forum Action Item – Approval of DUR Board Meeting Minutes – Appendix A Action Item – Vote on 2016 Meeting Dates – Appendix B Update on Medication Coverage Authorization Unit/Bowel Preparation Medication Post-Educational Mailing – Appendix C Action Item – Vote to Prior Authorize Tykerb® (Lapatinib), Halaven® (Eribulin), Ixempra® (Ixabepilone), Kadcyla® (Ado-Trastuzumab), Afinitor® (Everolimus), & Perjeta® (Pertuzumab) – Appendix D Action Item – Vote to Prior Authorize Orkambi™ (Lumacaftor/Ivacaftor) – Appendix E Action Item – Vote to Prior Authorize Savaysa® (Edoxaban) – Appendix F Action Item – Vote to Prior Authorize Epanova® (Omega-3-Carboxylic Acids), Praluent® (Alirocumab), & Repatha™ (Evolocumab) – Appendix G Annual Review of Constipation and Diarrhea Medications and 30-Day Notice to Prior Authorize Movantik™ (Naloxegol), Viberzi™ (Eluxadoline), & Xifaxan® (Rifaximin) – Appendix H 30-Day Notice to Prior Authorize Daraprim® (Pyrimethamine) – Appendix I Annual Review of Allergy Immunotherapies and 30-Day Notice to Prior Authorize Oralair® (Sweet Vernal, Orchard, Perennial Rye, Timothy, & Kentucky Blue Grass Mixed Pollens Allergen Extract) – Appendix J Annual Review of Non-Steroidal Anti-Inflammatory Drugs and 30-Day Notice to Prior Authorize Dyloject™ (Diclofenac Sodium) – Appendix K ORI-4403 • P.O. -

M2021: Pharmacogenetic Testing
Pharmacogenetic Testing Policy Number: AHS – M2021 – Pharmacogenetic Prior Policy Name and Number, as applicable: Testing • M2021 – Cytochrome P450 Initial Presentation Date: 06/16/2021 Revision Date: N/A I. Policy Description Pharmacogenetics is defined as the study of variability in drug response due to heredity (Nebert, 1999). Cytochrome (CYP) P450 enzymes are a class of enzymes essential in the synthesis and breakdown metabolism of various molecules and chemicals. Found primarily in the liver, these enzymes are also essential for the metabolism of many medications. CYP P450 are essential to produce many biochemical building blocks, such as cholesterol, fatty acids, and bile acids. Additional cytochrome P450 are involved in the metabolism of drugs, carcinogens, and internal substances, such as toxins formed within cells. Mutations in CYP P450 genes can result in the inability to properly metabolize medications and other substances, leading to increased levels of toxic substances in the body. Approximately 58 CYP genes are in humans (Bains, 2013; Tantisira & Weiss, 2019). Thiopurine methyltransferase (TPMT) is an enzyme that methylates azathioprine, mercaptopurine and thioguanine into active thioguanine nucleotide metabolites. Azathioprine and mercaptopurine are used for treatment of nonmalignant immunologic disorders; mercaptopurine is used for treatment of lymphoid malignancies; and thioguanine is used for treatment of myeloid leukemias (Relling et al., 2011). Dihydropyrimidine dehydrogenase (DPD), encoded by the gene DPYD, is a rate-limiting enzyme responsible for fluoropyrimidine catabolism. The fluoropyrimidines (5-fluorouracil and capecitabine) are drugs used in the treatment of solid tumors, such as colorectal, breast, and aerodigestive tract tumors (Amstutz et al., 2018). A variety of cell surface proteins, such as antigen-presenting molecules and other proteins, are encoded by the human leukocyte antigen genes (HLAs). -

Endothelin-Receptor Antagonists Are Proapoptotic and Antiproliferative in Human Colon Cancer Cells
British Journal of Cancer (2003) 88, 788 – 795 & 2003 Cancer Research UK All rights reserved 0007 – 0920/03 $25.00 www.bjcancer.com Endothelin-receptor antagonists are proapoptotic and antiproliferative in human colon cancer cells 1 1 ,1 L Peduto Eberl , R Bovey and L Juillerat-Jeanneret* 1 University Institute of Pathology, CHUV, University of Lausanne, Bugnon 25, CH1011 Lausanne, Switzerland Endothelin (ET)-1 can act as an autocrine/paracrine growth factor or an antiapoptotic factor in human cancers. To study the role of ET-1 in human colon cancer, proliferation and apoptosis of colon carcinoma cells was investigated using human HT-29 and SW480 colon carcinoma cells. ET-1 was secreted by these cells. Treatment of cells with bosentan, a dual ETA/B-receptor antagonist, decreased cell number. Inhibition of DNA synthesis by bosentan was observed only in the presence of serum. Exogenously added ET-1 did not increase DNA synthesis in serum-deprived cells. SW480 cells were sensitive and HT-29 cells were resistant to FasL- induced apoptosis. Bosentan sensitised resistant HT-29 cells to FasL-induced, caspase-mediated apoptosis, but not to TNF-a-induced apoptosis. Bosentan and/or FasLigand (FasL) did not modulate the expression of caspase-8 or FLIP. Bosentan sensitisation to À13 À10 À9 À7 apoptosis was reversed by low concentrations (10 –10 M), but not by high concentrations (10 –10 M) of ET-1. These results suggest that the binding of ET-1 to high-affinity sites inhibits FasL-induced apoptosis, while the binding of either ET-1 or receptor antagonists to low-affinity sites promotes FasL-induced apoptosis. -
VITAL Jan 2019 Follow-Up
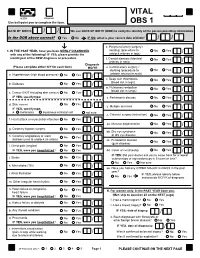
VITAL 6308 Request Use ball-point pen to complete the form. OBS 1 DATE OF BIRTH: / / We use DATE OF BIRTH (DOB) to verify the identity of the person providing information. Is the DOB above correct? Yes No IF NO, what is your correct date of birth? / / s. Peripheral artery surgery / 1. IN THE PAST YEAR, have you been NEWLY DIAGNOSED stenting (procedure to No Yes / with any of the following? IF YES, please provide the unblock arteries in legs) month/year of the NEW diagnosis or procedure. t. Carotid stenosis (blocked No Yes Answer NO/YES on each line. arteries in neck) / Diagnosis (Please complete either N/Y for each item) MO/YR u. Carotid artery surgery / stenting (procedure to No Yes / a. Hypertension (high blood pressure) No Yes / unblock arteries in neck) v. Deep vein thrombosis No Yes (blood clot in legs) / b. Diabetes No Yes / w. Pulmonary embolism No Yes (blood clot in lungs) / c. Cancer (NOT including skin cancer) No Yes / IF YES, specify type: _______________________ x. Parkinson's disease No Yes / d. Skin cancer No Yes / y. Multiple sclerosis No Yes IF YES, specify type: / e. melanoma squamous or basal cell not sure z. Cataract surgery (extraction) No Yes / f. Heart attack or myocardial infarction No Yes / aa. Macular degeneration No Yes / g. Coronary bypass surgery No Yes / bb. Dry eye syndrome No Yes or dry eye disease / h. Coronary angioplasty or stent No Yes (balloon used to unblock an artery) / cc. Periodontal disease No Yes (gum disease) / i. Chest pain (angina) No Yes / IF YES, were you hospitalized? No Yes dd. -
Frequently Asked Questions for Addison Patients
FREQUENTLY ASKED QUESTIONS FOR ADDISON PATIENTS TABLE OF CONTENT (Place your cursor over the subject line, hold down the Control Button and Click your mouse. To get back to the Table of Content, hold down the Control Button and press the Home key) ADDISONIAN CRISIS / EMERGENCY ADDISONS AND OTHER DISORDERS ADDISONS AND OTHER MEDICATIONS ADRENALINE BLOOD PRESSURE COMMON COLD/FLU/OTHER ILLNESS CORTISOL DAY CURVE CORTISOL MEDICATION CRAMPS DIABETES DIAGNOSING ADDISONS EXERCISE / SPORTS FATIGUE FLORINEF / SALT / SODIUM HERBAL / VITAMIN SUPPLEMENTS HYPERPIGMENTATION IMMUNIZATION MENOPAUSE, PREGNANCY, HORMONE REPLACEMENT, BIRTH CONTROL, HYSTERECTOMY MISCELLANEOUS OSTEOPOROSIS SECONDARY ADDISON’S SHIFT WORK SLEEP 1 STRESS DOSING SURGICAL, MEDICAL, DENTAL PROCEDURES THYROID TRAVEL WEIGHT GAIN 2 ADDISONIAN CRISIS / EMERGENCY How do you know when to call an ambulance? If you are careful, you should not have to call an ambulance. If someone with adrenal insufficiency has gastrointestinal problems and is unable to keep down their cortisol or other glucocorticoid for more than 24 hrs, they should be taken to an emergency department so they can be given intravenous solucortef and saline. It is not appropriate to wait until they are so ill that they cannot be taken to the hospital by a family member. If the individual is unable to retain anything by mouth and is very ill, or if they have had a sudden stress such as a fall or an infection, then it would be necessary for them to go by ambulance as soon as possible. It is important that you should have an emergency kit at home and that someone in the household knows how to use it.