Mhealth Series
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Renao (Heat-Noise), Deities’ Efficacy, and Temple Festivals in Central and Southern Hebei Provincel
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Apollo Journal of Cambridge Studies 1 Renao (Heat-noise), Deities’ Efficacy, and Temple Festivals in Central and Southern Hebei Provincel Zhiya HUA School of Social Administration, Shanghai University of Political Science and Law, PRC [email protected] Abstract: There is a tradition of holding temple festivals in villages in central and southern Hebei Province. This tradition was once suspended after the establishment of P.R.C., but it revived and thrived after the reform and opening-up. Temple festivals are a kind of renao (热闹, heat-noise) events in rural life, and the organizers of temple festivals pursue the effect of renao as much as possible. Renao is a popular life condition welcomed by people; meanwhile, it can be regarded as an important exterior indicator of the efficacy of deities. Hence holding temple festivals and make renao at them provides an opportunity not only for people to experience and enjoy renao, but to acknowledge, publicize, and even produce the efficacy of deities. These sacred and secular rewards can partly account for the enduring resilience and vitality of the local tradition of holding temple festivals. Key Words: Temple festivals, Renao, Efficacy, Folk religion, Central and Southern Hebei Province This article is based on a part of the author’s Ph.D. dissertation. The author is grateful to Prof. Graeme Lang for his instruction and criticism. In addition, the author wants to thank Dr. Yue Yongyi for his criticism and help. This article is also one of the outcomes of a research project sponsored by Shanghai Pujiang Program (No. -

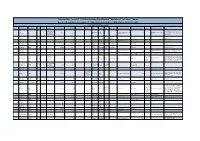
Table of Codes for Each Court of Each Level
Table of Codes for Each Court of Each Level Corresponding Type Chinese Court Region Court Name Administrative Name Code Code Area Supreme People’s Court 最高人民法院 最高法 Higher People's Court of 北京市高级人民 Beijing 京 110000 1 Beijing Municipality 法院 Municipality No. 1 Intermediate People's 北京市第一中级 京 01 2 Court of Beijing Municipality 人民法院 Shijingshan Shijingshan District People’s 北京市石景山区 京 0107 110107 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Haidian District of Haidian District People’s 北京市海淀区人 京 0108 110108 Beijing 1 Court of Beijing Municipality 民法院 Municipality Mentougou Mentougou District People’s 北京市门头沟区 京 0109 110109 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Changping Changping District People’s 北京市昌平区人 京 0114 110114 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Yanqing County People’s 延庆县人民法院 京 0229 110229 Yanqing County 1 Court No. 2 Intermediate People's 北京市第二中级 京 02 2 Court of Beijing Municipality 人民法院 Dongcheng Dongcheng District People’s 北京市东城区人 京 0101 110101 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Xicheng District Xicheng District People’s 北京市西城区人 京 0102 110102 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Fengtai District of Fengtai District People’s 北京市丰台区人 京 0106 110106 Beijing 1 Court of Beijing Municipality 民法院 Municipality 1 Fangshan District Fangshan District People’s 北京市房山区人 京 0111 110111 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Daxing District of Daxing District People’s 北京市大兴区人 京 0115 -

Annual Report 2015
ANNUAL REPORT 2015 Annual Report 2015 .suntien.com w ww Contents Chairman’s Statement 2 Corporate Profile 4 Financial Highlights and Major Operational Data 13 Management Discussion and Analysis 16 Human Resources 33 Biographies of Directors, Supervisors and Senior Management 35 Report of the Board of Directors 41 Corporate Governance Report 59 Report of the Board of Supervisors 72 Independent Auditors’ Report 75 Consolidated Statement of Profit or Loss and Other Comprehensive Income 77 Consolidated Statement of Financial Position 78 Consolidated Statement of Changes in Equity 80 Consolidated Statement of Cash Flows 81 Notes to Financial Statements 83 Definitions 180 Corporate Information 183 China Suntien Suntien Green Green Energy Energy Corporation Corporation Limited Limited Annual AnnualReport 2015 Report 2015 Chairman’s Statement 2 China Suntien Green Energy Corporation Limited Annual Report 2015 Chairman’s Statement Dear Shareholders, In 2015, due to the continual weakening of the global economic recovery and complicated economic situation, international trade contracted and financial risks increased. China’s economy was also at an unfavourable stage of “triple transition”, during which the economic growth decelerated with mounting downward pressure. In the meantime, the Company also faced with complicated and severe situations such as price reduction in wind power, declining demand of natural gas and difficulties encountered by infrastructure projects. The Board of Directors of the Company strived for making progress while maintaining stability, proactively responding to market changes and making preparations and plans so as to direct all employees to unite together and forge ahead. We also continued to speed up the process to seize market resources inside and outside the province, accelerated the progress of project construction and expanded the domestic and overseas financing channels, which greatly enhanced internal management and steadily optimized the business structure of the Company. -

Deities' Efficacy, and Temple Festivals in Central and Southern Hebei
Journal of Cambridge Studies 1 Renao (Heat-noise), Deities’ Efficacy, and Temple Festivals in Central and Southern Hebei Provincel Zhiya HUA School of Social Administration, Shanghai University of Political Science and Law, PRC [email protected] Abstract: There is a tradition of holding temple festivals in villages in central and southern Hebei Province. This tradition was once suspended after the establishment of P.R.C., but it revived and thrived after the reform and opening-up. Temple festivals are a kind of renao (热闹, heat-noise) events in rural life, and the organizers of temple festivals pursue the effect of renao as much as possible. Renao is a popular life condition welcomed by people; meanwhile, it can be regarded as an important exterior indicator of the efficacy of deities. Hence holding temple festivals and make renao at them provides an opportunity not only for people to experience and enjoy renao, but to acknowledge, publicize, and even produce the efficacy of deities. These sacred and secular rewards can partly account for the enduring resilience and vitality of the local tradition of holding temple festivals. Key Words: Temple festivals, Renao, Efficacy, Folk religion, Central and Southern Hebei Province This article is based on a part of the author’s Ph.D. dissertation. The author is grateful to Prof. Graeme Lang for his instruction and criticism. In addition, the author wants to thank Dr. Yue Yongyi for his criticism and help. This article is also one of the outcomes of a research project sponsored by Shanghai Pujiang Program (No. 13PJC099). Volume 8, No. -
Documented Cases of 1,352 Falun Gong Practitioners "Sentenced" to Prison Camps
Documented Cases of 1,352 Falun Gong Practitioners "Sentenced" to Prison Camps Based on Reports Received January - December 2009, Listed in Descending Order by Sentence Length Falun Dafa Information Center Case # Name (Pinyin)2 Name (Chinese) Age Gender Occupation Date of Detention Date of Sentencing Sentence length Charges City Province Court Judge's name Place currently detained Scheduled date of release Lawyer Initial place of detention Notes Employee of No.8 Arrested with his wife at his mother-in-law's Mine of the Coal Pingdingshan Henan Zhengzhou Prison in Xinmi City, Pingdingshan City Detention 1 Liu Gang 刘刚 m 18-May-08 early 2009 18 2027 home; transferred to current prison around Corporation of City Province Henan Province Center March 18, 2009 Pingdingshan City Nong'an Nong'an 2 Wei Cheng 魏成 37 m 27-Sep-07 27-Mar-09 18 Jilin Province County Guo Qingxi March, 2027 Arrested from home; County Court Zhejiang Fuyang Zhejiang Province Women's 3 Jin Meihua 金美华 47 f 19-Nov-08 15 Fuyang City November, 2023 Province City Court Prison Nong'an Nong'an 4 Han Xixiang 韩希祥 42 m Sep-07 27-Mar-09 14 Jilin Province County Guo Qingxi March, 2023 Arrested from home; County Court Nong'an Nong'an 5 Li Fengming 李凤明 45 m 27-Sep-07 27-Mar-09 14 Jilin Province County Guo Qingxi March, 2023 Arrested from home; County Court Arrested from home; detained until late April Liaoning Liaoning Province Women's Fushun Nangou Detention 6 Qi Huishu 齐会书 f 24-May-08 Apr-09 14 Fushun City 2023 2009, and then sentenced in secret and Province Prison Center transferred to current prison. -

The Nation-State, the Contract Responsibility System, and the Economy of Temple Incense: the Politics and Economics of a Temple Festival on a Landscaped Holy Mountain
Rural China: An International Journal of History and Social Science 13 (2016) 240-287 brill.com/rchs The Nation-State, the Contract Responsibility System, and the Economy of Temple Incense: The Politics and Economics of a Temple Festival on a Landscaped Holy Mountain Yongyi Yue* School of Chinese Language and Literature, Beijing Normal University, China [email protected] 民族国家、承包制与香火经济: 景区化圣山庙会的政治-经济学 岳永逸 Abstract Belief practices in mainland China have been subject to contracts as a result of a combination of factors: politics, economic growth, cultural development, and historic preservation. Thanks to the investigative reporting of the media, “contracting out belief” has lost all legitimacy on the level of politics, culture, religion, administration, and morality. The economy of temple incense has been re- lentlessly criticized for the same reason. In recent decades, Mount Cangyan, in Hebei, has changed from being a sacred site of pilgrimage to a landscaped tourist attraction. At the same time, the Mount Cangyan temple festival, which centers on the worship of the Third Princess, has gained legitimacy on a practical level. Conventional and newly emerged agents, such as beggars, charlatans, spirit me- diums, do-gooders, and contractors of the temple, are actively involved in the thriving temple fes- tival, competing, and sometimes cooperating, with each other. However, it is for the sake of maxi- mizing profit that landscaped Mount Cangyan under the contract responsibility system has been re-sanctified around the worship of the Third Princess along with other, new gods and attractions. The iconic temple festival on this holy mountain has influenced other temple festivals in various nearby * Yue Yongyi is a professor of the Institute of Folk Literature, School of Chinese Language and Lit- erature, Beijing Normal University, and an associate editor of the Cambridge Journal of China Studies. -

Hebei Small Cities and Towns Development Demonstration Sector Project
Resettlement Planning Document Resettlement Plan Document Stage: Final Project Number: 40641 October 2008 People’s Republic of China: Hebei Small Cities and Towns Development Demonstration Sector Project Prepared by Urban Construction Investment Co. Ltd of Zhao County. The resettlement plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB’s Board of Directors, Management, or staff, and may be preliminary in nature. Zhaozhou Township Infrastructure Improvement Component Resettlement Plan Urban Construction Investment Co. Ltd. of Zhao County 1st October 2008 ENDORSEMENT LETTER FOR THE RESETTLEMENT PLAN With sufficient assistances from all sub-project units, we have prepared and compiled this Resettlement Plan (RP) for Zhaozhou Township Infrastructure Improvement Project. This RP is in accordance with relevant laws, policies and regulations of PRC, Hebei Province, Shijiazhuang City and Zhao County as well as the involuntary resettlement policies of Asian Development Bank. We endorse the actuality of the PR and have the commitment to the smooth implementation of land acquisition, house demolition, resettlement, compensation and budget. The PR is based on the Feasibility Study Report and the primary socio-economic survey. Once the project construction differs from the Feasibility Study Report and impacts on the implementation of the PR essentially, the PR should be revised timely and appropriately and reported to ADB for approval before its implementation. Chief Manager of Urban Construction -

Prevalence of Mobile Phones and Factors Influencing Usage by Caregivers of Young Children in Daily Life and for Health Care in Rural China: a Mixed Methods Study
RESEARCH ARTICLE Prevalence of Mobile Phones and Factors Influencing Usage by Caregivers of Young Children in Daily Life and for Health Care in Rural China: A Mixed Methods Study Michelle Helena van Velthoven1☯,YeLi2☯, Wei Wang2, Li Chen2, Xiaozhen Du2, Qiong Wu2, Yanfeng Zhang2*, Igor Rudan3, Josip Car1 a11111 1 Global eHealth Unit, Department of Primary Care and Public Health, Imperial College London, London, United Kingdom, 2 Department of Integrated Early Childhood Development, Capital Institute of Paediatrics, Beijing, China, 3 Centre for Population Health Sciences and Global Health Academy, University of Edinburgh Medical School, Edinburgh, United Kingdom ☯ These authors contributed equally to this work. * [email protected] OPEN ACCESS Citation: van Velthoven MH, Li Y, Wang W, Chen L, Abstract Du X, Wu Q, et al. (2015) Prevalence of Mobile Phones and Factors Influencing Usage by Caregivers of Young Children in Daily Life and for Health Care in Introduction Rural China: A Mixed Methods Study. PLoS ONE To capitalise on mHealth, we need to understand the use of mobile phones both in daily life 10(3): e0116216. doi:10.1371/journal.pone.0116216 and for health care. Academic Editor: Don Operario, Brown University, UNITED STATES Objective Received: September 5, 2014 To assess the prevalence and factors that influence usage of mobile phones by caregivers Accepted: December 5, 2014 of young children. Published: March 19, 2015 Copyright: © 2015 van Velthoven et al. This is an Materials and Methods open access article distributed under the terms of the A mixed methods approach was used, whereby a survey (N=1854) and semi-structured in- Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any terviews (N=17) were conducted concurrently. -

Distribution, Genetic Diversity and Population Structure of Aegilops Tauschii Coss. in Major Whea
Supplementary materials Title: Distribution, Genetic Diversity and Population Structure of Aegilops tauschii Coss. in Major Wheat Growing Regions in China Table S1. The geographic locations of 192 Aegilops tauschii Coss. populations used in the genetic diversity analysis. Population Location code Qianyuan Village Kongzhongguo Town Yancheng County Luohe City 1 Henan Privince Guandao Village Houzhen Town Liantian County Weinan City Shaanxi 2 Province Bawang Village Gushi Town Linwei County Weinan City Shaanxi Prov- 3 ince Su Village Jinchengban Town Hancheng County Weinan City Shaanxi 4 Province Dongwu Village Wenkou Town Daiyue County Taian City Shandong 5 Privince Shiwu Village Liuwang Town Ningyang County Taian City Shandong 6 Privince Hongmiao Village Chengguan Town Renping County Liaocheng City 7 Shandong Province Xiwang Village Liangjia Town Henjin County Yuncheng City Shanxi 8 Province Xiqu Village Gujiao Town Xinjiang County Yuncheng City Shanxi 9 Province Shishi Village Ganting Town Hongtong County Linfen City Shanxi 10 Province 11 Xin Village Sansi Town Nanhe County Xingtai City Hebei Province Beichangbao Village Caohe Town Xushui County Baoding City Hebei 12 Province Nanguan Village Longyao Town Longyap County Xingtai City Hebei 13 Province Didi Village Longyao Town Longyao County Xingtai City Hebei Prov- 14 ince 15 Beixingzhuang Town Xingtai County Xingtai City Hebei Province Donghan Village Heyang Town Nanhe County Xingtai City Hebei Prov- 16 ince 17 Yan Village Luyi Town Guantao County Handan City Hebei Province Shanqiao Village Liucun Town Yaodu District Linfen City Shanxi Prov- 18 ince Sabxiaoying Village Huqiao Town Hui County Xingxiang City Henan 19 Province 20 Fanzhong Village Gaosi Town Xiangcheng City Henan Province Agriculture 2021, 11, 311. -

Minimum Wage Standards in China August 11, 2020
Minimum Wage Standards in China August 11, 2020 Contents Heilongjiang ................................................................................................................................................. 3 Jilin ............................................................................................................................................................... 3 Liaoning ........................................................................................................................................................ 4 Inner Mongolia Autonomous Region ........................................................................................................... 7 Beijing......................................................................................................................................................... 10 Hebei ........................................................................................................................................................... 11 Henan .......................................................................................................................................................... 13 Shandong .................................................................................................................................................... 14 Shanxi ......................................................................................................................................................... 16 Shaanxi ...................................................................................................................................................... -

Mobile Phone Text Messaging Data Collection on Care-Seeking for Childhood Diarrhoea and Pneumonia in Rural China: a Mixed Methods Study
Mobile phone text messaging data collection on care-seeking for childhood diarrhoea and pneumonia in rural China: a mixed methods study Helena Maria Marcella Theodora van Velthoven Global eHealth Unit Department of Primary Care and Public Health School of Public Health Imperial College London A thesis submitted for the degree of Doctor of Philosophy 2014 2 3 Abstract Background. Health information systems are inadequate in many countries. For childhood diarrhoea and pneumonia specifically, the leading infectious causes of child mortality worldwide, current data collection methods are not providing sufficient information for surveillance. The collection of health data could be greatly assisted with the use of mobile devices (mHealth). Mobile phone text messaging is widely used, but its potential for health data collection has not yet been realised. Aim. To explore the application of mHealth-based collection of information relevant to childhood diarrhoea and pneumonia in rural China. Methods. A mixed methods approach was used: (i) a survey and semi-structured interviews to assess the usage of mobile phones by caregivers of young children; (ii) cognitive interviews, usability testing and a cluster randomised cross-over study to determine the validity of a text messaging survey on care-seeking for childhood diarrhoea and pneumonia; and (iii) researchers’ observations and structured interviews with participants of the cross-over study to evaluate factors influencing participation in mHealth-based studies. Results. Many of the 1854 survey participants (1620; 87.4%) used mobile phones. Of 1014 participants in the cross-over study, 662 (65.3%) responded to the first text message. Of 651 participants willing to participate, 356 (54.7%) completed the text messaging survey. -
Environmental Monitoring Report
Environmental Monitoring Report Project Number: 40641-013 December 2011 PRC: Hebei Small Cities and Towns Development Demonstration Sector Project Submitted by: Hebei Project Management Office This environmental monitoring report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Environmental Monitoring Report (July 2011 to December 2011) Hebei Small Cities and Towns Development Demonstration Sector Project ADB Loan NO.: 2574-PRC Submitted to Asian Development Bank Submitted by: Hebei Project Management Office Prepared by HydroQual Inc. In association with China Construction Design International Group Co. December 30, 2011 ABBREVIATIONS ADB Asian Development Bank EA executing agency EIA environmental impact assessment EMC environmental monitoring consultant EMP environmental management plan EPB environmental protection bureau ESE environmental supervision engineer GDP Gross Domestic Products IA Implementing Agency LA Loan Agreement BUCDC Bazhou Urban Construction Development Co., Ltd. ZCCCIC Zhao County City Construction Invesrment Co., Ltd. HCSWTC Hebei Changshan Solid Waste Treatment Co., Ltd. TFDHWWTC Tangshan Fengnan Huichong Waste Water Treatment Co., Ltd. HWSC Huaian Water Supply Company HQWWTC Huaian Qingyuan Waste Water Treatment Co., Ltd. HHHPC Huaian Huayuan Heating Power Co., Ltd. ZCBCDC Zhulu County Boda Construction Development Co., Ltd. ZWSC Zhulu Water Supply Company PWSC Pingquan Water Supply Company CLHC Chengde Longhong Heating Co., Ltd.