Pathophysiological Mechanisms and Functional Hearing Consequences of Auditory Neuropathy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cranial Nerve VIII
Cranial Nerve VIII Color Code Important (The Vestibulo-Cochlear Nerve) Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives At the end of the lecture, the students should be able to: ✓ List the nuclei related to vestibular and cochlear nerves in the brain stem. ✓ Describe the type and site of each nucleus. ✓ Describe the vestibular pathways and its main connections. ✓ Describe the auditory pathway and its main connections. Due to the difference of arrangement of the lecture between the girls and boys slides we will stick to the girls slides then summarize the pathway according to the boys slides. Ponto-medullary Sulcus (cerebello- pontine angle) Recall: both cranial nerves 8 and 7 emerge from the ventral surface of the brainstem at the ponto- medullary sulcus (cerebello-pontine angle) Brain – Ventral Surface Vestibulo-Cochlear (VIII) 8th Cranial Nerve o Type: Special sensory (SSA) o Conveys impulses from inner ear to nervous system. o Components: • Vestibular part: conveys impulses associated with body posture ,balance and coordination of head & eye movements. • Cochlear part: conveys impulses associated with hearing. o Vestibular & cochlear parts leave the ventral surface* of brain stem through the pontomedullary sulcus ‘at cerebellopontine angle*’ (lateral to facial nerve), run laterally in posterior cranial fossa and enter the internal acoustic meatus along with 7th (facial) nerve. *see the previous slide Auditory Pathway Only on the girls’ slides 04:14 Characteristics: o It is a multisynaptic pathway o There are several locations between medulla and the thalamus where axons may synapse and not all the fibers behave in the same manner. -

Anatomy of the Ear ANATOMY & Glossary of Terms
Anatomy of the Ear ANATOMY & Glossary of Terms By Vestibular Disorders Association HEARING & ANATOMY BALANCE The human inner ear contains two divisions: the hearing (auditory) The human ear contains component—the cochlea, and a balance (vestibular) component—the two components: auditory peripheral vestibular system. Peripheral in this context refers to (cochlea) & balance a system that is outside of the central nervous system (brain and (vestibular). brainstem). The peripheral vestibular system sends information to the brain and brainstem. The vestibular system in each ear consists of a complex series of passageways and chambers within the bony skull. Within these ARTICLE passageways are tubes (semicircular canals), and sacs (a utricle and saccule), filled with a fluid called endolymph. Around the outside of the tubes and sacs is a different fluid called perilymph. Both of these fluids are of precise chemical compositions, and they are different. The mechanism that regulates the amount and composition of these fluids is 04 important to the proper functioning of the inner ear. Each of the semicircular canals is located in a different spatial plane. They are located at right angles to each other and to those in the ear on the opposite side of the head. At the base of each canal is a swelling DID THIS ARTICLE (ampulla) and within each ampulla is a sensory receptor (cupula). HELP YOU? MOVEMENT AND BALANCE SUPPORT VEDA @ VESTIBULAR.ORG With head movement in the plane or angle in which a canal is positioned, the endo-lymphatic fluid within that canal, because of inertia, lags behind. When this fluid lags behind, the sensory receptor within the canal is bent. -

Acoustically Responsive Fibers in the Vestibular Nerve of the Cat
The Journal of Neuroscience, October 1994, 74(10): 6056-6070 Acoustically Responsive Fibers in the Vestibular Nerve of the Cat Michael P. McCue1v2*a and John J. Guinan, Jr.r.2.3-4 ‘Eaton-Peabody Laboratory of Auditory Physiology, Department of Otolaryngology, Massachusetts Eye and Ear Infirmary, Boston, Massachusetts 02114, 2Harvard-MIT Division of Health Science and Technology and Research Laboratory of Electronics, and 3Department of Electrical Engineering and Computer Science, Massachusetts Institute of Technology, Cambridge, Massachusetts 02139, and 4Department of Otology and Laryngology, Harvard Medical School, Boston, Massachusetts 02115 Recordings were made from single afferent fibers in the and levels within the normal range of human hearing. We inferior vestibular nerve, which innervates the saccule and suggest a number of auditory roles that these fibers may posterior semicircular canal. A substantial portion of the fi- play in the everyday life of mammals. bers with irregular background activity increased their firing [Key words: saccule, otoliths, auditory system, mamma- in response to moderately intense clicks and tones. lian sound reception, middle-ear muscles, cochlear nucleus] In responsive fibers, acoustic clicks evoked action poten- tials with minimum latencies of I 1 .O msec. Fibers fell into The vertebrate inner ear contains several senseorgans involved two classes, with the shortest latency either to condensation in the maintenance of equilibrium and the detection of vibra- clicks (PUSH fibers) or to rarefaction clicks (PULL fibers). tion. The precise sensory role assumedby homologous organs Low-frequency (800 Hz) tone bursts at moderately high sound varies among species.For example, the sacculeis thought to act levels (>80 dB SPL) caused synchronization of spikes to asa linear accelerometerin mammals(Fernindez and Goldberg, preferred phases of the tone cycle. -

Anatomic Moment
Anatomic Moment Hearing, I: The Cochlea David L. Daniels, Joel D. Swartz, H. Ric Harnsberger, John L. Ulmer, Katherine A. Shaffer, and Leighton Mark The purpose of the ear is to transform me- cochlear recess, which lies on the medial wall of chanical energy (sound) into electric energy. the vestibule (Fig 3). As these sound waves The external ear collects and directs the sound. enter the perilymph of the scala vestibuli, they The middle ear converts the sound to fluid mo- are transmitted through the vestibular mem- tion. The inner ear, specifically the cochlea, brane into the endolymph of the cochlear duct, transforms fluid motion into electric energy. causing displacement of the basilar membrane, The cochlea is a coiled structure consisting of which stimulates the hair cell receptors of the two and three quarter turns (Figs 1 and 2). If it organ of Corti (Figs 4–7) (4, 5). It is the move- were elongated, the cochlea would be approxi- ment of hair cells that generates the electric mately 30 mm in length. The fluid-filled spaces potentials that are converted into action poten- of the cochlea are comprised of three parallel tials in the auditory nerve fibers. The basilar canals: an outer scala vestibuli (ascending spi- membrane varies in width and tension from ral), an inner scala tympani (descending spi- base to apex. As a result, different portions of ral), and the central cochlear duct (scala media) the membrane respond to different auditory fre- (1–7). The scala vestibuli and scala tympani quencies (2, 5). These perilymphatic waves are contain perilymph, a substance similar in com- transmitted via the apex of the cochlea (helico- position to cerebrospinal fluid. -

Processing in the Cochlear Nucleus
Processing in The Cochlear Nucleus Alan R. Palmer Medical Research Council Institute of Hearing Research University Park Nottingham NG7 2RD, UK The Auditory Nervous System Cortex Cortex MGB Medial Geniculate Body Excitatory GABAergic IC Inferior Colliculus Glycinergic DNLL Nuclei of the Lateral Lemniscus Lateral Lemniscus Cochlear Nucleus DCN PVCN MSO Lateral Superior Olive AVCN Medial Superior Olive Cochlea MNTB Medial Nucleus of the Trapezoid Body Superior Olive The cochlear nucleus is the site of termination of fibres of the auditory nerve Cochlear Nucleus Auditory Nerve Cochlea 1 Frequency Tonotopicity Basilar membrane Inner hair cell Auditory nerve Fibre To the brain Each auditory-nerve fibre responds only to a narrow range of frequencies Tuning curve Action potential Evans 1975 2 Palmer and Evans 1975 There are many overlapping single-fibre tuning curves in the auditory nerve Audiogram Palmer and Evans 1975 Tonotopic Organisation Lorente - 1933 3 Tonotopic Organisation Base Anterior Cochlea Characteristic Basilar Membrane Frequency Hair Cells Auditory Nerve Apex Cochlear Nucleus Spiral Ganglion Posterior Tonotopic projection of auditory-nerve fibers into the cochlear nucleus Ryugo and Parks, 2003 The cochlear nucleus: the first auditory nucleus in the CNS Best frequency Position along electrode track (mm) Evans 1975 4 stellate (DCN) Inhibitory Synapse Excitatory Synapse DAS to inferior colliculus cartwheel fusiform SUPERIOR OLIVARY giant COMPLEX INFERIOR COLLICULUS granule vertical vertical OCB AANN to CN & IC via TB golgi DORSAL -
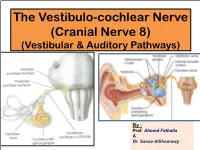
The Vestibulo-Cochlear Nerve (Cranial Nerve 8) (Vestibular & Auditory Pathways)
The Vestibulo-cochlear Nerve (Cranial Nerve 8) (Vestibular & Auditory Pathways) By : Prof. Ahmed Fathalla & Dr. Sanaa AlShaarawy OBJECTIVES At the end of the lecture, the students should be able to: qList the nuclei related to vestibular and cochlear nerves in the brain stem. qDescribe the type and site of each nucleus. qDescribe the vestibular pathways and its main connections. qDescribe the auditory pathway and its main connections. BRAIN – VENTRAL SURFACE Ponto-medullary Sulcus (cerebello- pontine angle) Vestibulo-Cochlear Nerve • Type: Special sensory (SSA) • Conveys impulses from inner ear to nervous system. • Components: § Vestibular part: conveys impulses associated with body posture ,balance and coordination of head & eye movements. § Cochlear part: conveys impulses associated with hearing. • Vestibular & cochlear parts leave the ventral surface of brain stem through the pontomedullary sulcus ‘at crebellopontine angle’ (lateral to facial nerve), run laterally in posterior cranial fossa and enter the internal acoustic meatus along with 7th nerve. Vestibular Nerve • The cell bodies (1st order neurons) are Vestibular nuclei belong to located in the vestibular ganglion special somatic afferent within the internal auditory meatus. column in brain stem. • The Peripheral processes (vestibular nerve fibers) make dendritic contact with hair cells of the membranous labyrinth (inner ear). 2 • The central processes (form the vestibular nerve) ‘’Efferent Fibres’’ : 1. Mostly end up in the lateral, medial, inferior and superior 1 vestibular nuclei (2nd order neurons) of the rostral medulla, located beneath the lateral part of the floor of 4th ventricle 2. Some fibers go to the cerebellum through the inferior cerebellar peduncle • Other Efferents from the vestibular nuclei project to other regions for the maintenance of balance, conscious awareness of vestibular stimulation , co-ordination of head & eye movements and control the posture. -

Cranial Nerve Disorders: Clinical Manifestations and Topographyଝ
Radiología. 2019;61(2):99---123 www.elsevier.es/rx UPDATE IN RADIOLOGY Cranial nerve disorders: Clinical manifestations and topographyଝ a,∗ a b c M. Jorquera Moya , S. Merino Menéndez , J. Porta Etessam , J. Escribano Vera , a M. Yus Fuertes a Sección de Neurorradiología, Hospital Clínico San Carlos, Madrid, Spain b Servicio de Neurología, Hospital Clínico San Carlos, Madrid, Spain c Neurorradiología, Hospital Ruber Internacional, Madrid, Spain Received 17 November 2017; accepted 27 September 2018 KEYWORDS Abstract The detection of pathological conditions related to the twelve cranial pairs rep- Cranial pairs; resents a significant challenge for both clinicians and radiologists; imaging techniques are Cranial nerves; fundamental for the management of many patients with these conditions. In addition to knowl- Cranial neuropathies; edge about the anatomy and pathological entities that can potentially affect the cranial pairs, Neuralgia; the imaging evaluation of patients with possible cranial pair disorders requires specific exami- Cranial nerve palsy nation protocols, acquisition techniques, and image processing. This article provides a review of the most common symptoms and syndromes related with the cranial pairs that might require imaging tests, together with a brief overview of the anatomy, the most common underlying processes, and the most appropriate imaging tests for different indications. © 2018 SERAM. Published by Elsevier Espana,˜ S.L.U. All rights reserved. PALABRAS CLAVE Sintomatología derivada de los pares craneales: Clínica y topografía Pares craneales; Resumen La detección de la patología relacionada con los doce pares craneales representa Nervios craneales; un importante desafío, tanto para los clínicos como para los radiólogos. Las técnicas de imagen Neuropatía de pares craneales; son fundamentales para el manejo de muchos de los pacientes. -

The Vestibulocochlear Nerve (VIII)
Diagnostic and Interventional Imaging (2013) 94, 1043—1050 . CONTINUING EDUCATION PROGRAM: FOCUS . The vestibulocochlear nerve (VIII) a,∗ b a F. Benoudiba , F. Toulgoat , J.-L. Sarrazin a Department of neuroradiology, Kremlin-Bicêtre university hospital, 78, rue du Général-Leclerc, 94275 Le Kremlin-Bicêtre, France b Diagnostic and interventional neuroradiology, Laennec hospital, Nantes university hospitals, boulevard Jacques-Monod, Saint-Herblain, 44093 Nantes cedex 1, France KEYWORDS Abstract The vestibulocochlear nerve (8th cranial nerve) is a sensory nerve. It is made up of Cranial nerves; two nerves, the cochlear, which transmits sound and the vestibular which controls balance. It is Pathology; an intracranial nerve which runs from the sensory receptors in the internal ear to the brain stem Vestibulocochlear nuclei and finally to the auditory areas: the post-central gyrus and superior temporal auditory nerve (VIII) cortex. The most common lesions responsible for damage to VIII are vestibular Schwannomas. This report reviews the anatomy and various investigations of the nerve. © 2013 Published by Elsevier Masson SAS on behalf of the Éditions françaises de radiologie. The cochlear nerve Review of anatomy [1] The cochlear nerve has a peripheral sensory origin and follows a centripetal path. It ori- ginates in the cochlear membrane sensory canal, forming the spiral organ (the organ of Corti) and lies on the basilar membrane (Fig. 1). The neuronal fibers of the protoneu- ron connect to the ciliated cells on the spiral lamina (Fig. 2). The axons are grouped together along the axis of the cochlea (modiolus), forming the cochlear nerve which then enters the internal auditory meatus (IAM). Within the internal auditory meatus, the nerve joins the vestibular nerve to form the vestibulocochlear nerve which crosses the cere- bellopontine angle (Figs. -

Balance and Equilibrium, II: the Retrovestibular Neural Pathway
Anatomic Moment Balance and Equilibrium, II: The Retrovestibular Neural Pathway Joel D. Swartz, David L. Daniels, H. Ric Harnsberger, John L. Ulmer, Steven Harvey, Katherine A. Shaffer, and Leighton Mark In this article, we will consider the anatomy of nerve within this quadrant (Fig 3). This ana- the retrovestibular pathways: the superior and tomic arrangement allows for surgical denerva- inferior vestibular nerves and related intraaxial tion of the posterior semicircular canal (singular structures. The reader is encouraged to review neurectomy), a procedure indicated for many previous installments if questions arise regard- patients with chronic benign positional vertigo ing terminology. (cupulolithiasis) (4). The internal auditory canal (IAC) is highly The vestibular (Scarpa’s) ganglion is situated variable in size, shape, and orientation (1). As a within the IAC and is responsible for mediation general rule, there is symmetry between the of afferent and efferent impulses of the saccule, right and left canals in the same person. The utricle, and all three semicircular canals (3). As IAC is defined as having a porus (meatus) me- such, the vestibular nerve has five terminal dially along the petrous surface and a fundus branches. Four vestibular nuclei are located in laterally abutting the labyrinth. At the fundus, a the brain stem at the pontomedullary junction transverse (falciform) crest separates the canal medial to the cochlear nuclei at the level of the into superior and inferior compartments. Fur- floor of the fourth ventricle (2, 5) (Fig 6). Fibers thermore, a vertical crest (Bill’s bar) subdivides of the vestibular nerves synapse in these nuclei. the superior compartment into anterior and Activity within the brain stem is quite complex posterior portions (Figs 1 and 2). -

Pathway of a Sound Wave
Pathway of a Sound Wave 1. The sound waves arrive at the pinna (auricle), the only visible part of the ear. 2. Once the sound waves have passed the pinna, they move into the auditory canal (external acoustic meatus) before hitting the tympanic membrane (eardrum). 3. Once the sound waves reach the tympanic membrane, it begins to vibrate and they enter into the middle ear. 4. The vibrations are transmitted further into the ear via three bones (ossicles): malleus (hammer), incus (anvil), and the stapes (stirrup). These three bones form a bridge from the tympanic membrane to the oval window. 5. Once sound passes through the oval window, it enters into the cochlea in the inner ear. 6. Hair cells in the organ of Corti (within the cochlea) are stimulated which in turn stimulates the cochlear branch of the vestibulocochlear nerve. 7. The cochlear nerve then transmits electrical impulses to the auditory region of the brain in the temporal lobe. Pathway of a Sound Wave 1. The sound waves arrive at the pinna (auricle), the only visible part of the ear. 2. Once the sound waves have passed the pinna, they move into the auditory canal (external acoustic meatus) before hitting the tympanic membrane (eardrum). 3. Once the sound waves reach the tympanic membrane, it begins to vibrate and they enter into the middle ear. 4. The vibrations are transmitted further into the ear via three bones (ossicles): malleus (hammer), incus (anvil), and the stapes (stirrup). These three bones form a bridge from the tympanic membrane to the oval window. -
Identification and Management of Infants and Young Children with Consensus
Guidelines for Identification and Management of Infants and Young Children with Auditory Neuropathy Spectrum Disorder Guidelines Development Conference at NHS 2008, Como, Italy More Hearing. Slim Design. WaterResistant. Now available: Naída, designed for moderately-severe to profound hearing loss. Restoration of high frequency audibility and uncompromised performance. Get the power to change life, now for all degrees of significant hearing loss. www.naida.phonak.com Guidelines for Identification and Management of Infants and Young Children with Auditory Neuropathy Spectrum Disorder Co-Chairs Deborah Hayes, PhD Co-Chair, Bill Daniels Center for Children’s Hearing Kelley Family/Schlessman Family Scottish Rite Masons Chair in Childhood Language Disorders The Children’s Hospital – Colorado Yvonne S. Sininger, PhD Professor, Head and Neck Surgery David Geffen School of Medicine University of California, Los Angeles Los Angeles, California Editor Jerry Northern, PhD Professor Emeritus University of Colorado School of Medicine Colorado Hearing Foundation Denver, Colorado Conference and Editorial Assistant Valerie Hernandez Program Assistant Bill Daniels Center for Children’s Hearing The Children’s Hospital – Colorado This monograph is sponsored in part by a generous grant from the Kelley Family/Schlessman Family Scottish Rite Masons Chair in Childhood Language Disorders The Children’s Hospital – Colorado ©2008 The Children’s Hospital – Colorado, Aurora, Colorado USA. All Rights Reserved. The ONLYONLY handheld OAE-Tympanometry combination system... Audiologists Physicians Birth-to-3 Programs School Health TM BENEFITS • Sequenced protocols permit a full test battery with the press of only one button. • OAE and tympanometry are completed in as little as 20 seconds. • Easy operation for every level of tester. -

Cochlear Anatomy, Function and Pathology II
Cochlear anatomy, function and pathology II Professor Dave Furness Keele University [email protected] Aims and objectives of this lecture • Focus (2) on the biophysics of the cochlea, the dual roles of hair cells, and their innervation: – Cochlear frequency selectivity – The cochlear amplifier – Neurotransmission and innervation of the hair cells – Spiral ganglion and the structure of the auditory nerve Frequency analysis in the cochlea • Sound sets up a travelling wave along the basilar membrane • The peak of motion determines the frequency selectivity (tuning) of the cochlea at that point • The peak moves further along as frequency gets lower Active mechanisms • Basilar membrane motion in a dead cochlea does not account for the very sharp tuning of a live mammalian cochlea • Measurements by Rhode and others showed that an active intact cochlea had very sharp tuning, by looking at basilar membrane motion and auditory nerve fibre tuning • Cochlear sensitivity and frequency selectivity are highly dependent on this active process The gain and tuning of the cochlear amplifier at the basilar membrane From: Robles and Ruggero, Physiological Reviews 81, No. 3, 2001 The gain and tuning of the cochlear amplifier at the basilar membrane Why do we use decibels? The ear is capable of hearing a very large range of sounds: the ratio of the sound pressure that causes permanent damage from short exposure to the limit that (undamaged) ears can hear is more than a million. To deal with such a range, logarithmic units are useful: the log of a million is 6, so this ratio represents a difference of 120 dB.