Amtrak Passenger Train 501 Derailment Dupont, Washington December 18, 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Venture Trainsets Redefining the Intercity Rail Experience
Venture Trainsets Redefining the intercity rail experience usa.siemens.com/mobility Venture Trainsets | Mobility Next generation rail, built for North America. With our latest, intercity trainset, Built, tested, and proven Siemens is redefining what intercity rail While designed and built for tomorrow, the can be. It’s an unsurpassed passenger Venture trainsets are a proven product. Our experience that’s also raising the bar for vehicles are in use throughout North America efficiency with service-proven vehicles and have been built on a tested and designed for tomorrow and in production service-proven platform. Benefiting from today. In short, the Venture is a 21st century decades of experience in North America, trainset that’s being embraced by passengers, we’ve developed them to meet the unique operators, and agencies alike. needs of the market. All vehicles are designed and validated in accordance with FRA Riders will enjoy new levels of comfort and regulations, APTA standards and PRIIA 305 convenience along with the latest amenities. specifications for next generation equipment. The Venture features spacious interiors and flexibility for multiple configurations of First in safety economy, business, cafe and cab cars. Providing the most protection for the riding Integrated crash energy management public is our top priority. That’s why Venture provides next generation safety. trainsets feature the safest rail car design on Reduce operating costs and enhance the market. All carbodies incorporate Crash sustainability with the clean and green Energy Management (CEM) crumple zones Charger diesel-electric locomotive. Light to absorb energy at both ends of the car. and powerful, it delivers maximum Our design also includes a controlled performance and reliability up to collapse feature to enhance safety in the 125 mph. -

The Signal Bridge
THE SIGNAL BRIDGE Volume 18 NEWSLETTER OF THE MOUNTAIN EMPIRE MODEL RAILROADERS CLUB Number 5B MAY 2011 BONUS PAGES Published for the Education and Information of Its Membership NORFOLK & WESTERN/SOUTHERN RAILWAY DEPOT BRISTOL TENNESSEE/VIRGINIA CLUB OFFICERS LOCATION HOURS President: Secretary: Newsletter Editor: ETSU Campus, Business Meetings are held the Fred Alsop Donald Ramey Ted Bleck-Doran: George L. Carter 3rd Tuesday of each month. Railroad Museum Meetings start at 7:00 PM at Vice-President: Treasurer: Webmaster: ETSU Campus, Johnson City, TN. John Carter Duane Swank John Edwards Brown Hall Science Bldg, Room 312, Open House for viewing every Saturday from 10:00 am until 3:00 pm. Work Nights each Thursday from 5:00 pm until ?? APRIL 2011 THE SIGNAL BRIDGE Page 2 APRIL 2011 THE SIGNAL BRIDGE Page 3 APRIL 2011 THE SIGNAL BRIDGE II scheme. The "stripe" style paint schemes would be used on AMTRAK PAINT SCHEMES Amtrak for many more years. From Wikipedia, the free encyclopedia Phase II Amtrak paint schemes or "Phases" (referred to by Amtrak), are a series of livery applied to the outside of their rolling stock in the United States. The livery phases appeared as different designs, with a majority using a red, white, and blue (the colors of the American flag) format, except for promotional trains, state partnership routes, and the Acela "splotches" phase. The first Amtrak Phases started to emerge around 1972, shortly after Amtrak's formation. Phase paint schemes Phase I F40PH in Phase II Livery Phase II was one of the first paint schemes of Amtrak to use entirely the "stripe" style. -

Amtrak SMP 28603 Mechanical Standards for Operating Privately
Amtrak Equipment Maintenance Department Standard Maintenance Procedure SMP NO.: 28603 ISSUE DATE: January 12, 1982 REVISION DATE: September 13, 2013 TITLE: Mechanical Standard for Operating Privately Owned Cars in Amtrak Trains EQUIPMENT TYPE MAINTENANCE TYPE All Passenger Trains L – Locomotive Locomotives Cars C – Cars All Locomotives All Cars X All Types C All Maintenance – L/C Acela HST Power Car Acela Baggage Daily – L/C AEM-7 Amfleet I Cafe 30 Day – C Cab Car: (Under Cars) Amfleet II Coach Quarterly –L/C Car Movers Auto Carrier Diner Semi-Annual – L/C Commuter Commuter Dinette Annual – L/C F59PHI Freight Lounge 720 Day – L GP38-3 Heritage HEP Sleeper COT&S – C GP15D Horizon Other: Initial Terminal – L/C HHP8 Material Handling Cars Intermediate Terminal – L/C MP15 X Private Cars Modification – L/C Non Powered Control Units Superliner I Overhaul – L/C P32-8 Superliner II Running Repair – L/C P32AC-DM Surfliner Seasonal – C P-40 Talgo Wheels – L/C P-42 Turboliner Facility SW1001 Viewliner Other: SW1200 X Other: Railroad Business Cars SW1500 Turboliner Talgo Other: 1.0 PURPOSE This document describes the Amtrak Mechanical Department requirements for the handling in Amtrak trains of privately owned passenger cars, as well as railroad-owned business cars of freight carriers which have an Amtrak operating agreement. For the purpose of this document, a passenger car is defined as a vehicle meeting Association of American Railroads (AAR) or American Public Transportation Association Standard S-034 for the construction of passenger equipment cars, or similar standard for older cars, for operation in passenger train service, and does not include caboose cars, freight cars, or maintenance of way equipment. -

March 25, 2019 Volume 39
MARCH 25, 2019 ■■■■■■■■■■■ VOLUME 39 ■■■■■■■■■■ NUMBER 3 13 The Semaphore 17 David N. Clinton, Editor-in-Chief CONTRIBUTING EDITORS Southeastern Massachusetts…………………. Paul Cutler, Jr. “The Operator”………………………………… Paul Cutler III Cape Cod News………………………………….Skip Burton Boston Herald Reporter……………………… Jim South 24 Boston Globe & Wall Street Journal Reporters Paul Bonanno, Jack Foley Western Massachusetts………………………. Ron Clough Rhode Island News…………………………… Tony Donatelli “The Chief’s Corner”……………………… . Fred Lockhart Mid-Atlantic News……………………………. Doug Buchanan PRODUCTION STAFF Publication…………….………………… …. … Al Taylor Al Munn Jim Ferris Bryan Miller Web Page …………………..………………… Savery Moore Club Photographer……………………………. Joe Dumas The Semaphore is the monthly (except July) newsletter of the South Shore Model Railway Club & Museum (SSMRC) and any opinions found herein are those of the authors thereof and of the Editors and do not necessarily reflect any policies of this organization. The SSMRC, as a non-profit organization, does not endorse any position. Your comments are welcome! Please address all correspondence regarding this publication to: The Semaphore, 11 Hancock Rd., Hingham, MA 02043. ©2019 E-mail: [email protected] Club phone: 781-740-2000. Web page: www.ssmrc.org VOLUME 39 ■■■■■ NUMBER 3 ■■■■■ MARCH 2019 CLUB OFFICERS BILL OF LADING President………………….Jack Foley Vice-President…….. …..Dan Peterson Treasurer………………....Will Baker Book Review ........ ………12 Secretary……………….....Dave Clinton Chief’s Corner ...... ……. .3 Chief Engineer……….. .Fred Lockhart Contests ................ ……….3 Directors……………… ...Bill Garvey (’20) ……………………….. .Bryan Miller (‘20) Clinic……………..………3 ……………………… ….Roger St. Peter (’19) Editor’s Notes. ….….....….12 …………………………...Gary Mangelinkx (‘19) Members ............... …….....12 Memories .............. ………..4 th Potpourri ............... ..…..…..5 ON THE COVER: March 9-10 Show Running Extra....... .….……13 and Open House memories. (Photos by Joe Dumas) 2 FORM 19 ORDERS Fred Lockhart MARCH B.O.D. -
Avril by Talgo. the New Renfe High-Speed Train
Report - New high-speed train Avril by Talgo: Renfe’s new high-speed, variable gauge train On 28 November the Minister of Pub- Renfe Viajeros has awarded Talgo the tender for the sup- lic Works, Íñigo de la Serna, officially -an ply and maintenance over 30 years of fifteen high-speed trains at a cost of €22.5 million for each composition and nounced the award of a tender for the Ra maintenance cost of €2.49 per kilometre travelled. supply of fifteen new high-speed trains to This involves a total amount of €786.47 million, which represents a 28% reduction on the tender price Patentes Talgo for an overall price, includ- and includes entire lifecycle, with secondary mainte- nance activities being reserved for Renfe Integria work- ing maintenance for thirty years, of €786.5 shops. The trains will make it possible to cope with grow- million. ing demand for high-speed services, which has increased by 60% since 2013, as well as the new lines currently under construction that will expand the network in the coming and Asfa Digital signalling systems, with ten of them years and also the process of Passenger service liberaliza- having the French TVM signalling system. The trains will tion that will entail new demands for operators from 2020. be able to run at a maximum speed of 330 km/h. The new Avril (expected to be classified as Renfe The trains Class 106 or Renfe Class 122) will be interoperable, light- weight units - the lightest on the market with 30% less The new Avril trains will be twelve car units, three mass than a standard train - and 25% more energy-effi- of them being business class, eight tourist class cars and cient than the previous high-speed series. -

Transportation: Request for Passenger Rail Bonding -- Agenda Item II
Legislative Fiscal Bureau One East Main, Suite 301 • Madison, WI 53703 • (608) 266-3847 • Fax: (608) 267-6873 Email: [email protected] • Website: http://legis.wisconsin.gov/lfb October 31, 2019 TO: Members Joint Committee on Finance FROM: Bob Lang, Director SUBJECT: Department of Transportation: Request for Passenger Rail Bonding -- Agenda Item II REQUEST On October 3, 2019, the Department of Transportation (DOT) submitted a request under s. 85.061 (3)(b) of the statutes for approval to use $13,248,100 BR in GPR-supported, general obligation bonding from DOT's passenger rail route development appropriation to fund the required state match for a recently awarded Federal Railroad Administration (FRA) grant for the purchase of six single-level coach cars and three cab-coach cars to be placed into service in the Milwaukee- Chicago Hiawatha corridor. BACKGROUND DOT is required to administer a rail passenger route development program funded from a transportation fund continuing appropriation (SEG) and a general fund-supported, general obligation bonding appropriation (BR). From these sources, DOT may fund capital costs related to Amtrak service extension routes (the Hiawatha service, for example) or other rail service routes between the cities of Milwaukee and Madison, Milwaukee and Green Bay, Milwaukee and Chicago, Madison and Eau Claire, and Madison and La Crosse. Under the program, DOT is not allowed to use any bond proceeds unless the Joint Finance Committee (JFC) approves the use of the proceeds and, with respect to any allowed passenger route development project, the Department submits evidence to JFC that Amtrak, or the applicable railroad, has agreed to provide rail passenger service on that route. -

Northern Michigan Rail Ridership Feasibility and Cost Estimate Study
NORTHERN MICHIGAN RAIL RIDERSHIP FEASIBILITY AND COST ESTIMATE STUDY PREPARED FOR: The Groundwork Center For Resilient Communities Grant Fiduciary: Bay Area Transportation Authority PREPARED BY: Transportation Economics & Management Systems, Inc. OCTOBER 2018 FINAL REPORT This page intentionally left blank NORTHERN MICHIGAN RAIL RIDERSHIP FEASIBILITY AND COST ESTIMATE STUDY About the Groundwork Center for Resilient Communities The Groundwork Center for Resilient Communities works with people to build a thriving local farm and food economy; to make Michigan towns and villages stronger, more walkable, bike-able, and transit- friendly; and to develop local, clean energy. They seek to achieve on-the-ground results in northwest Michigan and leverage them to support other communities and improvements to state policy. All of this is designed to strengthen the local economy, protect the environment, and build community. Re-establishing passenger rail service between Ann Arbor, Petoskey, and Traverse City—homes to growing technology industries—will link the growing northwest with population centers in the southeast and universities along the way. Civic and business leaders believe this effort will help our state attract the next generation workforce that wants to live and thrive in Michigan without depending on a car. Groundwork believes that bringing passenger rail service back to northern Michigan is possible in less than a decade with a focused campaign of public engagement, technical analysis, and support from community, state and federal agencies. For More Information Groundwork center 148 E. Front Street, Suite 301 Traverse City, MI 49684-5725 (231) 941-6584 [email protected] Introduction October 2018 Page i NORTHERN MICHIGAN RAIL RIDERSHIP FEASIBILITY AND COST ESTIMATE STUDY This page intentionally left blank Introduction October 2018 Page ii NORTHERN MICHIGAN RAIL RIDERSHIP FEASIBILITY AND COST ESTIMATE STUDY Acknowledgements This study was prepared by Transportation Economics & Management Systems, Inc. -

Amtrak Cascades Fleet Management Plan
Amtrak Cascades Fleet Management Plan November 2017 Funding support from Americans with Disabilities Act (ADA) Information The material can be made available in an alternative format by emailing the Office of Equal Opportunity at [email protected] or by calling toll free, 855-362-4ADA (4232). Persons who are deaf or hard of hearing may make a request by calling the Washington State Relay at 711. Title VI Notice to Public It is the Washington State Department of Transportation’s (WSDOT) policy to assure that no person shall, on the grounds of race, color, national origin or sex, as provided by Title VI of the Civil Rights Act of 1964, be excluded from participation in, be denied the benefits of, or be otherwise discriminated against under any of its federally funded programs and activities. Any person who believes his/her Title VI protection has been violated, may file a complaint with WSDOT’s Office of Equal Opportunity (OEO). For additional information regarding Title VI complaint procedures and/or information regarding our non-discrimination obligations, please contact OEO’s Title VI Coordinator at 360-705-7082. The Oregon Department of Transportation ensures compliance with Title VI of the Civil Rights Act of 1964; 49 CFR, Part 21; related statutes and regulations to the end that no person shall be excluded from participation in or be denied the benefits of, or be subjected to discrimination under any program or activity receiving federal financial assistance from the U.S. Department of Transportation on the grounds of race, color, sex, disability or national origin. -
Sounder Expansion to Dupont
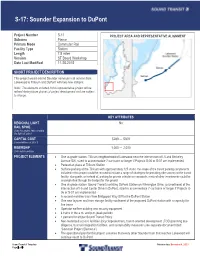
S-17: Sounder Expansion to DuPont Project Number S-17 PROJECT AREA AND REPRESENTATIVE ALIGNMENT Subarea Pierce Primary Mode Commuter Rail Facility Type Station Length 7.8 miles Version ST Board Workshop Date Last Modified 11-25-2015 SHORT PROJECT DESCRIPTION This project would extend Sounder commuter rail service from Lakewood to Tillicum and DuPont with two new stations. Note: The elements included in this representative project will be refined during future phases of project development and are subject to change. KEY ATTRIBUTES REGIONAL LIGHT No RAIL SPINE Does this project help complete the light rail spine? CAPITAL COST $289 — $309 Cost in Millions of 2014 $ RIDERSHIP 1,000 — 2,000 2040 daily boardings PROJECT ELEMENTS · One at-grade station: Tillicum neighborhood of Lakewood near the intersection of I-5 and Berkeley Avenue SW, sized to accommodate 7-car trains or longer if Projects S-06 or S-07 are implemented · Pedestrian plaza at Tillicum Station · Surface parking at the Tillicum with approximately 125 stalls; the scope of the transit parking components included in this project could be revised to include a range of strategies for providing rider access to the transit facility; along with, or instead of, parking for private vehicles or van pools, a mix of other investments could be accomplished through the budget for this project · One at-grade station: Sound Transit’s existing DuPont Station on Wilmington Drive, just northeast of the intersection of I-5 and Center Drive in DuPont, sized to accommodate 7-car trains or longer if Projects S- 06 or S-07 are implemented · A second mainline track from Bridgeport Way SW to the DuPont Station · One new layover and train storage facility southwest of the proposed DuPont station with a capacity for five trains · Operator welfare building and security equipment · 4 trains in the a.m. -

HQ-2017-1239 Final.Pdf
Federal Railroad Administration Office of Railroad Safety Accident and Analysis Branch Accident Investigation Report HQ-2017-1239 Amtrak 501 DuPont, Washington December 18, 2017 Note that 49 U.S.C. §20903 provides that no part of an accident or incident report, including this one, made by the Secretary of Transportation/Federal Railroad Administration under 49 U.S.C. §20902 may be used in a civil action for damages resulting from a matter mentioned in the report. U.S. Department of Transportation FRA File #HQ-2017-1239 Federal Railroad Administration FRA FACTUAL RAILROAD ACCIDENT REPORT SYNOPSIS On December 18, 2017, at 7:33 a.m., PST, southbound National Railroad Passenger Corporation (Amtrak) Passenger Train Number 501 (Train 501) derailed in an 8-degree, 22-minute, left-hand curve at Milepost (MP) 19.86 on the Central Puget Sound Regional Transit Authority, Sounder Commuter Rail (Sound Transit) Lakewood Subdivision, in DuPont, Washington. The lead locomotive and 12 cars derailed, with some sliding down an embankment, and some landing on the southbound lanes of Interstate 5, colliding with several highway vehicles. Train 501 is part of the Amtrak Cascades passenger train service funded by the States of Washington and Oregon. The Cascades passenger train service operates between Vancouver, British Columbia, and Eugene, Oregon, using Talgo, Inc. (Talgo) passenger equipment. DuPont, Washington, is located approximately 18 miles southwest of Tacoma, Washington. Sound Transit is the host railroad to Amtrak on the Lakewood Subdivision, which is approximately 20 miles in length from Tacoma to DuPont. Train 501 was traveling from Seattle, Washington, to Portland, Oregon, over the Point Defiance Bypass track between Tacoma and DuPont. -

Table of Contents
TABLE OF CONTENTS PAGE ABOUT US (i) FACTS ABOUT DVDs / POSTAGE RATES (ii) LOOKING AFTER YOUR DVDs (iii) Greg Scholl 1 Pentrex (Incl.Pentrex Movies) 9 ‘Big E’ 32 General 36 Electric 39 Interurban 40 Diesel 41 Steam 63 Modelling (Incl. Allen Keller) 78 Railway Productions 80 Valhalla Video Productions 83 Series 87 Steam Media 92 Channel 5 Productions 94 Video 125 97 United Kindgom ~ General 101 European 103 New Zealand 106 Merchandising Items (CDs / Atlases) 110 WORLD TRANSPORT DVD CATALOGUE 112 EXTRA BOARD (Payment Details / Producer Codes) 113 ABOUT US PAYMENT METHODS & SHIPPING CHARGES You can pay for your order via VISA or MASTER CARD, Cheque or Australian Money Order. Please make Cheques and Australian Money Orders payable to Train Pictures. International orders please pay by Credit Card only. By submitting this order you are agreeing to all the terms and conditions of trading with Train Pictures. Terms and conditions are available on the Train Pictures website or via post upon request. We will not take responsibility for any lost or damaged shipments using Standard or International P&H. We highly recommend Registered or Express Post services. If your in any doubt about calculating the P&H shipping charges please drop us a line via phone or send an email. We would love to hear from you. Standard P&H shipping via Australia Post is $3.30/1, $5.50/2, $6.60/3, $7.70/4 & $8.80 for 5-12 items. Registered P&H is available please add $2.50 to your standard P&H postal charge. -
Point Defiance Bypass Project Environmental Assessment
Point Defiance Bypass Project Environmental Assessment Prepared for: U.S. Department of Transportation Federal Railroad Administration Prepared by: For more information you can: Call the WSDOT Rail Office at (360) 705-7900 Write to the WSDOT Rail Office at WSDOT Rail Office, P.O. Box 47407 Olympia, WA 98504-7407 Fax your comments to (360) 705-6821 E-mail your comments to [email protected] Title VI Notice to Public It is the Washington State Department of Transportation's (WSDOT) policy to assure that no person shall, on the grounds of race, color, national origin or sex, as provided by Title VI of the Civil Rights Act of 1964, be excluded from participation in, be denied the benefits of, or be otherwise discriminated against under any of its federally funded programs and activities. Any person who believes his/her Title VI protection has been violated may file a complaint with WSDOT's Office of Equal Opportunity (OEO). For Title VI complaint forms and advice, please contact OEO’s Title VI Coordinators, George Laue at (509) 324-6018 or Jonte' Sulton at (360) 705-7082. Persons with disabilities may request this information be prepared and supplied in alternate forms by calling the WSDOT ADA Accommodations Hotline collect at (206) 389-2839. Persons with vision or hearing impairments may access the WA State Telecommunications Relay Service at TT 1-800-833-6388, Tele-Braille at 1-800-833-6385, or voice at 1-800-833- 6384, and ask to be connected to (360) 705-7097. Point Defiance Bypass Project Environmental Assessment Submitted pursuant to the National Environmental Policy Act (42 U.S.C.