The Effects on Riding Performance Using Active Vs Passive Recovery During a Simulated Motocross Race
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Outlast Newsletter
Hello – With the first quarter of 2013 underway, we have many positive developments in the works to strengthen our brand positioning and continue to bring more products to market that feature the proactive benefits of our technology. We've rolled out our new brand identity that includes a refreshed logo. The new design pays respect to the strength and success of the Outlast brand as the global leader in phase change materials (PCMs) for the past 22 years, while encapsulating our relentless push for technological innovation in our field. To support this, our R&D team has introduced the world's first-ever polyester fiberfill with Outlast® technology - a development ideally suited for comforters, sleeping bags, jackets, etc. Outlast® Polyfill brings polyester fiber into the 21st century. Additionally, our partnerships continue to expand on the apparel front with a new women's boot to be introduced later this year from Papillon International. We're also working with Spanish company LS2 on new motorcycle racing helmets, as well as Ripzone™ on their line of Trilogy™ snowboarding jackets that will be lined with Outlast® technology for the 2013/2014 season. Our continued success, as always, is due in large part to our partnerships and relationships around the globe and everyone involved in our operations that contribute to expanded product offerings and applications. Warmest wishes to all of you in the New Year. Sincerely, Michael Coors CEO, Outlast Technologies Papillon International Introduces Women's Riding Boot - Fall Preview! We've partnered with Papillon International to bring to market women's riding boots for the fall 2013 season, featuring Outlast® technology in the ankle and foot lining, and the sock footbed. -
MDC Physical Activity
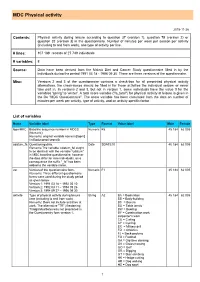
MDC Physical activity 2015-11-26 Contents: Physical activity during leisure according to question 37 (version 1), question 75 (version 2) or question 32 (version 3) in the questionnaire. Number of minutes per week per season per activity (including to and from work), one type of activity per line. # lines: 107 189 records of 27 749 individuals # variables: 8 Source: Data have been derived from the Malmö Diet and Cancer Study questionnaire filled in by the individuals during the period 1991 03 18 - 1996 09 30. There are three versions of the questionnaire. Misc: Versions 2 and 3 of the questionnaire contains a check-box for all preprinted physical activity alternatives, the check-boxes should be filled in for those activities the individual seldom or never take part in. In versions 2 and 3, but not in version 1, some individuals have the value 0 for the variables 'spring' to 'winter'. A total score variable ("fa_total") for physical activity at leisure is given in the file "MDC Questionnaire". The score variable has been calculated from the data on number of minutes per week per activity, type of activity, and an activity specific factor List of variables Name Variable label Type Format Value label Male Female lopnrMKC Baseline sequence number in MDCS Numeric F5 45 184 62 005 (Numeric). Remarks: original variable name is [lopnr] (in Bodycomp [seqno]). udatum_fa Questioning date. Date SDATE10 45 184 62 005 Remarks:The variable 'udatum_fa' ought to be identical with the variable "udatum" in MDC baseline questionnaire, however the date differ for nine individuals, as a consequence the suffix "_fa" has been added to the variable name. -

Motor Racing Questionnaire
Motor Racing Questionnaire Name (first, middle initial, last) Date of birth (d/m/y) Policy no. ________________ - __ Advisor’s name Advisor’s no. 1 | Automobile racing Types(s) of racing engaged in: Auto crash: २ T-bone, Rollover, Dive Bomber, etc. Kart २ Enduro, Sprint २ Demolition Derby २ Experimental, others २ Grand Touring (including Trans-Am Midget/Sprint car: २ 1/4, 1/2 and IROC) २ 3/4 Full (Outlaw) २ Record attempts २ IMSA GT Drag Racer: २ Top Fuel Dragster, Funny Car, Prostock (PRO) २ Indy Light Car २ Other or Amateur २ Vintage or other sports car racing २ Off-Road (Baja 500, Mexican 1000, etc.) Rally: २ Professional २ Stock car (Specify type) २ Other or amateur Record Attempts २ Sedan Racing (BMW, Audi, etc.) Jet Car: २ Exhibition २ Time trials २ Record attempts २ Pleasure or Income Sports Cars: २ Can-Am Professional Training २ Yes No Other _________________ २ Formula car (Specify type): Make(s), model(s) and engine size(s) of vehicles(s): _____________________________________________________________________________ ______________________________________________________________________________________________________________________________2 | Motorcycle racing Types(s) of racing engaged in: २ Drag Racer: २ Top Fuel २ Road racing (Grandprix or Productions): २ Stunt riding, acrobats, daredevils, २ Modified २ Street or stock Engine size: _____________ cc time trials or speed record attempts Make and model: _____________ _____________________________ Professional Training २ Yes २ No २ Pleasure or २ Motorcross: २ Income Engine -

Motocross Isa Team Sport...Sure Most Consider Motorcycle Racing An
Motocross IS a team sport ....Sure most consider motorcycle racing an Individual action. Yes, you can do It alone, but when we look at the big picture we clearly see there are so many elements that are Involved In the sport Many of us on the outside do not realize the behind scenes preparation The work that It takes ... From sign up to trophies .... An enormous amount of organization IS Involved April 17, 1978, a man by the name of Jerry Sharp opened a European style motocross track in Springfield, Missoun. The name of the track was Possum Hollow In dedication to their adventure In finding the ground At this time there were only three motocross tracks In the state of Mlssoun, Cycle World USA In SI. lOUIS, lake City In the Kansas City area, and Possum Hollow In Spnngfleld. For the next three years Jerry and wife, Ellie, promoted and organ- Ized motocross races at the Ozark Empire Fair Grounds and Possum Hollow It s said that Jerry was fifteen to twenty years ahead of his time In the arenacross style of racing. In 1981 Jerry started a senes that Included two tracks, Gene lewIs' lake City and his very own Possum Hollow. Tied to the GNC the events were qualifiers, at that time, for Ponca City and lake Whitney In Texas. As the years flew by Jerry continued his full time job With Gibson Greeting Cards travel- ing the states of Missoun and northern Arkansas puttmg In fifty to sixty hour weeks and still bUilding and promoting the senes. -

Racetrack Safety Guidelines
RACETRACK SAFETY GUIDELINES Published by CIRSA 3665 Cherry Creek North Drive Denver, Colorado 80209 800.228.7136 FAX 303.757.8950 www.cirsa.org © CIRSA 2007 Table of Contents I. Introduction 2 II. Location 2 III. Operation, Maintenance & Inspection 3 IV. Event Operation 4 V. Claims Reporting & Investigation 4 VI. Budgeting 4 VII. Release of Liability & Indemnifi cation Agreement 6 VIII. Audit & Inspection Sample Checklists 9 * This publication is meant for informational purposed only, and as with all CIRSA publications, is intended only to assist CIRSA members in their own loss control activities. It is not intended to replace programs and activities, or provide specifi c legal, technical, or other advice. * 1 Introduction Automobile racing in America can be traced back to 1895, when six racers competed in a 54 mile race from Chicago to Evanston, Illinois and back for a $2,000 prize. Through snowy condi- tions, Frank Duryea crossed the fi nish line fi rst with a time of 10 hours and 23 minutes. The love of speed and competition has catapulted the popularity of racing as well as the types of racing to new highs annually. Autos and motorcycles are raced in a gamut of categories and the availability of local facilities draws many participants of all skill levels. Municipalities may own a racing facility, be it a drag strip, road course, or an old airport runway con- verted to a race track in efforts to bring tourism and revenue to the local area. Owning and operating a facility for this high risk activity is normally outside the scope of standard municipal operations, such as water treatment or playground maintenance. -

Brembo Confirms Motorsport Leadership with Wins in 2020
BREMBO CONFIRMS MOTORSPORT LEADERSHIP WITH WINS IN 2020 The competition record of the company is enriched with over 42 titles won in 2020, with the result of 500 world championships won in the main Motorsport categories Brembo, leader in high performance braking systems, confirms its technological supremacy in Motorsport through the many championships won with teams and manufacturers in 2020. With 42 world titles won, including drivers, manufacturers and team titles the Brembo group, Motorsport supplier for over 45 years, reaches the milestone of *500 world titles obtained in various two and four-wheel competitions. In Formula 1 all of the 17 Grand Prix races in the current season have been won by cars equipped with Brembo components. The Bergamo-based company can boast victories in 442 out of 785 Grand Prix that have taken place since 1975, the year of the debut in Formula 1, until today, for a total of 26 world drivers’ championships and 30 world constructors’ championship won with the top teams. Brembo’s dominance also continues in MotoGP, to which are added new wins in Moto2 and Moto3 (also with Marchesini). Over 500 victories in the premier class (500 class and MotoGP): for the fifth consecutive season Brembo supplied all the teams. Specifically, the 27 riders who raced at least one race in MotoGP this year relied on the high levels of performance and safety guaranteed by Brembo components: brake calipers, carbon discs and pads, brake pumps and clutch pumps. Starting from 1978 to 2001, it’s possible to count the first 185 GPs won by bikes with Brembo brakes in the 500 class. -

2017 Rules for Professional Motocross Competition
2017 RULES FOR PROFESSIONAL MOTOCROSS COMPETITION Introduction This book contains the rules and technical requirements governing all events that make up the AMA Pro Racing Motocross Championship, and is designed to provide the necessary information to assist licensed riders in the preparation of motorcycles for motocross competitions sanctioned by AMA Pro Racing. As a general rule, unless optional equipment or modification is specifically permitted by this Rulebook, it is prohibited. The intent of a specific rule will override a competitor’s interpretation of that rule. The intent of a rule will be determined by AMA Pro Racing officials. If any equipment rule is unclear to the competitor, the competitor is advised to obtain written approval prior to making any modifications. Requests for rule clarifications or interpretations must be submitted in writing by riders and teams to AMA Pro Racing technical staff. Any prior verbal approval from AMA Pro Racing staff or officials without a written statement from the Technical Department with regard to the interpretation of a rule or procedure will be deemed invalid. While every effort has been made to write these rules in a clear and unambiguous fashion, it is impossible to anticipate every circumstance. It will be the Race Director’s responsibility to make decisions regarding rule enforcement. DISCLOSURE: AMA PRO RACING STRIVES TO REGULATE THE SPORT OF PROFESSIONAL MOTORCYCLE RACING IN THE FAIREST POSSIBLE MANNER. ALL PARTIES INVOLVED IN AMA PRO RACING PROFESSIONAL RACES ARE EXPECTED TO CONDUCT THEMSELVES IN A PROFESSIONAL MANNER, RESPECTING AT ALL TIMES THE RIGHTS OF OTHERS. THE RULES FOR COMPETITION ARE INTENDED ONLY AS A GUIDE FOR THE CONDUCT OF THE SPORT PURSUANT TO THE UNIFORM RULES. -

OFFICIAL CAR of Motogp™. BMW M2 Motogp SAFETY CAR. MEDIA GUIDE 2016
BMW M Official Car of MotoGP™ Sheer Driving Pleasure BMW M – OFFICIAL CAR OF MotoGP™. BMW M2 MotoGP SAFETY CAR. MEDIA GUIDE 2016. FOREWORD. FRANK VAN MEEL, PRESIDENT OF BMW M DIVISION. Dear Media Representative, Millions of motorsport enthusiasts around the world are looking forward to the We dedicate all of our know-how to this role. The BMW M MotoGP start of the 2016 MotoGP season. The best riders in the world and breath- Safety Cars are innovative high-performance models with thoroughbred taking race action – MotoGP is undoubtedly the pinnacle of motorcycle racing. racing genes. In the 2016 season, we are presenting another genuine highlight. The new BMW M2 Coupé enjoyed its much-anticipated world We are proud to have been a part of this captivating world championship for debut in Detroit in January. In the BMW M2 MotoGP Safety Car, we are almost two decades. Since 1999 we have been a partner of MotoGP organiser now taking the pure power and dynamics of this high-performance automobile Dorna Sports, and 2016 marks the 18th season of BMW M as “Official Car of to the racetrack. Like its predecessors, the BMW M2 MotoGP Safety Car MotoGP”. We are pleased with the deep trust that Dorna Sports has placed uses technological innovation, performance, precision and agility to help in us. BMW M Division uses technology taken from motorsport, together with guarantee safety. innovative ideas, to ensure that race events run safely. In us, Dorna Sports knows that it has a strong partner on its side, for whom the safety of the riders on their high-performance racing prototypes has the utmost priority. -

Evaluation of Accidents and Injuries in International Rally Organizations Held in Turkey Ramazan SABIRLI1*, Damla ANBARLI METİN2, Emre KARSLI3 and Ömer ÇANACIK1
ISSN: 2474-3674 SABIRLI et al. Int J Crit Care Emerg Med 2020, 6:096 DOI: 10.23937/2474-3674/1510096 Volume 6 | Issue 1 International Journal of Open Access Critical Care and Emergency Medicine ORIGINAL RESEARCH ARTICLE Evaluation of Accidents and Injuries in International Rally Organizations Held in Turkey Ramazan SABIRLI1*, Damla ANBARLI METİN2, Emre KARSLI3 and Ömer ÇANACIK1 1 Check for Academic Emergency Department, Kafkas University, Turkey updates 2Çiğli Regional Educational Hospital, Turkey *Corresponding author: Dr. Ramazan Sabirli, Department of Emergency Medicine, Kafkas University, Kars, Turkey, Tel: +90-5387344298 Abstract incidences for WRX, Bosphorus Rally, WRC 2018, and WRC 2019 were 140.04/100 hours, 23.31/100 hours, International rally events, such as the World Rally Cham- 8.42/100 hours, and 13.26/100 hours, respectively. The ac- pionship (WRC) and the Bosphorus Rally and the World cindent incidences of WRX was found 6 times higher than Rally Cross Championship (WRX), have been held in Tur- Bosphorus Rally, 16.62 times higher than WRC 2018 and key from 2014 onwards. In all three rally organizations, the 10.55 times higher than WRC 2019. International Rally Federation (FIA) pay painstaking atten- tion to the points, such as race safety and safety of drivers The incidence of Class 1 accidents per race time in the as well as medical plan. four international rallies was calculated as 12/100 hours, while that of Class 2, Class 3, and Class 6 turned out to The rally car accidents and spectator accidents that occur- be 1.11/100 hours, 1.39/100 hours, and 0.2/100 hours, re- red in the international rally races held in Turkey (WRX, Bo- spectively. -

New Vegan Products! Pre-Race Meal 'Best
Our biggest issue ever! $3.95 'Best by' dates are back! Pre-race meal (Why less is more!) Incorporating Compex into your workout New vegan products! Product spotlight : PSA Caps www.hammernutrition.com 1 Laurie Hug secures a 2nd place podium finish at USMS Summer Nationals. Photo : www.wadleyphotography.com IN THIS ISSUE #82 Contents Letters 3 Athlete Spotlight : Eric Steele 48 Tribute to Hammer Nutrition 84 Welcome 4 ITU Long Course World Championships 50 Team Hammer 85 A day with the Duros 6 Coffee Corner : The Down Shift 52 Hammer Nutrition International 86 New vegan products for 2013 7 Join the coffee club 53 Ask Dr. Bill 88 Hammer Flask 8 Nate's Corner 54 Sponsored events 90 'Best by' dates are back 9 Kenda/Felt team's pro contenders 60 Living large in Death Valley 92 Recovery Bar musings 10 Just another day in the office 63 Team CMG 93 Brian's summer vacation 12 Proper fueling 64 Hammer Nutrition junior athletes 94 Product Spotlight : PSA Caps 14 Tales of a Cat 1 roadie 66 Hammerbuck$ winners 98 How to endure for life . 18 Fueling for 14,115' 68 From our athletes 102 Delta- and gamma-tocopherols 20 100 miles of guts, grit, and determination 70 Cycling skills with Mike Freeman 22 A solid plan for a solid finish 71 Hammer Camps 24 Where are they now? 72 Bell peppers 26 Enjoy FREE product with referrals 74 Yet another reason to avoid aspartame 28 Preparing for ski season 76 USMS Summer Nationals 30 CashCall rides to a podium finish 78 Peak performance with Compex 32 Arthur Webb blasts Badwater 80 Incorporating Compex into your workout 36 Where do you Hammer? Lake Michigan 82 Recovering, resting, and racing 38 Levi’s après workout lesson 40 Good days on the road to Kona 42 ON THE COVER From the kitchen of Bill Sirl 44 Bryan Mickiewicz pushes to a 4th place finish during the Battle the Bear MTB Marathon. -

Motor Sports
MOTOR SPORTS 1 Introduction 2 Car Racing Trends In 2015, the Japanese automotive industry continued Table 1 lists the main categories of car races held in- to benefit from the weak yen. side and outside Japan, and the results of each competi- In Japanese car racing, the newly developed 2.0-liter tion. inline 4-cylinder turbocharged engines adopted in the Su- 2. 1. Trends in Japan per GT and Super Formula race series achieved promis- In 2015, the new entry-level FIA Formula 4 (F4) series ing results and helped to stimulate a growing number of got off to a good start with around 40 entrants. However, close battles based on driver skill and team tactics. there were no major changes in either Super GT or Su- Outside Japan, Honda struggled in its return to For- per Formula after the substantial rule changes in 2014. mula 1 (F1), underlining the difficulty of achieving results 2. 1. 1. Super GT (Fig. 1) after the recent regulation changes. In the FIA World 2015 was the second year since the vehicle regulations Endurance Championship (WEC), Toyota also struggled were harmonized with those of the Deutsche Tourenwa- to reproduce its double title-winning success of a year gen Masters (DTM: German Touring Car Masters) series. ago. Porsche won the manufacturer’s title in its second These regulations include adopting common parts such season as new teams came to the forefront and Japanese as the monocoque, brakes, and gearbox. Each manufac- marques found success hard to come by. turer competes through development of the 2.0-liter In a new initiative, the Mazda Women in Motorsport 4-cylinder turbocharged direct injection engine and some project featuring Keiko Ihara attracted several hundred aerodynamic parts. -

Rennen! Vitesse! Races!
Rennen! Races! Vitesse! Racing Circuits Netherlands Belgium Germany Austria Luxembourg Switzerland Rob Semmeling Rennen! Races! Vitesse! Page 2 Contents Foreword 3 Netherlands 5 Belgium 44 Germany 78 Austria 133 Luxembourg & Switzerland 148 Copyright © Rob Semmeling 2009-2016 / all rights reserved www.wegcircuits.nl Rennen! Races! Vitesse! Page 3 Foreword Motorsport essentially consists of three ingredients. First, you need a motor vehicle - which can be anything from a Formula 1 car to a lawn mower, or from a MotoGP motorcycle to a pocket bike. Second, you need a driver or rider to operate the vehicle, and finally, a place to go racing - a circuit. To most people this last ingredient is probably the least interesting. The number of books about famous racing drivers and cars, or great riders and their motorcycles, is far larger than the number of books about racing circuits. However, to me circuits are the most interesting aspect of motorsport, for two main reasons. First is their great diversity: in terms of shape, layout, length, difficulty, fame and many other factors, every circuit is different, and each has its own story to tell. Second, it is fascinating to see just how many circuits there are. Once you start looking, you can find them just about any- where. Finding lost circuits or discovering long-forgotten tracks is one of the most fun aspects of researching racing circuits. When looking for information about racing circuits online, I often found it frustrating that the available sources were not complete, and that they often lacked detail and accuracy. This is one of the reasons why I started my website www.wegcircuits.nl and why I made Rennen! Races! Vitesse! - a downloadable pdf-file that lists racing circuits of past and present in four European countries: the Netherlands, Belgium, Germany and Austria.