Motor Racing Questionnaire
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Outlast Newsletter
Hello – With the first quarter of 2013 underway, we have many positive developments in the works to strengthen our brand positioning and continue to bring more products to market that feature the proactive benefits of our technology. We've rolled out our new brand identity that includes a refreshed logo. The new design pays respect to the strength and success of the Outlast brand as the global leader in phase change materials (PCMs) for the past 22 years, while encapsulating our relentless push for technological innovation in our field. To support this, our R&D team has introduced the world's first-ever polyester fiberfill with Outlast® technology - a development ideally suited for comforters, sleeping bags, jackets, etc. Outlast® Polyfill brings polyester fiber into the 21st century. Additionally, our partnerships continue to expand on the apparel front with a new women's boot to be introduced later this year from Papillon International. We're also working with Spanish company LS2 on new motorcycle racing helmets, as well as Ripzone™ on their line of Trilogy™ snowboarding jackets that will be lined with Outlast® technology for the 2013/2014 season. Our continued success, as always, is due in large part to our partnerships and relationships around the globe and everyone involved in our operations that contribute to expanded product offerings and applications. Warmest wishes to all of you in the New Year. Sincerely, Michael Coors CEO, Outlast Technologies Papillon International Introduces Women's Riding Boot - Fall Preview! We've partnered with Papillon International to bring to market women's riding boots for the fall 2013 season, featuring Outlast® technology in the ankle and foot lining, and the sock footbed. -

Revs Institute for Automotive Research, to Keep You Updated, at Le Mans
SUMMER 2012 V OL 1, ISSU E 02 Revs I NSTITUTE fO R AUTOMOTI ve R ESearCH REVIEW INTRODUCING REILLy P. BRENNAN The Revs Program at Stanford works closely with the Revs Institute in Naples. The Revs Program at Stanford is well on its way to becoming a foremost center of interdisciplinary study of the automobile. A major step forward took place earlier this year with the hiring of REVS INSTITUTe fOR Reilly P. Brennan as the new Executive Director. Prior to joining Stanford AUTOMOTive ReSEARCH University, Reilly was the Editorial Director Elevating the study of the automobile, not only as a at AOL’s automotive sites and properties. technological device, but as an agent for social and economic He has over a decade of experience in change, and worthy to be considered among the masterpieces media and communications associated with the world of cars. Reilly was notably part of of mankind’s creation. The Revs Review is a publication of the the team that brought victory to Corvette Revs Institute for Automotive Research, to keep you updated, at Le Mans. He has also written extensively informed and Revved Up! for several magazines and was the co- founder of an online automotive database. he Revs Institute for Automotive Research, Reilly is an enthusiastic “car guy” who Inc. is a not for profit 501(c)3 private operating has logged many hours in test vehicles foundation. It is a growing leader as an and brings both expertise and passion to developing the Revs Program. Among information destination and image resource for his first initiatives at Stanford will be to Tan international community of transportation establish a scholarship aimed at helping and automotive professionals, enthusiasts and authors with worthy publishing projects in students. -

Porsche 919 Hybrid English.Indd
Porsche 919 Hybrid Return to top-level sport Porsche is making its comeback to the top-level motorsport arena: with the new 919 Hybrid the sports car brand is sending a platform for pioneering technology to the top category of the FIA World Endurance Championship (WEC) with the undisputed seasonal highlight of the 24-hour Le Mans race. Porsche's reputation precedes it at this venue: with 16 overall victories under its belt, the brand holds the record for this, the most famous endurance race in the world. In 2014 Porsche is returning to the top-level class endurance race after a 16-year absence - namely Le Mans Prototypes (LMP1). Matthias Müller, Chairman of the Executive Board of Porsche AG explains: "The new and revolutionary efficiency regulations for this class were what prompted us to take this step. In 2014 it is not going to be the fastest contender who is going to win the sports car world championship and Le Mans, but the car that gets furthest with the defined amount of energy. And it is precisely this challenge that the automotive industry has to face. The 919 Hybrid is like a high speed research laboratory and the most complex racing car Porsche has ever built." The new WEC regulations for the LMP1 racing car gives engineers an unusual amount of leeway and demands pioneering technology, such as hybridisation, downsizing engines and consistent lightweight construction. This is all particularly relevant for the development of future generations of factory-spec sports cars. Maximum sporting performance and highest efficiency are at the heart of "Porsche Intelligent Performance". -
MDC Physical Activity
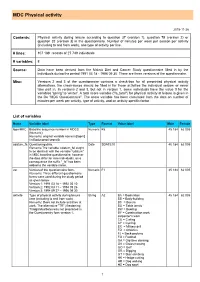
MDC Physical activity 2015-11-26 Contents: Physical activity during leisure according to question 37 (version 1), question 75 (version 2) or question 32 (version 3) in the questionnaire. Number of minutes per week per season per activity (including to and from work), one type of activity per line. # lines: 107 189 records of 27 749 individuals # variables: 8 Source: Data have been derived from the Malmö Diet and Cancer Study questionnaire filled in by the individuals during the period 1991 03 18 - 1996 09 30. There are three versions of the questionnaire. Misc: Versions 2 and 3 of the questionnaire contains a check-box for all preprinted physical activity alternatives, the check-boxes should be filled in for those activities the individual seldom or never take part in. In versions 2 and 3, but not in version 1, some individuals have the value 0 for the variables 'spring' to 'winter'. A total score variable ("fa_total") for physical activity at leisure is given in the file "MDC Questionnaire". The score variable has been calculated from the data on number of minutes per week per activity, type of activity, and an activity specific factor List of variables Name Variable label Type Format Value label Male Female lopnrMKC Baseline sequence number in MDCS Numeric F5 45 184 62 005 (Numeric). Remarks: original variable name is [lopnr] (in Bodycomp [seqno]). udatum_fa Questioning date. Date SDATE10 45 184 62 005 Remarks:The variable 'udatum_fa' ought to be identical with the variable "udatum" in MDC baseline questionnaire, however the date differ for nine individuals, as a consequence the suffix "_fa" has been added to the variable name. -

Fresno Chapter Event 8&9 SFR Goes to the Runoffs 2020 Election Board
1948–2020 CELEBRATING 72 YEARS VOL. 61 | October 2020 The official publication of the San Francisco Region of the Sports Car Club Of America Fresno Chapter Event 8&9 p. 8 SFR Goes to the Runoffs p. 10 2020 Election Board of Directors p. 21 SONOMA RACEWAY (800) 708-RACE WWW.WINECOUNTRYMOTORSPORTS.COM ASK ABOUT OUR SCCA SPECIALS! ARE YOU READY FOR THE NEW RULE REQUIRING FORWARD FACING CAMERAS? WE ARE! SPECIALS FOR SCCA! GoPro Hero 7 Silver GoPro Hero 8 Black AIM Smartycam HD $19999 $39999 $999 FREE 32GB SD CARD FREE ROLL BAR MOUNT FREE ROLL BAR MOUNT CALL 800-708-7223 TO ORDER - GET IT SHIPPED TO YOU AT NO EXTRA COST! CAMLOCK 2020 HARNESSES SEASON AUTO RACING SUITS KICKOFF 15% OFF 10-30% OFF Start at $15995 MAY 2020 Above-Michael Gardner topping CAMC both days in his GT350 On the cover: Ric Quinonez in his AMOD taking TTOD both days. Paul Newton in the Peelz 718 Cayman GT4 Clubsport 6 The Way of the Fist 14 Wheelworks 18 Thunderhill Rally Cross Final 21 2020 Election Board of directors 8 Fresno Chapter 16 Motorsports News 19 Dick Mudd FEATURES 26 Notes From The Archives 10 SFR Goes to the Runoofs 18 Profile: Rhea Dods 20 Confessions of a Cone Slayer 28 Thunderhill Report IN EVERY ISSUE 4 Calendar 4 Travel Tech 29 Race Car Rentals 30 The Garage: Classified Ads The views expressed in The Wheel are those of the authors and do not necessarily reflect the position or policy of San Francisco Region or the SCCA. -

A Guide to ICSCC Race Classes
A Guide to ICSCC Race Classes This is meant as a general guide only. For specific requirements refer to the ICSCC Competition Regulations. Sports car racing has the most variety of cars of any type of racing. The cars can be broken down into four basic types: Production cars, GT cars, Formula cars, and Sports Racers. Within each of these types, there are numerous classifications: 53 in all. These classifications are divided into six race groups, and all cars assigned to a particular group will run all practice, qualifying, and races together. Any race has several classes of cars running, so there will be races within the race. This can lead to some confusion as to what is happening on track! This guide will help you sort it out... Production Cars The Production cars are the closest to street vehicles, and many are driven to and from the track. There are very limited modifications permitted. The drive train is for all practical purposes stock. The interior can be stripped to reduce fire hazard, and basic safety equipment is added, such as a roll cage and fire suppression systems. Production cars are divided into ten classes designated ‘A’ through ‘J’. Markings on the car will tell you which class they are in: AP, BP, CP, and so on. The cars are placed into a class by using the ratio of horsepower to curb weight as a guide. Other factors will affect the classification of a particular car such as type of tires being used. As you watch the Production cars you will notice that certain models of cars domi- nate in a given class. -
History of the Alpine Brand
HISTORY OF THE ALPINE BRAND Alpine is the story of a brand, but it is also the story of men before being, tomorrow, the story of a renewal. CONTENTS I. A "RENAULT" FAMILY II. JEAN RÉDÉLÉ, RACING CHAMPION III. THE CREATION OF ALPINE IV. FROM ALPINE TO ALPINE-RENAULT V. AN INNOVATIVE EXPORT POLICY VI. ALPINE’S REBIRTH VII. MOTORSPORT, ALPINE’S DNA VIII. ALPINE: A HISTORY OF MEN IX. ALPINE PRODUCTION IN FIGURES X. SOME TITLES WON BY ALPIN 1 Confidential C I. A RENAULT ‘FAMILY’ Jean Rédélé was the first-born son of Madeleine Prieur and Emile Rédélé, a Renault dealer based in Dieppe and a former mechanic of Ferenc Szisz – the first Renault Frères ‘factory driver’, winner of the Grand Prix de la Sarthe in 1906 at Le Mans and runner-up in the Grand Prix de l'A.C.F. in Dieppe in 1907. Louis Renault himself had hired Emile Rédélé right at the beginning of the 20th Century. At the end of the First World War, at the request of Louis Renault, the young Emile Rédélé settled in Dieppe and opened a Renault dealership there in rue Thiers. Two years later, Jean-Emile- Amédée Rédélé was born on May 17, 1922. After completing his studies in Normandy, Jean Rédélé took his Baccalauréat exam during the Second World War and came into contact with people as diverse as Antoine Blondin, Gérard Philipe and Edmond de Rothschild. He chose to be a sub-prefect before settling on a career direction and enrolling at the H.E.C. -

Motocross Isa Team Sport...Sure Most Consider Motorcycle Racing An
Motocross IS a team sport ....Sure most consider motorcycle racing an Individual action. Yes, you can do It alone, but when we look at the big picture we clearly see there are so many elements that are Involved In the sport Many of us on the outside do not realize the behind scenes preparation The work that It takes ... From sign up to trophies .... An enormous amount of organization IS Involved April 17, 1978, a man by the name of Jerry Sharp opened a European style motocross track in Springfield, Missoun. The name of the track was Possum Hollow In dedication to their adventure In finding the ground At this time there were only three motocross tracks In the state of Mlssoun, Cycle World USA In SI. lOUIS, lake City In the Kansas City area, and Possum Hollow In Spnngfleld. For the next three years Jerry and wife, Ellie, promoted and organ- Ized motocross races at the Ozark Empire Fair Grounds and Possum Hollow It s said that Jerry was fifteen to twenty years ahead of his time In the arenacross style of racing. In 1981 Jerry started a senes that Included two tracks, Gene lewIs' lake City and his very own Possum Hollow. Tied to the GNC the events were qualifiers, at that time, for Ponca City and lake Whitney In Texas. As the years flew by Jerry continued his full time job With Gibson Greeting Cards travel- ing the states of Missoun and northern Arkansas puttmg In fifty to sixty hour weeks and still bUilding and promoting the senes. -

The Squeal | March 2015
March 2015 Sports Car Club of America, Inc. - Incorporated June 29, 1959 You Won’t Find This Another Episode On SCCA’s Calendar Of “Un-Barn Find” Inside Alan Lesher has another of his “Un-Barn Find” discoveries to tell about, this time it’s a 1983½ Dodge Shelby Charger. Alan found this car in somewhat race trim and went to work refining and turning it into a versatile race platform capable of track work, hillclimbing and autocrossing. Check out Alan’s full story on Page 4. q These guys have donned their helmets for an early auto competition. Photo from the George Grantham Bain Collection, Library of Congress Henry Brillinger has dug deeply into automobile competition and came up with a form of Gymkhana that for obvious reasons didn’t make it to modern times. Check out Henry’s story on Page 11. q Also In This Issue Daren Stonesifer tell us about a new motor for his race program on Page 8 and Ed Womer Since Alan Lesher purchased this Shelby Charger, tells of his recent trip to Daytona International he has spent several years refining it for a variety of competition venues.. — Chris Paveglio photo Raceway for the Rolex 24 Hour on Page 13. q From the Page 2 Editor’s 2 MARCH 2015 The Squeal is a monthly publication of Desk Susquehanna Region, SCCA Send editorial, scheduling and advertising to: SATURDAY! SATURDAY!, SATURDAY! The Squeal — John Rudy, Editor 3800 Hillcrest Road, Harrisburg, PA 17109 SUNDAY! SUNDAY! SUNDAY! [email protected] HERSHEY PARK LARGE LOT! BE THERE! Susquehanna Region begins its competition Susquehanna Region’s membership meets season this weekend in Hershey with at 7:30 PM on the fourth Tuesday of each Autocross #1 on Saturday and Autocross #2 on month, except December, at Gilligan’s Bar & Grill, 987 Eisenhower Blvd, Harrisburg, PA. -

Racetrack Safety Guidelines
RACETRACK SAFETY GUIDELINES Published by CIRSA 3665 Cherry Creek North Drive Denver, Colorado 80209 800.228.7136 FAX 303.757.8950 www.cirsa.org © CIRSA 2007 Table of Contents I. Introduction 2 II. Location 2 III. Operation, Maintenance & Inspection 3 IV. Event Operation 4 V. Claims Reporting & Investigation 4 VI. Budgeting 4 VII. Release of Liability & Indemnifi cation Agreement 6 VIII. Audit & Inspection Sample Checklists 9 * This publication is meant for informational purposed only, and as with all CIRSA publications, is intended only to assist CIRSA members in their own loss control activities. It is not intended to replace programs and activities, or provide specifi c legal, technical, or other advice. * 1 Introduction Automobile racing in America can be traced back to 1895, when six racers competed in a 54 mile race from Chicago to Evanston, Illinois and back for a $2,000 prize. Through snowy condi- tions, Frank Duryea crossed the fi nish line fi rst with a time of 10 hours and 23 minutes. The love of speed and competition has catapulted the popularity of racing as well as the types of racing to new highs annually. Autos and motorcycles are raced in a gamut of categories and the availability of local facilities draws many participants of all skill levels. Municipalities may own a racing facility, be it a drag strip, road course, or an old airport runway con- verted to a race track in efforts to bring tourism and revenue to the local area. Owning and operating a facility for this high risk activity is normally outside the scope of standard municipal operations, such as water treatment or playground maintenance. -

Brembo Confirms Motorsport Leadership with Wins in 2020
BREMBO CONFIRMS MOTORSPORT LEADERSHIP WITH WINS IN 2020 The competition record of the company is enriched with over 42 titles won in 2020, with the result of 500 world championships won in the main Motorsport categories Brembo, leader in high performance braking systems, confirms its technological supremacy in Motorsport through the many championships won with teams and manufacturers in 2020. With 42 world titles won, including drivers, manufacturers and team titles the Brembo group, Motorsport supplier for over 45 years, reaches the milestone of *500 world titles obtained in various two and four-wheel competitions. In Formula 1 all of the 17 Grand Prix races in the current season have been won by cars equipped with Brembo components. The Bergamo-based company can boast victories in 442 out of 785 Grand Prix that have taken place since 1975, the year of the debut in Formula 1, until today, for a total of 26 world drivers’ championships and 30 world constructors’ championship won with the top teams. Brembo’s dominance also continues in MotoGP, to which are added new wins in Moto2 and Moto3 (also with Marchesini). Over 500 victories in the premier class (500 class and MotoGP): for the fifth consecutive season Brembo supplied all the teams. Specifically, the 27 riders who raced at least one race in MotoGP this year relied on the high levels of performance and safety guaranteed by Brembo components: brake calipers, carbon discs and pads, brake pumps and clutch pumps. Starting from 1978 to 2001, it’s possible to count the first 185 GPs won by bikes with Brembo brakes in the 500 class. -

Open Exhaust - Summer 2021
Open Exhaust - Summer 2021 What’s in this issue: The official newsletter of the Detroit Region of SCCA ® Thanks to Ralph Thayer Auto- The Club motive for supporting our Ral- About us Scott Beutte at Saginaw lycross program. Join the Club Fairgrounds RX test day. Solo Results Pic by Ryan Long Solo Nationals Formula SAE RallyX Enthusiast of the year New RallyX venue Summer Daze Rallycross Rallycross Nationals Links: Detroit Region Website Press on Regardless Facebook page Detroit Grand Prix Facebook Solo Corner Workers Facebook Rallycross SCCA Steering “Wheel” MotorsportReg Moonlight Monte TSD Cincinnati Region 2021 Runoffs at Indy Saginaw Valley Region Western MI Region SCCA 2022 Convention NE Ohio Region Area 4 update—Dayle Frame Waterford Hills Racetrack Long Service Awards Note that there are many links expanding on the stories. Also, Michigan Turn Marshals some of the photos are clickable for higher resolution. Grattan Raceway MIS Ralph Thayer Automotive Open Exhaust Volume MMXXI, Issue 2 © 2021 SCCA Detroit Region - All Rights Reserved Page 1 8/23/2021 About us Director and officials Membership Frank Putman Regional Executive The Detroit Region of the Sports Car Club of America is one of the larger regions Cindy Wisner Assistant Regional Executive with about 1400 members. It has something for every taste, including some of the country’s best organized Rallycross, Solo, and TSD Rallies. Brian Thorpe Secretary, Open Exhaust Editor Membership includes a subscription to Sports Car magazine, discounts and sav- Greg Valade Treasurer, ings, schools and classes, experts and information and insurance while participat- Dan Assenmacher Financial Director ing at SCCA events.