Imported Malaria and Epidemiologic Components of This Infection In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Investing and Providing the Solutions to Confront The
Abstract: Today, tourism industry is considered as the largest and the most various industries in the world and many countries regard the industry as a part of their main source of income, employment, the growth of the private sector and the development of infrastructure. Coastal areas naturally attract human beings and include the required potential for tourists. And coastal tourism can be undoubtedly seen as a source of added value and special income for coastal cities. But, the point is necessary that coastal INVESTING AND PROVIDING THE environment is so sensitive and vulnerable and the resulted pressures from tourism-based activities such SOLUTIONS TO CONFRONT THE as creating different projects to attract tourist like hotels, markets, diving clubs, docks, etc. may destroy ENVIRONMENTAL ISSUES OF THE the environment’s ecological balance. The method PROJECTS RELATED TO COASTAL of the present research is descriptive-analytical, and data collection has been performed through library TOURISM IN KISH ISLAND studies and field observations. The research’s purpose is practical; and next to the basic knowledge of coastal tourism, it has been embarked on the study of the INVESTIR E FORNECER SOLUÇÕES PARA role of tourists in destroying the environment of Kish Island and the environmental effects of tourism-based ENFRENTAR AS QUESTÕES AMBIENTAIS projects. In the following, the research has studied the intruder factors like users’ changes and their effects on DOS PROJETOS RELACIONADOS AO the transformation of coasts as well as the changes TURISMO COSTEIRO NA ILHA DE KISH made on sandy coasts caused by the impact of human structures. The results show that the increasing number of tourists and building the tourism and welfare facilities for them have destroyed and transformed the natural form of the coasts and the issue makes it Alireza Moshabbaki Isfahani 1 necessary to planning for the sustainable development Vahideh Mojahed 2 of the coasts. -

Population-Based Seroprevalence of Malaria in Hormozgan Province, Southeastern Iran: a Low Transmission Area
Hindawi Publishing Corporation Malaria Research and Treatment Volume 2015, Article ID 174570, 5 pages http://dx.doi.org/10.1155/2015/174570 Research Article Population-Based Seroprevalence of Malaria in Hormozgan Province, Southeastern Iran: A Low Transmission Area Gholam Reza Hatam,1 Fatemeh Nejati,1 Tahereh Mohammadzadeh,2,3 Reza Shahriari Rad,4 and Bahador Sarkari1,3 1 Basic Sciences in Infectious Diseases Research Center, Shiraz University of Medical Sciences, Shiraz, Iran 2Department of Parasitology and Mycology, School of Medicine, Baqiyatallah University of Medical Sciences, Tehran, Iran 3Department of Parasitology and Mycology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran 4Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran Correspondence should be addressed to Bahador Sarkari; [email protected] Received 31 July 2015; Revised 13 September 2015; Accepted 21 September 2015 Academic Editor: Ogobara K. Doumbo Copyright © 2015 Gholam Reza Hatam et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The seroepidemiological condition of malaria in three main districts of Hormozgan Province, a low transmission area in southeast of Iran, was investigated. Methods. Sera samples (803) were collected from healthy volunteers from the three main districts (Bandar Lengeh in the west, Bandar Abbas in the center, and Bandar Jask in the east) of Hormozgan Province. A questionnaire was used to record the sociodemographic features of the participants during sample collecting. An in-house ELISA test, using crude antigens obtained from cell culture of Plasmodium falciparum, was adapted and used to detect anti-malaria antibodies in the sera. -

Systematic Paleontology, Distribution and Abundance of Cenozoic Benthic Foraminifera from Kish Island, Persian Gulf, Iran
Journal of the Persian Gulf (Marine Science)/Vol. 8/No. 28/ June 2017/22/19-40 Systematic Paleontology, Distribution and Abundance of Cenozoic Benthic Foraminifera from Kish Island, Persian Gulf, Iran Fahimeh Hosseinpour1, Ali Asghar Aryaei1*, Morteza Taherpour-Khalil-Abad2 1- Department of Geology, Mashhad Branch, Islamic Azad University, Mashhad, Iran 2- Young Researchers and Elite Club, Mashhad Branch, Islamic Azad University, Mashhad, Iran Received: January 2017 Accepted: June 2017 © 2017 Journal of the Persian Gulf. All rights reserved. Abstract Foraminifera are one of the most important fossil microorganisms in the Persian Gulf. During micropaleontological investigations in 5 sampling stations around the Kish Island, 14 genera and 15 species of dead Cenozoic benthic foraminifera were determined and described. Next to these assemblages, other organisms, such as microgastropods and spines of echinids were also looked into. In this study, the statistical analysis of foraminiferal distribution was done in one depth-zone (60-150 m and compared with the Australian-Iran Jaya Continental margin depth- zone. Keywords: Foraminifera, Distribution analysis, Kish Island, Persian Gulf, Iran Downloaded from jpg.inio.ac.ir at 9:20 IRST on Monday October 4th 2021 1. Introduction approximately 226000 km2. Its average depth is about 35 m, and it attains its maximum depth about Persian Gulf is the location of phenomenal 100 m near its entrance - the Straits of Hormuz (for hydrocarbon reserves and an area of the world where more details see details in Seibold and Vollbrecht, the oil industry is engaged in intense hydrocarbon 1969; Seibold and Ulrich 1970). It is virtually exploration and extraction. -
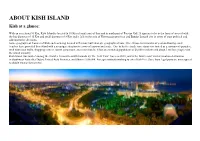
ABOUT KISH ISLAND Kish at a Glance
ABOUT KISH ISLAND Kish at a glance: With an area about 91 Km, Kish Island is located in 18 Km of south part of Iran and in north part of Persian Gulf. It appears to be in the form of an oval with the big diameter of 15 Km and small diameter of 8 Km and it falls in the area of Hormozgan province and Bandar Lengeh city in terms of state political and administrative divisions. Some geographical features of Kish such as being located in Persian Gulf strategic geographical zone, fine climate in 8 months of year and having coral beaches have provided this island with a so unique situation in terms of tourism and trade. Due to its free trade zone status it is touted as a consumer's paradise, with numerous malls, shopping centres, tourist attractions, and resort hotels. It has an estimated population of 26,000 residents and about 1 million people visit the island annually. Kish Island was ranked among the world’s 10 most beautiful islands by The New York Times in 2010, and is the fourth most visited vacation destination in Southwest Asia after Dubai, United Arab Emirates, and Sharm el-Sheikh. Foreign nationals wishing to enter Kish Free Zone from legal ports are not required to obtain visas prior to travel. Unique advantages of Kish free zone • Tourism enormous attractions • Access to world free waters • No need to visa for foreign visitors • Strategic situation and closeness to Asalooyeh oil zones • Energy resources (gas fuel) independent from the main land • Independent air lines and shipping lines with ability to carry vehicles • High level -

List of Cities in Iran
S.No. Name of City 1 Abadan 2 Abadeh 3 Abyek 4 Abhar 5 Abyaneh 6 Ahar 7 Ahvaz 8 Alavicheh 9 Aligoodarz 10 Alvand 11 Amlash 12 Amol 13 Andimeshk 14 Andisheh 15 Arak 16 Ardabil 17 Ardakan 18 Asalem 19 Asalouyeh 20 Ashkezar 21 Ashlagh 22 Ashtiyan 23 Astaneh Arak 24 Astaneh-e Ashrafiyyeh 25 Astara 26 Babol 27 Babolsar 28 Baharestan 29 Balov 30 Bardaskan 31 Bam 32 Bampur 33 Bandar Abbas 34 Bandar Anzali 35 Bandar Charak 36 Bandar Imam 37 Bandar Lengeh 38 Bandar Torkman 39 Baneh 40 Bastak 41 Behbahan 42 Behshahr 43 Bijar 44 Birjand 45 Bistam 46 Bojnourd www.downloadexcelfiles.com 47 Bonab 48 Borazjan 49 Borujerd 50 Bukan 51 Bushehr 52 Damghan 53 Darab 54 Dargaz 55 Daryan 56 Darreh Shahr 57 Deylam 58 Deyr 59 Dezful 60 Dezghan 61 Dibaj 62 Doroud 63 Eghlid 64 Esfarayen 65 Eslamabad 66 Eslamabad-e Gharb 67 Eslamshahr 68 Evaz 69 Farahan 70 Fasa 71 Ferdows 72 Feshak 73 Feshk 74 Firouzabad 75 Fouman 76 Fasham, Tehran 77 Gachsaran 78 Garmeh-Jajarm 79 Gavrik 80 Ghale Ganj 81 Gerash 82 Genaveh 83 Ghaemshahr 84 Golbahar 85 Golpayegan 86 Gonabad 87 Gonbad-e Kavous 88 Gorgan 89 Hamadan 90 Hashtgerd 91 Hashtpar 92 Hashtrud 93 Heris www.downloadexcelfiles.com 94 Hidaj 95 Haji Abad 96 Ij 97 Ilam 98 Iranshahr 99 Isfahan 100 Islamshahr 101 Izadkhast 102 Izeh 103 Jajarm 104 Jask 105 Jahrom 106 Jaleq 107 Javanrud 108 Jiroft 109 Jolfa 110 Kahnuj 111 Kamyaran 112 Kangan 113 Kangavar 114 Karaj 115 Kashan 116 Kashmar 117 Kazeroun 118 Kerman 119 Kermanshah 120 Khalkhal 121 Khalkhal 122 Khomein 123 Khomeynishahr 124 Khonj 125 Khormuj 126 Khorramabad 127 Khorramshahr -

Kishinvex 2019 Post Show Report گزارش عملکرد
ﺑﺎزارﻫﺎی ﻣﺎﻟﯽ، روﻧﻖ ﺗﻮﻟﯿﺪ و ﺷﮑﻮﻓﺎﯾﯽ اﻗﺘﺼﺎد ﻣﻠﯽ 2019 ﺑﺮﮔﺰارﮐﻨﻨﺪه ﯾـﺎزدﻫﻤﯿـﻦ ﻧـﻤﺎﯾﺸـﮕﺎه ﻣـﻌﺮﻓـﯽ ﻓﺮﺻـﺖﻫـﺎی ﺳـﺮﻣﺎﯾـﻪﮔـﺬاری ﮐﺸــﻮر Exhibition on Presenting Iran's Investment Opportunities www.kishinvex.ir ﺷﺸﻤﯿﻦ ﻧﻤﺎﯾﺸﮕﺎه ﺑﯿﻦاﻟﻤﻠﻠﯽ ﺑﻮرس، ﺑﺎﻧﮏ، ﺑﯿﻤﻪ و ﺧﺼﻮﺻﯽﺳﺎزی International Exhibition of Exchange, Banking, Insurance & Privatization ﺳﺘﺎد ﺑﺮﮔﺰاری: ﻫﻤﺮاه ﺑﺎ ﺑﺮﮔﺰاری ۳۷ﻫﻤﺎﯾﺶ و ﻧﺸﺴﺖ ﺗﺨﺼﺼﯽ داﺧﻠﯽ وﺑﯿﻦاﻟﻤﻠﻠﯽ ۸۸۱ - ۰۲۱ POST SHOW ۷۹ ۷۹۰ ﺣﺎﻣﯽ رﺳﺎﻧﻪ ای REPORT گزارش عملکرد 27 لغایت 30 آبان ماه 1398 - جزیره کیش 18th - 21st Nov. 2019 Kish Island-Iran Post Show Report گزارش عملکرد Kish Island – the Venue Kish is a 91.5-square-kilometre (35.3 sq mi) resort island in Bandar Lengeh County, Hor- mozgān Province off the southern coast of Iran in the Persian Gulf. Owing to its free trade zone status, the island is touted as a consumer’s paradise, with numerous malls, shopping centres, tourist attractions, and resort hotels. It has an estimated population of slightly more than 40,000 residents and about 1 million visitors annually. Kish Island is one of the most-visited vacation destinations in Southwest Asia. Tourists from many countries who wish to enter Kish Free Zone, are exempt from having to obtain a visa. Kish Free Zone has been turned into a gateway to Iran’s economy. Kish economy has encom- passed a wide range of economic compositions in the country. Among the most important fields of Kish economy, one can find business interactions, tourism, industrial production and investments in the services sector. Like other Iranian Free Zones, Kish Island proposes incentives for foreign investment, including tax breaks, simplified procedures for exports and imports and the possibility of one hundred percent foreign ownership which is not avail- able on the mainland, is a valuable destination for the presence of investors and economic activists. -

Geotourism Attractions of Hormuz Island, Iran
GeoJournal of Tourism and Geosites Year XII, vol. 28, no. 1, 2020, p.232-245 ISSN 2065-1198, E-ISSN 2065-0817 DOI 10.30892/gtg.28118-465 GEOTOURISM ATTRACTIONS OF HORMUZ ISLAND, IRAN Mohsen RANJBARAN* School of Geology, College of Science, University of Tehran, Tehran, Iran, e-mail: [email protected] Syed Mohammad ZAMANZADEH Department of Geography, University of Tehran, Tehran, Iran, Tehran, Iran, e-mail: [email protected] Farzad SOTOHIAN Faculty of Natural Resources, Department: Environmental Science Department, University of Guilan, Iran, e-mail: [email protected] Citation: Ranjbaran, M., Zamanzadeh, S.M. & Sotohian, F. (2020). GEOTOURISM ATTRACTIONS OF HORMUZ ISLAND, IRAN. GeoJournal of Tourism and Geosites, 28(1), 232–245. https://doi.org/10.30892/gtg.28118-465 Abstract: Hormuz Island is a salt dome situated in the Persian Gulf waters near the mouth of Hormuz Strait in Hormuzgan province, at 8 kilometers distance from Bandar Abbas. The island is elliptical, and its rock is mostly of the igneous and often volcanic type. Hormuz is one of the most beautiful Islands of the Persian Gulf due to its geological phenomena and related landforms. This island is a mature salt diapir with great mineralogical and lithological diversity. In this research, we focused on fieldwork, which included data gathering and taking photographs and also a review of the published papers and books. The main geotourism attractions of the island include various landforms resulted from differential erosion, as well as very attractive geomorphologic structures such as rocky and sandy beaches, sea caves, colorful salt domes, coral reefs, etc. -
Analysis of Epidemiological Characteristics of COVID-19
Disease and Diagnosis Dis Diagn. 2021; 10(2):51-55 doi 10.34172/ddj.2021.10 Original Article Analysis of Epidemiological Characteristics of COVID-19 Patients in Rudan county, Iran Mirza Ali Nazarnezhad1 ID , Shokrollah Mohseni2 ID , Mohammad Shamsadiny2 ID , Pirdad Najafi2 ID , Morteza Salemi2* ID 1Infectious and Tropical Disease Research Center, Hormozgan Health Institute, Hormozgan University of Medical Sciences, Bandar Abbas, Hormozgan, Iran. 2Social Determinants in Health Promotion Research Center, Hormozgan Health Institute, Hormozgan University of Medical Sciences, Bandar Abbas, Iran. *Correspondence to Abstract Morteza Salemi,Social Background: On March 11, 2020, the World Health Organization (WHO) declared the novel Determinants in Health coronavirus disease 2019 (COVID-19) as a global pandemic. The aim of the present study was to Promotion Research Center, analyze the epidemiological characteristics of COVID-19 patients in Rudan county so that regional Hormozgan Health Institute, Hormozgan University of managers can make timely and effective decisions. Medical Sciences, Bandar Materials and Methods: This is a cross-sectional study performed on all registered patients with Abbas, Iran. confirmed COVID-19 in Rudan county by July 10, 2020. Patient information was extracted from Tel: 09177654404 COVID-19 patient information registration system. The collected data included gender, age, Email: morsal59@gmail. com mortality, underlying disease, time of infection, occupation, contact history, and hospitalizations. Data were analyzed using SPSS version 22.0. Results: In this study, 614 (56%) of the patients were male and 477 (43%) were female. The mean age of patients was 43 ± 17 years. A total of 136 patients (12.5%) had at least one underlying disease. -

IOSEA Site Network Proposal Presentation for Shidvar Island
General location & Area • Coordinates : 26.791656°, 53.411513° IOSEA Site Network proposal • Hormozgan Province Date of submission: 28/7/14 • 9 km off mainland coast, 157km Sheedvar island, Islamic Republic of from Bandar-E Lengeh Iran • Total area: 97 ha Name and address of compiler(s): Coastline: 5.5km (relevant to turtles: 2km) • No permanent population Physical characteristics & biological Management authority resources Physical Ecological characteristics resources Lavan Rural District in Kish Wildlife and Aquatic Affairs GEOMORPHOLOGY: Low-lying island. Sand , District, Bandar- Management Bureau shingle or pebble shores, Rocky marine MARINE TURTLES: hawksbill (estimated Authority E Lengeh shores, Fossil corals . total 30/yr), green (occasional). contacts DOE Provincial office in County, details Hormozgan Province Hormozgan Bandar-Abbas HABITATS USED BY TURTLES: B eaches NATIONAL Province (0.1 sq km), F eeding habitats (70 ha). OTHER FAUNA.: 20,000 - National Protected Area waterfowl, shore birds, sea- birds during breeding season - Protected Area and Wildlife Several features shared with Nakhiloo Refuge (1971, 1972) Strict and Ommolkaram, Bushehr province protected INTERNATIONAL status FLORA: limited sand-dune plant community, mostly - Ramsar (1999) Seuda vermiculata and - "Important Bird Area" Atriplex sp. Public Uniqueness : largest known ownership, breeding colony of terns in Iran; no private only known breeding colony of property Socotran Comoran in Iran Socio-eco values, land/ocean uses; Current/proposed research Threats; interventions -

(Epinephelus Coioides) Cage Culture in Qeshm Island, Based on GIS
Journal of Survey in Fisheries Sciences 5(2) 77-88 2019 Environmental and ecological considerations for orange- spotted grouper (Epinephelus coioides) cage culture in Qeshm Island, based on GIS Noory Balaneji M.1; Sourinejad I.1 *; Owfi F.2; Ghasemi Z.1 Received: May 2018 Accepted: September 2018 Abstract Statistics and all of that global governance the demand for its use in the den or tool is increasing rapidly. In Iran, most of it in the areas of population away from the work of the twenty of the month and those of the other tool except it was not different items, due to the growth of public awareness and disseminating information about the properties in use of the tool and its use is growing. Fish in cage one of these measures more effective tool in the development of its reserves and the impact of these the efficiency of these proteins in human society is taking. The system of the location information into the database as a centralized access to, stored building, to update the facade of the use of different forms of static data and other dynamic made possible with the help of the technology and the technology of obtaining information such as the burning of the land in both the surveyor, satellite geodesy is, however, the photogrammetry, remote sensing away and it is the policy of the database, members of the information (cartographer of elevation and computer graphics) and is now one of the modes and methods of the information, today as a powerful tool in the process are the reference location data (points geographic) to raise the maximum. -

A NEW SPECIES of the GENUS Tropiocolotes PETERS, 1880 from HORMOZGAN PROVINCE, SOUTHERN IRAN (REPTILIA: GEKKONIDAE)
South Western Journal of Vol.9, No.1, 2018 Horticulture, Biology and Environment pp.15-23 P-Issn: 2067- 9874, E-Issn: 2068-7958 Art.no. e18102 A NEW SPECIES OF THE GENUS Tropiocolotes PETERS, 1880 FROM HORMOZGAN PROVINCE, SOUTHERN IRAN (REPTILIA: GEKKONIDAE) Iman ROUNAGHI1, Eskandar RASTEGAR-POUYANI1,* and Saeed HOSSEINIAN2 1. Department of Biology, Faculty of Science, Hakim Sabzevari University, Sabzevar, Iran 2. Young Researchers and Elite Club, Islamic Azad University, Shirvan branch, Shirvan, Iran *Corresponding author: Email: [email protected] ABSTRACT. We have described a new species of gekkonid lizard of the genus Tropiocolotes from southern Iran, on the coastal regions of Persian Gulf from Bandar-e Lengeh, Hormozgan province. Tropiocolotes hormozganensis sp. nov. belongs to the eastern clade of the genus Tropiocolotes (wolfganboehmei-nattereri complex) that is distributed in western Asia. It can be distinguished from the recent described species by having four pairs of postmentals and four nasal scales around the nostril. Postmental scales also differentiate it from T. wolfgangboehmei. The new identification key for the Iranian species of genus Tropiocolotes is provided. KEY WORDS: Endemic, Hormozgan province, Iranian Plateau, Tropiocolotes, Zagros Mountains. ZOO BANK: urn:lsid:zoobank.org:pub:C49EA333-2BEE-4D8C-85CC-CDAC0AF27902 INTRODUCTION During recent years, many lizard species have been described from Iran, with most from the Phylodctylidae and Gekkonidae families (Smid et al. 2014). The Zagros Mountains is a high endemism area in Iran that has an important role in most speciation events during recent periods (Macey et al. 1998; Gholamifard 2011; Esmaeili-Rineh et al. 2016). Many species from Phylodacthylidae were described recently, all of which are endemic to the 16 I. -

Iranian Naval Provocations
NatSec Brief - August 2021 JINSA’s Gemunder Center for Defense and Strategy Iranian Naval Provocations Blaise Misztal - Vice President for Policy Charles B. Perkins - Director for U.S.-Israel Security Policy Jonathan Ruhe - Director of Foreign Policy Ari Cicurel - Senior Policy Analyst An Iranian suicide drone attack near Oman against the Israeli-operated MT Mercer Street killed two crewmembers on July 29, marking the most significant escalation in Tehran’s aggression at sea since 2019. The attack is an alarming convergence of two dangerous trends in Iran’s aggressive activities: its maritime harassment and increasing use of drones. This year, Iran and its proxies are increasingly using drones to strike U.S. service members, partners, and interests in Iraq, Syria, Saudi Arabia, and Yemen, with limited U.S. response to date. Now, Tehran is signaling its willingness and ability to apply the lessons it has learned about drones—including its relative impunity—to its maritime aggression. Shortly after the Mercer Street attack, reports indicate that Iranian hijackers took control of the MV Asphalt Princess, a Panama-flagged tanker, in the Gulf of Oman on August 3. To deter future Iranian naval and drone aggression, the United States needs a forceful, persistent, and integrated response, alongside its partners, that disrupts Tehran’s ability to mount such attacks and instills fear of future U.S. reactions. Otherwise, Iran is likely to only escalate its attacks, as it did in 2019. What Happened? • The United States, United Kingdom, Israel, and Romania have alleged that multiple Iranian unmanned aerial vehicles (UAVs) attacked the MT Mercer Street near Oman on July 29, killing the Romanian captain and one British crew member.