Diagnostic Code Descriptions (ICD9) Respiratory System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Laryngitis from Reflux: Prevention for the Performing Singer
Laryngitis from Reflux: Prevention for the Performing Singer David G. Hanson, MD, FACS Jack J. Jiang, MD, PhD Laryngitis in General Laryngitis is the bane of performers and other professionals who depend on their voice for their art and livelihood. Almost every person has experienced acute laryngitis, usually associated with a viral upper- respiratory infection. Whenever there is inflammation of the vocal fold epithelium, there is an effect on voice quality and strength. Therefore, it is important to understand the factors that can cause laryngitis, especially the preventable causes of laryngitis. Laryngitis is a generic term for inflammation or irritation of the laryngeal tissues. The inflammation can be caused by any kind of injury, including infection, smoking, contact with caustic or acidic substance, allergic reaction, or direct trauma. Inflammatory response of the tissues includes leakage of fluid from blood vessels with edema or swelling, congregation of white blood cells, which release mediators of inflammation, and engorgement of the blood vessels. Most commonly laryngitis occurs from viral infection of the laryngeal epithelial lining associated with a typical cold. The viral infection is almost always quickly conquered by the body's immune system and lasts at most a few days. This kind of acute laryngitis rarely causes any long-term problem unless the vocal folds are damaged by overuse during the illness. Examination of the larynx will show whether the vocal folds are inflamed and allows some prediction of the degree of risk for damage. Other infections of the larynx are fortunately not common but include infections with bacteria and other organisms. -

Hypersensitivity Pneumonitis: Challenges in Diagnosis and Management, Avoiding Surgical Lung Biopsy
395 Hypersensitivity Pneumonitis: Challenges in Diagnosis and Management, Avoiding Surgical Lung Biopsy Ferran Morell, MD1,2 Ana Villar, MD2,3 Iñigo Ojanguren, MD2,3 Xavier Muñoz, MD2,3 María-Jesús Cruz, PhD2,3 1 Vall d’Hebron Institut de Recerca (VHIR), Barcelona, Catalonia, Spain Address for correspondence Ferran Morell, MD, Vall d’Hebron Institut 2 Ciber de Enfermedades Respiratorias (CIBERES), Barcelona, Spain de Recerca (VHIR), PasseigValld’Hebron, 119-129, 08035 Barcelona, 3 Servei de Pneumologia, Hospital Universitari Vall d’Hebron, Catalonia, Spain (e-mail: [email protected]). Barcelona, Spain Semin Respir Crit Care Med 2016;37:395–405. Abstract This review presents an update of the currently available information related to Keywords hypersensitivity pneumonitis, with a particular focus on the contribution of several ► hypersensitivity techniques in the diagnosis of this condition. The methods discussed include proper pneumonitis elaboration of a complete medical history, targeted auscultation, detection of specific ► bronchoalveolar immunoglobulin G antibodies against the most common antigens causing this disease, lavage skin tests, antigen-specific lymphocyte activation assays, bronchoalveolar lavage, and ► fi speci c inhalation cryobiopsy. Special emphasis is placed on the relevant contribution of specificinhalation challenge challenge (bronchial challenge test). Surgical lung biopsy is presented as the ultimate ► bronchial challenge recourse, to be used when the diagnosis cannot be reached through the other methods test covered. -
Hoarseness a Guide to Voice Disorders
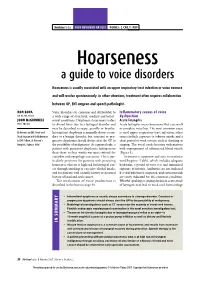
MedicineToday PEER REVIEWED ARTICLE POINTS: 2 CPD/1 PDP Hoarseness a guide to voice disorders Hoarseness is usually associated with an upper respiratory tract infection or voice overuse and will resolve spontaneously. In other situations, treatment often requires collaboration between GP, ENT surgeon and speech pathologist. RON BOVA Voice disorders are common and attributable to Inflammatory causes of voice MB BS, MS, FRACS a wide range of structural, medical and behav- dysfunction JOHN McGUINNESS ioural conditions. Dysphonia (hoarseness) refers Acute laryngitis FRCS, FDS RCS to altered voice due to a laryngeal disorder and Acute laryngitis causes hoarseness that can result may be described as raspy, gravelly or breathy. in complete voice loss. The most common cause Dr Bova is an ENT, Head and Intermittent dysphonia is normally always secon - is viral upper respiratory tract infection; other Neck Surgeon and Dr McGuinness dary to a benign disorder, but constant or pro- causes include exposure to tobacco smoke and a is ENT Fellow, St Vincent’s gressive dysphonia should always alert the GP to short period of vocal overuse such as shouting or Hospital, Sydney, NSW. the possibility of malignancy. As a general rule, a singing. The vocal cords become oedematous patient with persistent dysphonia lasting more with engorgement of submucosal blood vessels than three to four weeks warrants referral for (Figure 3). complete otolaryngology assessment. This is par- Treatment is supportive and aims to maximise ticularly pertinent for patients with persisting vocal hygiene (Table), which includes adequate hoarseness who are at high risk for laryngeal can- hydration, a period of voice rest and minimised cer through smoking or excessive alcohol intake, exposure to irritants. -

Parent's Guide to a Sore Throat
Contact your GP (or call 111) Useful contacts: again Your GP surgery on:....................................... Although in most cases the sore throat (Please insert surgery number here) improves in few days, please contact the GP if any of the following occurs: GP Out of Hours: (After 6.30pm and before 8am). Ring 111 and you can speak to a 1. Your child persistently refuses oral fl uids doctor. If necessary, your child can be seen and has not passed urine for over 18 at one of their centres. Parent’s guide hours. Bristol City Walk-in Centre at Broadmead 2. The fever does not settle within four or to a sore throat Medical Centre located in Boots fi ve days. (Mon-Sat 8am-8pm, Sundays and Bank Holidays 11am-5pm) on: 0117 954 9828 3. Your child develops diffi culty in swallowing despite regular paracetamol South Bristol NHS Community Hospital or ibuprofen. Urgent Care Centre (Every day 8am-8pm) on: 0117 342 9692 4. Your child starts drooling because they Visit www.nhs.uk to fi nd your nearest cannot swallow their saliva. centre. Call 999 If your child is seriously ill, you may be asked to attend the Children’s Hospital If your child develops severe breathing emergency department. diffi culties For further copies of this leafl et, or if you would like it in other formats or languages, please contact 0117 900 2384. Produced in partnership with Bristol Clinical Commissioning Group, North Bristol NHS Trust and University Hospitals Bristol NHS Foundation Trust. End date: June 2016 Your child has been diagnosed with a sore What is the treatment of a sore throat which is very common in children. -

Nebulizers: Diagnosis Codes – Medicare Advantage Policy Appendix
UnitedHealthcare® Medicare Advantage Policy Appendix: Applicable Code List Nebulizers: Diagnosis Codes This list of codes applies to the Medicare Advantage Policy Guideline titled Approval Date: September 8, 2021 Nebulizers. Applicable Codes The following list(s) of procedure and/or diagnosis codes is provided for reference purposes only and may not be all inclusive. The listing of a code does not imply that the service described by the code is a covered or non-covered health service. Benefit coverage for health services is determined by the member specific benefit plan document and applicable laws that may require coverage for a specific service. The inclusion of a code does not imply any right to reimbursement or guarantee claim payment. Other Policies and Guidelines may apply. Diagnosis Code Description For HCPCS Codes A7003, A7004, and E0570 A15.0 Tuberculosis of lung A22.1 Pulmonary anthrax A37.01 Whooping cough due to Bordetella pertussis with pneumonia A37.11 Whooping cough due to Bordetella parapertussis with pneumonia A37.81 Whooping cough due to other Bordetella species with pneumonia A37.91 Whooping cough, unspecified species with pneumonia A48.1 Legionnaires' disease B20 Human immunodeficiency virus [HIV] disease B25.0 Cytomegaloviral pneumonitis B44.0 Invasive pulmonary aspergillosis B59 Pneumocystosis B77.81 Ascariasis pneumonia E84.0 Cystic fibrosis with pulmonary manifestations J09.X1 Influenza due to identified novel influenza A virus with pneumonia J09.X2 Influenza due to identified novel influenza A virus with other -

Diapositivo 1
A.C. Nunes1, A. Domingues1, M. Almeida-Silva1,2, S. Viegas2, C. Viegas2 1 Escola Superior de Tecnologia e Saúde de Lisboa, Instituto Politécnico de Lisboa 2 Instituto Tecnológico e Nuclear, Instituto Superior Técnico, Universidade Técnica de Lisboa. Cork is a light, porous, impermeable material extracted from the bark of some trees. The most widely used cork is obtained from the cork tree Health Effects (Quercus suber). It is estimated that the area occupied by cork oaks in the Iberian Peninsula is around 33% in Portugal and 23% in Spain [1]. The studied articles refer two major diseases associated with this Portugal is the largest cork producing country in the world, followed by occupational setting, occupational asthma and Suberosis. Spain, and its industry is an important economical resource [2].The Occupational asthma is a disease whose origin is related to the processes used in the manufacture of cork depend on the end product to be obtained, being the production of stoppers for wine bottles the exposure to a particular factor in a workplace. Recent studies have main application. Most of the cork is stored under dark humid and identified Chrysonilia sitophila as a cause for this occupational disease moldy conditions. During the manufacturing process, workers are in the cork and logging industry [4, 5]. This fungi is a common mould exposed to an environment that is heavily contaminated with cork dust found in cork samples analyzed [6]. [3]. Due to this repeated exposure to moldy cork dust, cork workers are at risk for developing occupational lung diseases such as occupational Suberosis is the term applied to hypersensitivity pneumonitis due to asthma and Suberosis. -
Swallowing in Patients with Laryngitis
AG-2017-86 AHEADORIGINAL OF ARTICLEPRINT dx.doi.org/10.1590/S0004-2803.201800000-10 Swallowing in patients with laryngitis Isabela MODA, Hilton Marcos Alves RICZ, Lilian Neto AGUIAR-RICZ and Roberto Oliveira DANTAS Received 21/8/2017 Accepted 5/10/2017 ABSTRACT – Background – Dysphagia is described as a complaint in 32% of patients with laryngitis. Objective – The objective of this investigation was to evaluate oral and pharyngeal transit of patients with laryngitis, with the hypothesis that alteration in oral-pharyngeal bolus transit may be involved with dysphagia. Methods – Videofluoroscopic evaluation of the swallowing of liquid, paste and solid boluses was performed in 21 patients with laryngitis, 10 of them with dysphagia, and 21 normal volunteers of the same age and sex. Two swallows of 5 mL liquid bolus, two swallows of 5 mL paste bolus and two swallows of a solid bolus were evaluated in a random sequence. The liquid bolus was 100% liquid barium sulfate and the paste bolus was prepared with 50 mL of liquid barium and 4 g of food thickener (starch and maltodextrin). The solid bolus was a soft 2.2 g cookie coated with liquid barium. Durations of oral preparation, oral transit, pharyngeal transit, pharyngeal clearance, upper esophageal sphincter opening, hyoid movement and oral-pharyngeal transit were measured. All patients performed 24-hour distal esophageal pH evaluation previous to videofluoroscopy. Results – The evaluation of 24-hour distal esophageal pH showed abnormal gastroesophageal acid reflux in 10 patients. Patients showed longer oral preparation for paste bolus and a faster oral transit time for solid bolus than normal volunteers. -

Diagnostic Yield of Specific Inhalation Challenge in Hypersensitivity Pneumonitis
ERJ Express. Published on August 19, 2014 as doi: 10.1183/09031936.00060714 ORIGINAL ARTICLE IN PRESS | CORRECTED PROOF Diagnostic yield of specific inhalation challenge in hypersensitivity pneumonitis Xavier Mun˜oz1,2,3,Mo´nica Sa´nchez-Ortiz1,2, Ferran Torres4, Ana Villar1,2, Ferran Morell1,2 and Marı´a-Jesu´s Cruz1,2 Affiliations: 1Pulmonology Service, Medicine Dept, Hospital Universitari Vall d’Hebron, Universitat Auto`noma de Barcelona, Barcelona, Spain. 2CIBER Enfermedades Respiratorias (Ciberes), Spain. 3Dept of Cell Biology, Physiology and Immunology, Universitat Auto`noma de Barcelona, Barcelona, Spain. 4Biostatistics and Data Management Platform, IDIBAPS, Hospital Clinic, Biostatistics Unit, School of Medicine, Universitat Auto`noma de Barcelona, Barcelona, Spain. Correspondence: Xavier Mun˜oz, Servei de Pneumologia, Hospital Universitari Vall d’Hebron, Passeig Vall d’Hebron, 119, 08035 Barcelona, Spain. E-mail: [email protected] ABSTRACT Reliable methods are needed to diagnose hypersensitivity pneumonitis. Theaimofthestudywasto establish the diagnostic yield of specific inhalation challenge (SIC) in patients with hypersensitivity pneumonitis. All patients with suspected hypersensitivity pneumonitis in whom SIC was performed (n5113) were included. SIC was considered positive when patients showed a decrease of .15% in forced vital capacity (FVC) or .20% in diffusing capacity of the lung for carbon dioxide, or a decrease of 10% to 15% in FVC accompanied by a temperature increase of 0.5uC within 24 h of inhalation of the antigen. SIC was positive to the agents tested in 68 patients: 64 received a diagnosis of hypersensitivity pneumonitis and SIC results were considered false-positive in the remaining four patients. In the SIC- negative group (n545), 24 patients received a diagnosis of hypersensitivity pneumonitis and SIC results were considered false-negative, and 21 patients were diagnosed with other respiratory diseases. -

Download PDF File
GUIDELINES AND RECOMMENDATIONSPRACA ORYGINALNA Henryk Mazurek1, 2, Anna Bręborowicz3, Zbigniew Doniec4, Andrzej Emeryk5, Katarzyna Krenke6, Marek Kulus6, Beata Zielnik-Jurkiewicz7 1Department of Pneumonology and Cystic Fibrosis, Institute of Tuberculosis and Pulmonary Diseases, Rabka-Zdrój, Poland 2State Higher Vocational School, Nowy Sącz, Poland 3Department of Pneumonology, Pediatric Allergy and Clinical Immunology, Poznan University of Medical Science, Poznań, Poland 4Department of Pneumonology, Institute of Tuberculosis and Pulmonary Diseases, Rabka-Zdrój, Poland 5Department of Pulmonary Diseases and Children Rheumatology, Medical University of Lublin, Lublin, Poland 6Department of Pediatric Pneumonology and Allergy, Medical University of Warsaw, Warsaw, Poland 7Department of Otolaryngology, Children’s Hospital, Warsaw, Poland Acute subglottic laryngitis. Etiology, epidemiology, pathogenesis and clinical picture Abstract In about 3% of children, viral infections of the airways that develop in early childhood lead to narrowing of the laryngeal lumen in the subglottic region resulting in symptoms such as hoarseness, a barking cough, stridor, and dyspnea. These infections may eventually cause respiratory failure. The disease is often called acute subglottic laryngitis (ASL). Terms such as pseudocroup, croup syndrome, acute obstructive laryngitis and spasmodic croup are used interchangeably when referencing this disease. Although the differential diagnosis should include other rare diseases such as epiglottitis, diphtheria, fibrinous laryngitis and bacterial tracheobronchitis, the diagnosis of ASL should always be made on the basis of clinical criteria. Key words: subglottic laryngitis, croup, laryngeal obstruction, inspiratory dyspnoea, stridor Adv Respir Med. 2019; 87: 308–316 Definition and nomenclature have in common is laryngitis. However, some of them also indicate the location of the lesions In approximately 3% of children [1, 2], or their pathological background (e.g. -

The Growing Problem of Viral Respiratory Infections
The growing problem of viral respiratory infections 5th ESCMID School of Clinical Microbiology and Infectious Diseases Santander, Spain, 10 - 16 June 2006 Núria Rabella Respiratory tract Major portal of entry Most common afflictions in humans Wide range of clinical manifestations: from self-limited to devastating Children half a dozen each year, adults two or three. Most caused by viruses. Considerable impact on quality of life and productivity of society Respiratory tract Majority trivial colds and sore throats Serious lower respiratory tract infections tend to occur at the extremes of life Influenzavirus killing the elderly and respiratory syncytial virus killing the very young Altogether over 200 known viruses Respiratory tract infection High prevalence: large number of infectious agents and serotypes efficiency of transmission incomplete immunity Frequency: higher in children under 4 years Major reservoir it declines in teenagers schoolchildren rises again in parents lowest in the elderly Epidemiology (1) • Transmission: respiratory route • Shedding: sneezing, coughing or talking • sneeze: – 106 droplets < 10mm ê evaporation ê smaller- suspended in the air for several minutes – larger droplets fall to the ground • Spreading: • inhalation • direct contact Epidemiology (2) * Sneezing: 1.940.000 viral particles * To begin an infection: Adenovirus: 7 Influenza A virus: 3 Enterovirus: 6 * Some viruses remain infectious for prolonged periods Direct contact transmission Viral persistence Respiratory syncytial virus: porous surfaces for 30’ -

Occupational Lung Diseases
Occupational Lung diseases Dr Deepak Aggarwal Dept. Of Pulmonary Medicine To be discussed…. • Pneumoconiosis • Hypersensitivity Pneumonitis PNEUMOCONIOSIS Pneumoconioses are pulmonary diseases caused by mineral dust inhalation in workplace The specific types of pneumoconioses are named by the substance inhaled (e.g., silicosis, asbestosis, anthracosis) PNEUMOCONIOSIS Mineral Dust‐Induced Lung Disease Coal dust Simple coal workers' pneumoconiosis: Coal mining macules and nodules Complicated coal workers' pneumoconiosis: PMF Silica Silicosis Sandblasting, quarrying, mining, stone cutting, foundry work, ceramics Asbestos Asbestosis pleural effusions, pleural plaques, or Mining, milling, diffuse fibrosis; mesothelioma; carcinoma of the and fabrication of ores and lung and larynx materials; installation and removal of insulation Fibrogenic pneumoconioses "true pneumoconioses" • asbestosis • berylliosis • • silicosis talcosis • kaolin pneumoconiosis. • hard metal disease • coal workers' • aluminum fibrosis, pneumoconiosis Shaver's disease Non‐fibrogenic pneumoconioses benign pneumoconioses Causes: • antimony • iron • barium • tin • boric acid • titanium • manganese • bismuth PNEUMOCONIOSIS Pathogenesis The development of a pneumoconiosis depends on (1) the amount of dust retained in the lung and airways (2) the size, shape, and buoyancy of the particles (3) solubility and physiochemical reactivity (4) the possible additional effects of other irritants (e.g., concomitant tobacco smoking) PNEUMOCONIOSIS Pathogenesis (1)The amount of dust retained -

Managing Comorbidities in Ipf
Sponsored by Supported by an educational grant from “IPF Updates” Monograph Series MANAGING COMORBIDITIES IN IPF Steven A. Sahn, MD Medical University of South Carolina Charleston, South Carolina “IPF Updates” Monograph Series Managing Comorbidities in IPF CONTENTS CME Information ..................................................................................................................................... 2 Faculty and Disclosure ............................................................................................................................ 3 Managing Comorbidities in IPF ............................................................................................................... 4 References ............................................................................................................................................ 16 Attestation/Evaluation Form .................................................................................................................. 19 Posttest ................................................................................................................................................ 22 CONTENTS 1 CME INFORMATION Needs Statement/Intended Audience Commercial Support Acknowledgment This activity has been planned in accordance with the need This activity is supported by an educational grant from to provide pulmonologists and other health care providers InterMune. with a continuing medical education activity that addresses the best practices for management of patients with IPF.