Sensory Aids for the Deaf and the Blind
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Electromagnetic Field and TGF-Β Enhance the Compensatory
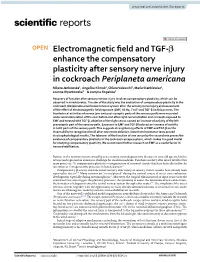
www.nature.com/scientificreports OPEN Electromagnetic feld and TGF‑β enhance the compensatory plasticity after sensory nerve injury in cockroach Periplaneta americana Milena Jankowska1, Angelika Klimek1, Chiara Valsecchi2, Maria Stankiewicz1, Joanna Wyszkowska1* & Justyna Rogalska1 Recovery of function after sensory nerves injury involves compensatory plasticity, which can be observed in invertebrates. The aim of the study was the evaluation of compensatory plasticity in the cockroach (Periplaneta americana) nervous system after the sensory nerve injury and assessment of the efect of electromagnetic feld exposure (EMF, 50 Hz, 7 mT) and TGF‑β on this process. The bioelectrical activities of nerves (pre‑and post‑synaptic parts of the sensory path) were recorded under wind stimulation of the cerci before and after right cercus ablation and in insects exposed to EMF and treated with TGF‑β. Ablation of the right cercus caused an increase of activity of the left presynaptic part of the sensory path. Exposure to EMF and TGF‑β induced an increase of activity in both parts of the sensory path. This suggests strengthening efects of EMF and TGF‑β on the insect ability to recognize stimuli after one cercus ablation. Data from locomotor tests proved electrophysiological results. The takeover of the function of one cercus by the second one proves the existence of compensatory plasticity in the cockroach escape system, which makes it a good model for studying compensatory plasticity. We recommend further research on EMF as a useful factor in neurorehabilitation. Injuries in the nervous system caused by acute trauma, neurodegenerative diseases or even old age are hard to reverse and represent an enormous challenge for modern medicine. -
Auditory System & Hearing
Auditory System & Hearing Chapters 9 part II Lecture 17 Jonathan Pillow Sensation & Perception (PSY 345 / NEU 325) Fall 2017 1 Cochlea: physical device tuned to frequency! • place code: tuning of different parts of the cochlea to different frequencies 2 The auditory nerve (AN): fibers stimulated by inner hair cells • Frequency selectivity: Clearest when sounds are very faint 3 Threshold tuning curves for 6 neurons (threshold = lowest intensity that will give rise to a response) Characteristic frequency - frequency to which the neuron is most sensitive threshold(dB) frequency (kHz) 4 Information flow in the auditory pathway • Cochlear nucleus: first brain stem nucleus at which afferent auditory nerve fibers synapse • Superior olive: brainstem region thalamus MGN in the auditory pathway where inputs from both ears converge • Inferior colliculus: midbrain nucleus in the auditory pathway • Medial geniculate nucleus (MGN): part of the thalamus that relays auditory signals to the cortex 5 • Primary auditory cortex (A1): First cortical area for processing audition (in temporal lobe) • Belt & Parabelt areas: areas beyond A1, where neurons respond to more complex characteristics of sounds 6 Basic Structure of the Mammalian Auditory System Comparing overall structure of auditory and visual systems: • Auditory system: Large proportion of processing before A1 • Visual system: Large proportion of processing after V1 7 Basic Structure of the Mammalian Auditory System Tonotopic organization: neurons organized spatially in order of preferred frequency • -

Sensory Change Following Motor Learning
A. M. Green, C. E. Chapman, J. F. Kalaska and F. Lepore (Eds.) Progress in Brain Research, Vol. 191 ISSN: 0079-6123 Copyright Ó 2011 Elsevier B.V. All rights reserved. CHAPTER 2 Sensory change following motor learning { k { { Andrew A. G. Mattar , Sazzad M. Nasir , Mohammad Darainy , and { } David J. Ostry , ,* { Department of Psychology, McGill University, Montréal, Québec, Canada { Shahed University, Tehran, Iran } Haskins Laboratories, New Haven, Connecticut, USA k The Roxelyn and Richard Pepper Department of Communication Sciences and Disorders, Northwestern University, Evanston, Illinois, USA Abstract: Here we describe two studies linking perceptual change with motor learning. In the first, we document persistent changes in somatosensory perception that occur following force field learning. Subjects learned to control a robotic device that applied forces to the hand during arm movements. This led to a change in the sensed position of the limb that lasted at least 24 h. Control experiments revealed that the sensory change depended on motor learning. In the second study, we describe changes in the perception of speech sounds that occur following speech motor learning. Subjects adapted control of speech movements to compensate for loads applied to the jaw by a robot. Perception of speech sounds was measured before and after motor learning. Adapted subjects showed a consistent shift in perception. In contrast, no consistent shift was seen in control subjects and subjects that did not adapt to the load. These studies suggest that motor learning changes both sensory and motor function. Keywords: motor learning; sensory plasticity; arm movements; proprioception; speech motor control; auditory perception. Introduction the human motor system and, likewise, to skill acquisition in the adult nervous system. -

Audiology and Hearing Aid Services
For more information, call the Hearing Aid Services office nearest you: Comprehensive hearing aid related services Barbourville Bowling Green are available to children diagnosed with (800) 348-4279 (800) 843-5877 permanent childhood hearing loss (PCHL). (606) 546-5109 (270) 746-7816 Elizabethtown Hazard Who should be referred to the OCSHCN (800) 995-6982 (800) 378-3357 Hearing Aid Services program? (270) 766-5370 (606) 435-6167 Children who are in need of new or Lexington Louisville replacement hearing aids and want to (800) 817-3874 (800) 232-1160 receive hearing aids and related services (859) 252-3170 (502) 429-4430 through a OCSHCN audiologist and wish to Morehead Owensboro receive Otology care outside of the (800) 928-3049 (877) 687-7038 clinical Otology program. (606) 783-8610 (270) 687-7038 What audiology services are available Paducah Prestonsburg (800) 443-3651 (800) 594-7058 through the OCSHCN Hearing Aid Services (270) 443-3651 (606) 889-1761 program? Licensed, certified audiologists conduct Somerset (800) 525-4279 periodic comprehensive hearing evaluations, (606) 677-4120 hearing aid checks, hearing aid repairs and Audiology and hearing aid evaluations according to ASHA best practices guidelines. Comprehensive Kentucky Cabinet for Health and Family Services Hearing Aid Services Office for Children with Special Health Care Needs reports are provided to the managing 310 Whittington Parkway, Suite 200, Louisville, KY 40222 otolaryngologist on an on-going basis; Phone: (502) 429-4430 or (800) 232-1160 FAX: (502) 429-4489 additional follow up testing will be http://chfs.ky.gov/agencies/ccshcn Information for Parents and Equal Opportunity Employer M/D/F completed at physician request. -

Anatomy of the Ear ANATOMY & Glossary of Terms
Anatomy of the Ear ANATOMY & Glossary of Terms By Vestibular Disorders Association HEARING & ANATOMY BALANCE The human inner ear contains two divisions: the hearing (auditory) The human ear contains component—the cochlea, and a balance (vestibular) component—the two components: auditory peripheral vestibular system. Peripheral in this context refers to (cochlea) & balance a system that is outside of the central nervous system (brain and (vestibular). brainstem). The peripheral vestibular system sends information to the brain and brainstem. The vestibular system in each ear consists of a complex series of passageways and chambers within the bony skull. Within these ARTICLE passageways are tubes (semicircular canals), and sacs (a utricle and saccule), filled with a fluid called endolymph. Around the outside of the tubes and sacs is a different fluid called perilymph. Both of these fluids are of precise chemical compositions, and they are different. The mechanism that regulates the amount and composition of these fluids is 04 important to the proper functioning of the inner ear. Each of the semicircular canals is located in a different spatial plane. They are located at right angles to each other and to those in the ear on the opposite side of the head. At the base of each canal is a swelling DID THIS ARTICLE (ampulla) and within each ampulla is a sensory receptor (cupula). HELP YOU? MOVEMENT AND BALANCE SUPPORT VEDA @ VESTIBULAR.ORG With head movement in the plane or angle in which a canal is positioned, the endo-lymphatic fluid within that canal, because of inertia, lags behind. When this fluid lags behind, the sensory receptor within the canal is bent. -

Sensory Overamplification in Layer 5 Auditory Corticofugal Projection Neurons Following Cochlear Nerve Synaptic Damage
Corrected: Publisher correction ARTICLE DOI: 10.1038/s41467-018-04852-y OPEN Sensory overamplification in layer 5 auditory corticofugal projection neurons following cochlear nerve synaptic damage Meenakshi M. Asokan1,2, Ross S. Williamson1,3, Kenneth E. Hancock1,3 & Daniel B. Polley1,2,3 Layer 5 (L5) cortical projection neurons innervate far-ranging brain areas to coordinate integrative sensory processing and adaptive behaviors. Here, we characterize a plasticity in 1234567890():,; L5 auditory cortex (ACtx) neurons that innervate the inferior colliculus (IC), thalamus, lateral amygdala and striatum. We track daily changes in sound processing using chronic widefield calcium imaging of L5 axon terminals on the dorsal cap of the IC in awake, adult mice. Sound level growth functions at the level of the auditory nerve and corticocollicular axon terminals are both strongly depressed hours after noise-induced damage of cochlear afferent synapses. Corticocollicular response gain rebounded above baseline levels by the following day and remained elevated for several weeks despite a persistent reduction in auditory nerve input. Sustained potentiation of excitatory ACtx projection neurons that innervate multiple limbic and subcortical auditory centers may underlie hyperexcitability and aberrant functional coupling of distributed brain networks in tinnitus and hyperacusis. 1 Eaton-Peabody Laboratories, Massachusetts Eye and Ear Infirmary, Boston, MA 02114, USA. 2 Division of Medical Sciences, Harvard University, Boston, MA 02114, USA. 3 Department of Otolaryngology, Harvard Medical School, Boston, MA 02114, USA. Correspondence and requests for materials should be addressed to M.M.A. (email: [email protected]) NATURE COMMUNICATIONS | (2018) 9:2468 | DOI: 10.1038/s41467-018-04852-y | www.nature.com/naturecommunications 1 ARTICLE NATURE COMMUNICATIONS | DOI: 10.1038/s41467-018-04852-y he auditory system employs a variety of gain control to the IC and striatum33 or both to the IC and brainstem34). -

Shopping Wisely for Hearing Aids
Consumer’s Edge Consumer Protection Division, Maryland Office of the Attorney General Brian E. Frosh, Maryland Attorney General Listen Up! Shopping Wisely for Hearing Aids Evelyn spent $2,300 for hearing aids but they did not your problem is diagnosed properly, since a hearing loss improve her ability to hear. Although she informed the may be a symptom of a more serious medical condition. seller, he repeatedly insisted she simply needed more time to get used to them. The sales contract didn’t in- A hearing aid seller is required by federal law to inform clude the 30-day notice of cancellation as required by you that it is in your best interest to have a medical exam law. After contacting the Attorney General’s Consumer by a licensed physician. In fact, your hearing must be Protection Division, she was able to get a refund. evaluated by a doctor before you buy a hearing aid, unless you sign a statement saying you’ve waived that protection. Don’t sign it. It’s always wise to have a medical evaluation to make sure all medically treatable conditions that may affect your hearing are identified and treated before you purchase a hearing aid. What kind of doctor should you see to have your hearing evaluated? The U.S. Food and Drug Administration recom- mends an ear, nose and throat specialist (otolaryngologist), an ear specialist (otologist) or any licensed physician. Look for the right seller. Once your doctor confirms you need a hearing aid, you’ll need a hearing aid evaluation. Hearing aids can be difficult to fit, often requiring several adjustments. -

Molecular Mechanisms of Mechanotransduction in Mammalian Sensory Neurons
REVIEWS Molecular mechanisms of mechanotransduction in mammalian sensory neurons Patrick Delmas, Jizhe Hao and Lise Rodat-Despoix Abstract | The somatosensory system mediates fundamental physiological functions, including the senses of touch, pain and proprioception. This variety of functions is matched by a diverse array of mechanosensory neurons that respond to force in a specific fashion. Mechanotransduction begins at the sensory nerve endings, which rapidly transform mechanical forces into electrical signals. Progress has been made in establishing the functional properties of mechanoreceptors, but it has been remarkably difficult to characterize mechanotranducer channels at the molecular level. However, in the past few years, new functional assays have provided insights into the basic properties and molecular identity of mechanotransducer channels in mammalian sensory neurons. The recent identification of novel families of proteins as mechanosensing molecules will undoubtedly accelerate our understanding of mechanotransduction mechanisms in mammalian somatosensation. mechanoreceptors Mechanoreceptor The ability of living organisms to perceive mechanical The ability of to detect mechanical A sensory receptor that forces is crucial for interacting with the physical world. cues relies on the presence of mechanotranducer channels responds to mechanical Mechanotransduction, the conversion of a mechanical on sensory nerve endings that rapidly transform pressure or distortion by causing stimulus into a biological response, constitutes the basis mechanical forces into electrical signals and depolarize membrane depolarization and action potential firing. of fundamental physiological processes, such as the the receptive field; this local depolarization, called the senses of touch, balance, proprioception and hearing, receptor potential, can generate action potentials that Mechanotransducer channel and makes a vital contribution to homeostasis. propagate towards the CNS. -
Auditory System
Auditory System Slides adapted from Rutgers University (http://qneuro.rutgers.edu ) and Imperial college (http://www.doc.ic.ac.uk/~phwl/teaching/mm/Index.html) The Nature of Sound (P. 149) Sound as mechanical wave energy requires a medium such as air or water in which to move. Sound: vibratory energy caused by movement of physical objects • Rate of vibration is called frequency – What we hear is pitch (high or low) – We hear 20-20,000 Hz (cycles/sec) • Size (intensity) of vibration is amplitude – What we experience is loudness – Measured in decibels (dB) (too loud too long = hearing loss) Frequency - A The number of sound pulses that travel past a fixed point within a second. A is a lower frequency sound than B. Unit is Hz. B Speed of Sound - How fast sound pulse travels. All sound travels at the same speed in a given medium In air, the speed of sound is 344 m/S. Species - Frequency Range Pitch. This is perception. A Humans 20 - 20,000 Hz high frequency sound is heard Bats 100,000 Hz as a high pitch. Any sound can be broken down into component frequencies Frequency Time The word “butter” Auditory Response Area Hearing occurs between the hearing threshold or audibility curve (at bottom) and the threshold for pain (at top). Tones below the audibility curve cannot be heard. Note that a 10 dB tone of low or very Equal Loudness curves From “Loudness: Its Definition, high frequency Measurement and Calculation,” by H. indicate tones of different Fletcher and W. A. Munson, 1933, cannot be heard. -
Mechanoreception
Mechanoreception Introduction Hair cells : the basic mechanosensory unit Hair cell structure Inner ear and accessory organ structures Vestibule Otolith organs Weberian ossicles Lateral line Lateral line structure Receptor organs Acoustic communication: sound production and reception Sound production mechanisms Locomotion and posture Introduction A mechanoreceptor is a sensory receptor that responds to mechanical pressure or distortion. In fishes mechanoreception concerns the inner ear and the lateral line system. Hair cells are the UNIVERSAL MECHANOSENSORY TRANSDUCERS in both the lateral line and hearing systems. The INNER EAR is responsible for fish EQUILIBRIUM, BALANCE and HEARING LATERAL LINE SYSTEM detects DISTURBANCES in the water. Hair cell structure EACH HAIR CELL CONSISTS OF TWO TYPES OF "HAIRS" OR RECEPTOR PROCESSES: Many microvillar processes called STEREOCILIA. One true cilium called the KINOCILLIUM. COLLECTIVELY, the cluster is called a CILIARY BUNDLE. The NUMBER OF STEREOCILIA PER BUNDLE IS VARIABLE, and ranges from a 10s of stereocilia to more than a 100. The STEREOCILIA PROJECT into a GELATINOUS CUPULA ON THE APICAL (exposed) SURFACE of the cell. The cilium and villi are ARRANGED IN A STEPWISE GRADATION - the longest hair is the kinocillium, and next to it, the stereocilia are arranged in order of decreasing length. These cells SYNAPSE WITH GANGLION CELLS. They have DIRECTIONAL PROPERTIES - response to a stimulus depends on the direction in which the hairs are bent. So, if the displacement causes the stereocilia to bend towards the kinocilium, the cell becomes DEPOLARIZED = EXCITATION. If the stereocilia bend in the opposite direction, the cell becomes HYPERPOLARIZED = INHIBITION of the cell. If the hair bundles are bent at a 90o angle to the axis of the kinocilium and stereocilia there will be no response. -

A Parent's Guide to Genetics and Hearing Loss
About 1 in 500 infants is born with or develops hearing loss during early childhood. Hearing loss has many causes: some are genetic (that is, caused by a baby’s genes) or non-genetic (such as certain infections the mother has during pregnancy, or infections the newborn baby has). A combination of genetic and non-genetic factors also can cause hearing loss. For many babies, the cause of hearing loss is unknown. This booklet answers many of the questions that families have about the causes of hearing loss, including genetic causes. For some of the topics, more extensive details are given in the shaded boxes. 1 About The Causes of Hearing Loss What are the types of hearing loss? There are many different ways to talk about the different types of hearing loss. o One way is based on whether or not a baby is born with hearing loss. If the baby is born with hearing loss it is called congenital. If the hearing loss occurs after the baby is born it is called acquired. o Another way depends on whether or not the hearing loss gets worse over time. Hearing loss that gets worse over time is called progressive. Hearing loss that does not change is called non-progressive. o A third way depends on whether or not other symptoms are present; that is, is it syndromic or non-syndromic. o A fourth way depends on whether or not hearing loss runs in the family. If it does, it is called familial; if it does not it is sporadic o A fifth way is based on where in the ear the hearing loss occurs. -

Balance Disorders
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES ∙ National Institutes of Health NIDCD Fact Sheet | Hearing and Balance Balance Disorders What is a balance disorder? Structures of the balance system inside the inner ear A balance disorder is a condition that makes you feel unsteady or dizzy. If you are standing, sitting, or lying down, you might feel as if you are moving, spinning, or floating. If you are walking, you might suddenly feel as if you are tipping over. Everyone has a dizzy spell now and then, but the term “dizziness” can mean different things to different people. For one person, dizziness might mean a fleeting feeling of faintness, while for another it could be an intense sensation of spinning (vertigo) that lasts a long time. Experts believe that more than four out of 10 Americans, sometime in their lives, will experience an episode of dizziness significant enough to send them to a doctor. Balance disorders can be caused by certain health conditions, medications, or a problem in the inner ear or the brain. A balance disorder can profoundly impact daily activities and cause Credit: NIH Medical Arts psychological and emotional hardship. } Dizziness or vertigo (a spinning sensation) What are the symptoms of a balance disorder? } Falling or feeling as if you are going to fall } Lightheadedness, faintness, or a floating sensation If you have a balance disorder, you may stagger when you try to walk, or teeter or fall when you try to stand } Blurred vision up. You might experience other symptoms such as: } Confusion or disorientation. NIDCD...Improving the lives of people with communication disorders Other symptoms might include nausea and When you turn your head, fluid inside the vomiting, diarrhea, changes in heart rate and semicircular canal moves, causing the cupula to blood pressure, and fear, anxiety, or panic.