General Surgery Profile
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
LIST of DOCTORS As of June 2018
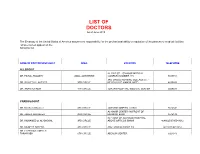
LIST OF DOCTORS As of June 2018 The Embassy of the United States of America assumes no responsibility for the professional ability or reputation of the persons or medical facilities whose names appear on the following list. NAME OF DOCTOR/SPECIALIST AREA LOCATION TELEPHONE ALLERGIST AL-RAZI ST. - SAMOOR MEDICAL DR. FAISAL TBAILEH JABAL ALHUSSEIN COMPLEX NUMBER 145 5695151 3RD CIRCLE NURSING COLLAGE ST. - DR. SAYYED AL-NATHER 3RD CIRCLE NEAR HAYAT AMMAN HOTEL 4655893 DR. ANAN ALFAQIH 4TH CIRCLE JORDAN HOSPITAL/ MEDICAL CENTER 5609031 CARDIOLOGIST DR. Munther AlSaafeen 4TH CIRCLE JORDAN HOSPITAL CLINIC 5624840 AL-KHAIR CENTER- IN FRONT OF DR. ZAHER ALKASEEH 3RD CIRCLE HOUSING BANK 4645138 IN FRONT OF ALKHALDI HOSPITAL, DR. MOHAMED O. AL-BAGGAL 3RD CIRCLE ABOVE OPTICOS SHAMI 4646625/0795543012 DR. MUNEER AREEDA 4TH CIRCLE ABU HASSAN COMPLEX 4613613/4613614 DR. HATEM SALAMEH AL- TARAWNEH 5TH CIRCLE ABDOUN CENTER 5924343 DR. AHMAD MOHANNA AL ABDOUN CENTER, INFRONT OF ARABIC HARASEES 5TH CIRCLE CENTER 5924343 DR. IMAD HADAD 4TH CIRCLE JORDAN HOSPITAL CLINIC 5626197/0795303502 DR. NAZIH NAJEH AL-QADIRI 4TH CIRCLE JORDAN HOSPITAL CLINIC 5680060/0796999695 JABER IBN HAYYAN ST./ IBN HAYYAN DR. SUHEIL HAMMOUDEH SHMEISANI MEDICAL COMPLEX 5687484/0795534966 DR. YOUSEF QOUSOUS JABAL AMMAN AL-KHALIDI ST./ AL- BAYROUNI COMP. 4650888/0795599388 CARDIOVASCULAR SURGEON JABAL AMMAN NEAR ALKHALDI DR. SUHEIL SALEH 3RD CIRCLE HOSPITAL 4655772 / 079-5533855 COLORECTAL & GENERAL SURGERY DR. WAIL FATAYER KHALIDI HOSPITAL RAJA CENTER 5TH FLOOR 4633398 / 079-5525090 AL- RYAD COMP.BLDG NO. 41/ FLOOR DR. MARWAN S. RUSAN KHALIDI HOSPITAL ST. GROUND 4655772 / 0795530049 DR. JAMAL ARDAH TLA' AL- ALI IBN AL-HAYTHAM HOSPITAL 5602780 / 5811911 DENTISTS DENTAL CONSULTATION CENTER MAKA ST. -

CV-Summer 2017.Pdf
CURRICULUM VITAE NAME: MARY THERESE KILLACKEY, MD OFFICE ADDRESS: 1430 Tulane Avenue New Orleans, LA 70112 t 504.988.2317 f 504.988.1874 [email protected] PLACE OF BIRTH: Yonkers, NY EDUCATION: 1990-1994 Columbia College, Columbia University New York, NY, B.A. (Biology) 1994-1998 College of Physicians & Surgeons, Columbia University New York, NY M.D. POST-GRADUATE TRAINING: 6/1998-6/1999 Intern, General Surgery Strong Memorial Hospital University of Rochester Rochester, NY 6/1999-6/2003 Resident, General Surgery Strong Memorial Hospital University of Rochester Rochester, NY 7/2003-6/2005 Fellow, Abdominal Organ Transplant Surgery Recanati/Miller Transplant Institute The Mount Sinai Hospital New York, NY 11/2010 Leadership Development Program American Society of Transplant Surgeons Northwestern University Kellogg School of Management Chicago, IL 6/2015 Surgeons as Leaders Course American College of Surgeons Chicago, IL 9/2015-8/2016 Clinical Leadership Development Program Tulane School of Medicine, Office of the Dean New Orleans, LA 12/2015 Mid-Career Women Faculty Professional Development Seminar Association of American Medical Colleges Austin, TX 6/2016 Being a Resilient Leader Association of American Medical Colleges Washington, DC 6/2017 - 4/2018 Fellow, Executive Leadership in Academic Medicine Drexel University College of Medicine Philadelphia, PA ACADEMIC APPOINTMENTS: 7/2003-6/2005 Instructor in Surgery Mount Sinai School of Medicine New York, NY 10/2006-present Assistant Professor of Surgery and Pediatrics Tulane University -
Partnering with Your Transplant Team the Patient’S Guide to Transplantation
Partnering With Your Transplant Team The Patient’s Guide to Transplantation U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Health Resources and Services Administration This booklet was prepared for the Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation by the United Network for Organ Sharing (UNOS). PARTNERING WITH YOUR TRANSPLANT TEAM THE PATIENT’S GUIDE TO TRANSPLANTATION U.S. Department of Health and Human Services Health Resources and Services Administration Public Domain Notice All material appearing in this document, with the exception of AHA’s The Patient Care Partnership: Understanding Expectations, Rights and Responsibilities, is in the public domain and may be reproduced without permission from HRSA. Citation of the source is appreciated. Recommended Citation U.S. Department of Health and Human Services (2008). Partnering With Your Transplant Team: The Patient’s Guide to Transplantation. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. DEDICATION This book is dedicated to organ donors and their families. Their decision to donate has given hundreds of thousands of patients a second chance at life. CONTENTS Page INTRODUCTION.........................................................................................................................1 THE TRANSPLANT EXPERIENCE .........................................................................................3 The Transplant Team .......................................................................................................................4 -

General Surgery
- 1 - KALEIDA HEALTH Name: ___________________________________ Date: ____________________________ DELINEATION OF PRIVILEGES - GENERAL SURGERY PLEASE NOTE: Please check the box for each privilege requested. Do not use an arrow or line to make selections. We will return applications that ignore this directive. GENERAL STATEMENTS - Privileges in Adult Surgery are separated into the following divisions: General Surgery and Plastic Surgery. Applicants desiring procedure privileges in more than one division must complete separate forms for each. Procedures designated with an asterisk (*) indicate that Moderate or Deep Sedation may be required. If you do not have Moderate or Deep Sedation privileges, you must invite a Kaleida Health anesthesiologist to participate in the procedure. Procedures are also separated into levels of complexity (Level I-A, Level I-B, Level I, Level II, and Level III), which require increasing levels of education and experience. In general, procedures learned during residency are grouped in Level I-A or Level I and are granted upon evidence of successful completion of residency training. Level II procedures may or may not require evidence of additional training beyond residency. Documentation of additional training and/or experience is required for all Level III procedures. LEVEL I-A PRIVILEGES Procedures which involve primarily wound care, can be done under local anesthetic and occasionally involve application of temporary skin coverage or application of agents to expedite wound healing. Can be performed by any competent -

General Surgery Career Resource
The American Journal of Surgery (2013) 206, 719-723 Association of Women Surgeons: Career Development Resources General surgery career resource Ana M. Parsee, M.D.a, Sharona B. Ross, M.D.b, Nancy L. Gantt, M.D.c, Kandace Kichler, M.D.d, Celeste Hollands, M.D.e,* aJohns Hopkins Hospital, Baltimore, MD, USA; bFlorida Hospital, Tampa, FL, USA; cNortheast Ohio Medical University, St. Elizabeth Health Center, Rootstown, OH, USA; dUniversity of Miami, Palm Beach Regional Campus, Palm Beach, FL, USA; eSt John’s Children’s Hospital, Springfield, IL, USA KEYWORDS: Abstract General surgery residency training can lead to a rewarding career in general surgery and General surgery; serve as the foundation for careers in several surgical subspecialties. It offers broad-based training with General surgery exposure to the cognitive and technical aspects of several surgical specialties and prepares graduating residency; residents for a wide range of career paths. This career development resource discusses the training as- Surgical fellowship; pects of general surgery. Surgical subspecialties; Ó 2013 Elsevier Inc. All rights reserved. Transition to practice; Surgery interest groups General surgery training provides the foundation for who enter medical school with an interest in surgery and many different surgical career paths. The training begins those who become interested early can become involved with a general surgery residency, which is usually followed in their schools’ surgery interest group (SIGs) as early as by either entry into practice or additional training. General the first day of medical school at most institutions. Each surgery residency programs provide broad-based training local SIG has different offerings to help students explore with exposure to the cognitive and technical aspects of and develop their interest in surgery as a career. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Posterior Cervical Discectomy: an Optimally Invasive Approach to Laterally Prolapsed Cervical Disc
Original Research Article DOI: 10.18231/2455-8451.2016.0005 Posterior cervical discectomy: An optimally invasive approach to laterally prolapsed cervical disc Shashank Sah1,*, Suresh Kumar Kaushik2, Neeraj Prajapati3 1Associate Professor, Dept. of General Surgery, 2Associate Professor, Dept. of Orthopaedics, 3Associate Professor, Dept. of Radiology, SRMSIMS, Bareilly, Uttar Pradesh *Corresponding Author: Email: [email protected] Abstract Aim: Posterior cervical discectomy is one of the surgical techniques for management of laterally prolapsed cervical disc causing cervical radiculopathy. This method has remained under-utilized in comparison to the classic technique of Anterior Cervical Discectomy and Fusion (ACDF). The study was conducted to evaluate it’s feasibility in terms of ease, challenges and short term outcome. Material and Methods: This is a prospective study conducted over a period of 65 months. Patients visiting to neurosurgery/ orthopedics OPD’s with cervical disc diseases and requiring surgery, were further evaluated on the basis of selection criteria for the feasibility of posterior cervical discectomy. Patients meeting the selection criteria were then operated upon by this approach and the outcome was evaluated. Results: Posterior cervical discectomy is essentially a disc conserving, optimally invasive microscopic technique - best suited for selected subset of patients with laterally prolapsed disc causing radiculopathy. 21 out of 23 patients appreciated the surgical benefit by as early as 48 hours of operation. There were no complications. Conclusion: Posterior cervical discectomy is an excellent direct approach to the diseased segment provided case selection criteria are properly followed. Keywords: Cervical disc, Posterior cervical discectomy, Lamino-foraminotomy, Motion preserving cervical disc surgery Introduction approach has largely remained underutilized and Cervical disc disease is a prevalent and disabling therefore in the present study we evaluated this disorder. -

Surgical Oncology 3 PGY3
Stanford University General Surgery Residency Program Surgical Oncology 3 / Endocrine Surgery Rotation Goals and Objectives Rotation Director: Dana Lin, MD Description The Surgical Oncology 3 / Endocrine Surgery rotation offers an intensive experience in the surgical care of patients with endocrine diseases as well as breast cancer and melanoma. Goals The goal of the Surgical Oncology 3 / Endocrine Surgery rotation is to: Gain the knowledge and experience in the evaluation and management of patients with endocrine diseases, breast cancer, and melanoma. The primary goals for the R-3 resident: Develop knowledge and experience in the evaluation and management of patients with endocrine diseases, breast cancer, and melanoma. Acquire and refine procedural and operative skills required in the care of these patients. Direct the post-operative / in-patient care of the patients on the service. Objectives The Surgical Oncology 3/ Endocrine Surgery R-3 rotation has the following objectives: The resident has primary responsibility for the management of all patients admitted to or evaluated by the team in conjunction with the attending surgeon. The R-3 gains knowledge of surgical care through discussion with and teaching from the attending physicians in the inpatient and outpatient setting, attendance at the multidisciplinary endocrine tumor board conference, as well as independent reading. The resident gains operative skills through pre-operative reading and preparation and by direct intra-operative teaching and guidance from the faculty. Residents can expect frequent teaching from members of the team, both at the bedside and during formal and informal sessions. Feedback and teaching is individualized to the needs of the residents. -

DR. GONZALO SAPISOCHIN Assistant Professor of Surgery UHN, Multi-Organ Transplant and HPB Surgical Oncology Division of General Surgery
DR. GONZALO SAPISOCHIN Assistant Professor of Surgery UHN, Multi-Organ Transplant and HPB Surgical Oncology Division of General Surgery Dr. Gonzalo Sapisochin is Staff Hepatobiliary and Transplant Surgeon at The Toronto General Hospital, University Health Network in Canada. Dr. Sapisochin received his Medical Diploma in 2005 from the Universidad Complutense de Madrid, Spain and went on to complete his General Surgery residency training in 2011 at the University Hospital of Vall d’Hebron in Barcelona where he successfully defended his Doctoral Thesis, “Optimization of Liver Transplantation for Hepatocellular Carcinoma”, to receive his PhD be the Universidad Autonoma de Barcelona. He went on to complete his Clinical Fellowship Hepatobiliary Surgical Oncology & Abdominal Transplant with the University of Toronto and was subsequently recruited in a position at the Toronto General Hospital as Staff Surgeon with the Division of General Surgery. He began his new job and tenure as Assistant Professor, Department of Surgery at the University of Toronto on January 1, 2016. Dr. Sapisochin main research interest is the “interface” between liver transplantation and cancer. He has focused his research in the management of hepatocellular carcinoma, cholangiocarcinoma and colorectal liver metastases. Dr. Sapisochin has over 65 publications in peer reviewed journals. He has several publications in the field of transplant oncology in journals such as Hepatology, Annals of Surgery, Journal of Hepatology and Annals of Surgical Oncology. Currently he is the PI of clinical trials for liver transplantation for colorectal liver metastasis and intrahepatic cholangiocarcinoma. Dr. Sapisochin is developing new protocols and improving surgical management for patients with liver cancers. Motto – Optimizing liver transplantation as a treatment of cancer . -

ACGME Specialties Requiring a Preliminary Year (As of July 1, 2020) Transitional Year Review Committee
ACGME Specialties Requiring a Preliminary Year (as of July 1, 2020) Transitional Year Review Committee Program Specialty Requirement(s) Requirements for PGY-1 Anesthesiology III.A.2.a).(1); • Residents must have successfully completed 12 months of IV.C.3.-IV.C.3.b); education in fundamental clinical skills in a program accredited by IV.C.4. the ACGME, the American Osteopathic Association (AOA), the Royal College of Physicians and Surgeons of Canada (RCPSC), or the College of Family Physicians of Canada (CFPC), or in a program with ACGME International (ACGME-I) Advanced Specialty Accreditation. • 12 months of education must provide education in fundamental clinical skills of medicine relevant to anesthesiology o This education does not need to be in first year, but it must be completed before starting the final year. o This education must include at least six months of fundamental clinical skills education caring for inpatients in family medicine, internal medicine, neurology, obstetrics and gynecology, pediatrics, surgery or any surgical specialties, or any combination of these. • During the first 12 months, there must be at least one month (not more than two) each of critical care medicine and emergency medicine. Dermatology III.A.2.a).(1)- • Prior to appointment, residents must have successfully completed a III.A.2.a).(1).(a) broad-based clinical year (PGY-1) in an emergency medicine, family medicine, general surgery, internal medicine, obstetrics and gynecology, pediatrics, or a transitional year program accredited by the ACGME, AOA, RCPSC, CFPC, or ACGME-I (Advanced Specialty Accreditation). • During the first year (PGY-1), elective rotations in dermatology must not exceed a total of two months. -

100 Years. 100 Facts
100 Years. 100 Facts. Celebrating 100 Years as the United Voice of Ohio Hospitals 1819 Daniel Drake obtains a charter for the Medical 001 College of Ohio, the forerunner of the University of Cincinnati College of Medicine. 100 Years. 100 Facts. | 3 1823 Ohio’s first hospital, the Cincinnati Commercial 002 Hospital and Lunatic Asylum, opens. 4 | Ohio Hospital Association 100 Years. 100 Facts. | 5 Starling Medical Center College/Saint 003 Francis Hospital is established on the 1849 present site of Grant Medical Center in Columbus as the first teaching hospital in the U.S. It is the forerunner for the College of Medicine at Ohio State University. 6 | Ohio Hospital Association Charity Hospital Medical Center, now 004 St. Vincent Charity Hospital, opens 1873 Cleveland’s first amphitheater for demonstration of surgery and clinical procedures. 100 Years. 100 Facts. | 7 8 | Ohio Hospital Association 1886 Mother M. Angela and Sister M. Rufina Dunn, of the 005 Congregation of the Sisters of the Holy Cross of Notre Dame, Indiana, convert a sturdy four-story red brick building to two wards, 18 private rooms and an operating room with an amphitheater. The facility is called Hawkes Hospital of Mount Carmel and eventually becomes Mount Carmel West. 100 Years. 100 Facts. | 9 A 10-bed Christ Hospital opens in 006 Cincinnati after a group of local 1889 businessmen led by James Gamble (whose prospering soap business eventually became Procter & Gamble) invited Isabella Thornburg to the city in 1888 to train deaconesses and missionaries. She soon expands beyond training to open a hospital in the west end of the city. -
Go Inside a Surgeon's Typical
HealthSigns Spring 2016 Go Inside a Surgeon’s Typical Day Top in Cancer Getting the Planet Friendly Care Picture Healthcare Earning kudos on quality More advanced imaging How we care for patients for nearly a decade tools in your community and the environment HealthSigns Spring 2016 5 10 Sustaining Going Quality Green Cancer program We’re leading the earns top national way to a healthier, award for third more sustainable time. environment. 6 11 Focused on Parking Garage Healing Near Opening General surgeon More convenient starts each day access helps with energy and patients, families endurance. and our community. 8 Easy Access to Imaging Outpatient center VISIT US ONLINE offers screenings, Stay connected to Washington Hospital at www.whhs.com diagnostics and and on Facebook. Browse our calendar of upcoming events and treatment. other happenings taking place at your community hospital. 2 | SPRING 2016 Information You Can Use MISSION STATEMENT Free, science-based diabetes education classes for people with diabetes and their families or anyone who wants to As the local Health Care District, find out more about this chronic disease affecting more our mission is to meet the than 29 million Americans. health care needs of the District Diabetes Matters residents through medical services, education and research. When: First Thursday of every month (except for July), 7 to 8 p.m. Within this scope, Washington Stay for the Diabetes Support Township Health Care District Group, 8 to 9 p.m. is committed to assuming the Location: Conrad E. Anderson, MD, Auditorium (Washington West) leadership role in improving and 2500 Mowry Ave., Fremont maintaining the health status of No registration needed.