Socioeconomic Status & Health Seeking Behavior Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Case of Bangladesh D National Se
Globalization, Local Crimes and National Security: The Case of Bangladesh Submitted by: Md. Ruhul Amin Sarkar Session: 149/2014-2015 Department: International Relations University of Dhaka. P a g e | 1 Abstract Globalization has become one of the most significant phenomena in the world since the end of the cold war. Globalization especially the economic globalization has brought about new opportunities and opened dynamic windows for the people of the world based on the notion of liberalism, free market, easy access of goods and services. Although globalization has brought about some positive gains for individuals and society, it has caused negative impacts on the society called ‘the dark side of globalization’. It has created complex and multifaceted security problems and threats to the countries especially the developing countries like Bangladesh. Globalization has changed the nature and dynamics of crime although crime is not a new phenomenon in Bangladesh. The nature or pattern of crime has changed remarkably with the advent of globalization, modern technology and various modern devices, which pose serious security threats to the individuals, society and the country. Globalization has created easy access to conducting illegal trade such as small arms, illegal drugs and human trafficking and some violent activities such as kidnapping, theft, murder, around the world as well as in Bangladesh. It has developed the new trends of crimes, gun violence, drugs crime, and increasing number of juvenile convicts and heinous crimes committed in Bangladesh. Over the years, the number of organized murder crimes is increasing along with rape cases and pretty nature of crimes with the advent of globalization and information technology. -

Bounced Back List.Xlsx
SL Cycle Name Beneficiary Name Bank Name Branch Name Upazila District Division Reason for Bounce Back 1 Jan/21-Jan/21 REHENA BEGUM SONALI BANK LTD. NA Bagerhat Sadar Upazila Bagerhat Khulna 23-FEB-21-R03-No Account/Unable to Locate Account 2 Jan/21-Jan/21 ABDUR RAHAMAN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number SHEIKH 3 Jan/21-Jan/21 KAZI MOKTADIR HOSEN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 4 Jan/21-Jan/21 BADSHA MIA SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 5 Jan/21-Jan/21 MADHAB CHANDRA SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number SINGHA 6 Jan/21-Jan/21 ABDUL ALI UKIL SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 7 Jan/21-Jan/21 MRIDULA BISWAS SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 8 Jan/21-Jan/21 MD NASU SHEIKH SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 9 Jan/21-Jan/21 OZIHA PARVIN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 10 Jan/21-Jan/21 KAZI MOHASHIN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 11 Jan/21-Jan/21 FAHAM UDDIN SHEIKH SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 12 Jan/21-Jan/21 JAFAR SHEIKH SONALI BANK LTD. -

Tor for Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan
Selection of Web Firm for Web Site Designing Development & Hosting ToR for Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan ANNEX-X TERMS OF REFERENCE (TOR) for Selection of Web Firm for Web Site Designing Development & Hosting Under ÒPÆMÖvg †Rjvi gximivB Dc‡Rjvi Dbœqb cwiKíbv cÖYqb t mvwe©K `y‡h©vM e¨e¯’vcbv‡K f~wg e¨env‡ii gva¨‡g m¤ú„³KiYÓ (Preparation of Development Plan for Mirsharai Upazila, Chattogram District: Risk Sensitive Landuse Plan) URBAN DEVELOPMENT DIRECTORATE Ministry of Housing and Public Works Government of the People’s Republic of Bangladesh November, 2016 Signature of the Bidder Signature of the Project Director Signature of the Director 131 Selection of Web Firm for Web Site Designing Development & Hosting ToR for Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan Table of Content Content Page No. Appendix-01: Background Information of the Project 133 Appendix-02: Scope of Work of the Assignment 136 Appendix-03: Bidding For Tender 141 Appendix-04: Format of Curriculum Vitae and Project Team 142 Signature of the Bidder Signature of the Project Director Signature of the Director 132 Selection of Web Firm for Web Site Designing Development & Hosting ToR for Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan APPENDIX 01 BCKGROUND INFORMATION OF THE PROJECT 1.1. Project Background Mirsharai Upazila (CHATTOGRAM DISTRICT) area 482.88 sqkm(BBS)/509.80sqkm(GIS Data), located in between 22°39' and 22°59' north latitudes and in between 91°27' and 91°39' east longitudes. -

Department of Sociology University of Dhaka Dhaka University Institutional Repository
THE NATURE AND EXTENT OF HOMICIDE IN BANGLADESH: A CONTENT ANALYSIS ON REPORTS OF MURDER IN DAILY NEWSPAPERS T. M. Abdullah-Al-Fuad June 2016 Department of Sociology University of Dhaka Dhaka University Institutional Repository THE NATURE AND EXTENT OF HOMICIDE IN BANGLADESH: A CONTENT ANALYSIS ON REPORTS OF MURDER IN DAILY NEWSPAPERS T. M. Abdullah-Al-Fuad Reg no. 111 Session: 2011-2012 Submitted in partial fulfillment of the requirements of the degree of Master of Philosophy June 2016 Department of Sociology University of Dhaka Dhaka University Institutional Repository DEDICATION To my parents and sister Dhaka University Institutional Repository Abstract As homicide is one of the most comparable and accurate indicators for measuring violence, the aim of this study is to improve understanding of criminal violence by providing a wealth of information about where homicide occurs and what is the current nature and trend, what are the socio-demographic characteristics of homicide offender and its victim, about who is most at risk, why they are at risk, what are the relationship between victim and offender and exactly how their lives are taken from them. Additionally, homicide patterns over time shed light on regional differences, especially when looking at long-term trends. The connection between violence, security and development, within the broader context of the rule of law, is an important factor to be considered. Since its impact goes beyond the loss of human life and can create a climate of fear and uncertainty, intentional homicide (and violent crime) is a threat to the population. Homicide data can therefore play an important role in monitoring security and justice. -
Appendix XIII
Preparatory Survey on Dhaka-Chittagong Main Power Grid Strengthening Project Final Report Appendices Appendix XIII Final Report on Abbreviated Resettlement Plan (ARP) PREPARATORY SURVEY ON DHAKA-CHITTAGONG MAIN POWER GRID STRENGTHENING PROJECT FINAL REPORT ON ABBREVIATED RESETTLEMENT PLAN (ARP) FOR MEGHNAGHAT-MADUNAGHAT-MATARBARI 400KV TRANSMISSION LINE PROJECT SUBMITTED BY ENGINEERS ASSOCIATES LIMITED (EAL) 1/3, ASAD GATE ROAD, BLOCK– A MOHAMMADPUR HOUSING ESTATE, DHAKA-1207 TEL.: 880-2-9111358, 880-2-8117246 FAX.: 880-2-8118512 E-MAIL: [email protected] WEBSITE: www.ealbd.com February 15, 2015 Table of Contents 1.0 Brief Project Description .................................................................................................... 1 1.1 Project Proponent .......................................................................................................... 1 1.2 Project location and area ................................................................................................ 1 1.2.1 Proposed Meghnaghat 400kV substation: .............................................................. 1 1.2.2 Propposed Madunaghat 400kV substation: ............................................................ 3 1.2.3 Route of Proposed 400kV Transmission Line: ........................................................ 5 1.3 Nature and size of the Project ........................................................................................ 8 2.0 Examination of Alternatives ......................................................................................... -
Landslide Inventory and Land-Use Mapping, DEM Preparation, Precipitation Threshold Value & Establishment of Early Warning Devices
Rainfall Triggered Landslide Hazard Zonation in Cox’s Bazaar and Teknaf Municipalities as well as Introducing Community-based Early Warning System for Landslide Hazard Management Report on Landslide Inventory & Land-use Mapping, DEM Preparation, Precipitation Threshold Value & Establishment of Early Warning Devices ComprehensiveDisasterManagementProgrammeII(CDMPII) MinistryofFoodandDisasterManagement(MoFDM) DisasterManagementandReliefDivision(DMRD) GovernmentofthePeoplesRepublicofBangladesh RainfallTriggeredLandslideHazardZonationinCox’sBazar&TeknafMunicipalitiesas well as Introducing Communitybased Early Warning System for Landslide Hazard Management Revised Report on Landslide Inventory and Land-use Mapping, DEM Preparation, Precipitation Threshold Value & Establishment of Early Warning Devices TableofContents Chapter1: LandslideInventoryMapping,LanduseMapping&DEMPreparation..................................................5 Executivesummary................................................................................................................................................5 1. LandslideInventoryMapping...............................................................................................................9 1.1. Introduction...............................................................................................................................................9 1.2. StatementoftheProblemandDescriptionoftheStudyArea........................................................10 1.2.1. GeneralLandslideHistoryofBangladesh.........................................................................................10 -

Report on AK Taj Group Masrur M. A. Hoque.Pdf (983.4Kb)
Internship Report on AK TAJ GROUP Prepared for, MD. Tamzidul Islam Assistant Professor BRAC BusinessSchool BRAC University Prepared By, Masrur M. A. Hoque ID # 12164092 Submission Date – 15/12/2015 LETTER OF TRANSMITTAL December 15, 2015 MD. Tamzidul Islam Assistant Professor BRAC BusinessSchool BRAC University Subject: Internship Report. Dear Sir, I would like to thank you for supervising and helping me throughout the semester. With due respect I am submitting a copy of intern report foryourappreciation. I have given my best effort to prepare the report with relevant information that I have collected from an onsite production department which is belongs to a group of company and from other sources during my accomplishthe course. I have the immense pleasure to have the opportunity to study on the marketing practices of AK TAJ Group. There is no doubt that the knowledge I have gathered during the study will help me in real life. For your kind consideration I would like to mention that there might be some errors and mistakes due to limitations of my knowledge. I expect that you will forgive me considering that I am still learner and in the process of learning. Thanking for your time and reviews. Yours faithfully Masrur M. A. Hoque ID-12164092 BRAC Business School BRAC University Acknowledgement The successful completion of this internship might not be possible in time without the help some person whose suggestion and inspiration made it happen. First of all I want to thank my Course Instructor MD. Tamzidul Islam for guiding me during the course. Without his help this report would not have been accomplished. -

List of Upazilas of Bangladesh
List Of Upazilas of Bangladesh : Division District Upazila Rajshahi Division Joypurhat District Akkelpur Upazila Rajshahi Division Joypurhat District Joypurhat Sadar Upazila Rajshahi Division Joypurhat District Kalai Upazila Rajshahi Division Joypurhat District Khetlal Upazila Rajshahi Division Joypurhat District Panchbibi Upazila Rajshahi Division Bogra District Adamdighi Upazila Rajshahi Division Bogra District Bogra Sadar Upazila Rajshahi Division Bogra District Dhunat Upazila Rajshahi Division Bogra District Dhupchanchia Upazila Rajshahi Division Bogra District Gabtali Upazila Rajshahi Division Bogra District Kahaloo Upazila Rajshahi Division Bogra District Nandigram Upazila Rajshahi Division Bogra District Sariakandi Upazila Rajshahi Division Bogra District Shajahanpur Upazila Rajshahi Division Bogra District Sherpur Upazila Rajshahi Division Bogra District Shibganj Upazila Rajshahi Division Bogra District Sonatola Upazila Rajshahi Division Naogaon District Atrai Upazila Rajshahi Division Naogaon District Badalgachhi Upazila Rajshahi Division Naogaon District Manda Upazila Rajshahi Division Naogaon District Dhamoirhat Upazila Rajshahi Division Naogaon District Mohadevpur Upazila Rajshahi Division Naogaon District Naogaon Sadar Upazila Rajshahi Division Naogaon District Niamatpur Upazila Rajshahi Division Naogaon District Patnitala Upazila Rajshahi Division Naogaon District Porsha Upazila Rajshahi Division Naogaon District Raninagar Upazila Rajshahi Division Naogaon District Sapahar Upazila Rajshahi Division Natore District Bagatipara -

TERMS of REFERENCE (TOR) for Subsurface Geological Study
Subsurface Geological Study and Seismic Hazard Assessment ToR for Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan ANNEX-VII TERMS OF REFERENCE (TOR) for Subsurface Geological Study and Seismic Hazard Assessment for Mirsharai Upazila under ÒPÆMÖvg †Rjvi gximivB Dc‡Rjvi Dbœqb cwiKíbv cÖYqb t mvwe©K `y‡h©vM e¨e¯’vcbv‡K f~wg e¨env‡ii gva¨‡g m¤ú„³KiYÓ (Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan) URBAN DEVELOPMENT DIRECTORATE Ministry of Housing and Public Works Government of the People’s Republic of Bangladesh November, 2016 pg. 81 Subsurface Geological Study and Seismic Hazard Assessment ToR for Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan Content Page No. Appendix-01: Background Information of the Project 83 Appendix-02: Scope of Work 85 Appendix-03: Bidding For Tender 91 Appendix-04: Format of Curriculum Vitae and Project Team 92 pg. 82 Subsurface Geological Study and Seismic Hazard Assessment ToR for Preparation of Development Plan for Mirsharai Upazila, Chittagong District: Risk Sensitive Landuse Plan APPENDIX 01 BCKGROUND INFORMATION OF THE PROJECT 1.1. Project Background Mirsharai Upazila (CHITTAGONG DISTRICT) area 482.88 sqkm(BBS)/509.80sqkm(GIS Data), located in between 22°39' and 22°59' north latitudes and in between 91°27' and 91°39' east longitudes. It is bounded by TRIPURA state of India, CHHAGALNAIYA and FENI SADAR upazilas on the north, SITAKUNDA upazila and BAY OF BENGAL on the south, FATIKCHHARI upazila on the east, SONAGAZI and COMPANIGANJ (NOAKHALI) upazilas on the west. -

A Study on Residential Shift of the Remittance Receiving Households
MURP THESIS A STUDY ON RESIDENTIAL SHIFT OF THE REMITTANCE RECEIVING HOUSEHOLDS KAUSIK DAS KAUSIK DAS DEPARTMENT OF URBAN AND REGIONAL PLANNING BANGLADESH UNIVERSITY OF ENGINEERING AND TECHNOLOGY DHAKA, BANGLADESH MAY 2010 MAY 2010 A STUDY ON RESIDENTIAL SHIFT OF THE REMITTANCE RECEIVING HOUSEHOLDS By KAUSIK DAS MASTER OF URBAN AND REGIONAL PLANNING DEPARTMENT OF URBAN AND REGIONAL PLANNING BANGLADESH UNIVERSITY OF ENGINEERING AND TECHNOLOGY DHAKA, BANGLADESH MAY 2010 The thesis titled, “A STUDY ON RESIDENTIAL SHIFT OF THE REMITTANCE RECEIVING HOUSEHOLDS” submitted by Kausik Das, Roll No: 100615032(F),Session: October 2006, has been accepted as satisfactory in partial fulfillment of the requirements for the degree of MASTER OF URBAN AND REGIONAL PLANNING (MURP) on 4 May, 2010 BOARD OF EXAMINERS Md. Musleh Uddin Hasan Assistant Professor Department of Urban and Regional Planning, BUET Chairman &Supervisor Dr. Sarwar Jahan Professor and Head Department of Urban and Regional Planning, BUET Member(Ex-Officio) Dr. Shakil Akther Associate Professor Department of Urban and Regional Planning, BUET Member Dr. Chowdhury Rafiqul Abrar Professor Department of International Relations, Member (External) Dhaka University Director RMMRU, Dhaka CANDIDATE’S DECLARATION It is hereby declared that this thesis or any part of it has not been submitted elsewhere for the award of any degree or diploma. Kausik Das Student No. 100615032 URP, BUET, Dhaka Dedicated to My parents TABLE OF CONTENT Page No. List of Tables iv List of Figures v List of Maps v Abbreviation -

Annex to Chapter 3. Results Framework for the 4Th HPBSP 2016
Annex to Chapter 3. Results Framework for the 4th HPBSP 2016-2021 Means of Result Indicator verification & Baseline & source Target 2021 timing Goal GI 1. Under-5 Mortality Rate (U5MR) BDHS, every 3 years 46, BDHS 2014 37 All citizens of GI 2. Neonatal Mortality Rate (NNMR) BDHS, every 3 years 28, BDHS 2014 21 Bangladesh enjoy health and well-being GI 3. Maternal Mortality Ratio (MMR) BMMS; MPDR 176, WHO 2015(http:// 105 www.who.int/ reproductivehealth/ publications/monitoring/ maternal-mortality-2015/ en/ GI 4. Total Fertility Rate (TFR) BDHS, every 3 years 2.3, BDHS 2014 1.7 GI 5. Prevalence of stunting among under- BDHS, every 3 years; 36.1%, BDHS 2014 25% 5children UESD, every non-DHS years GI 6. Prevalence of diabetes and hypertension BDHS, every 3 years; Dia: 11.2%; Hyp: 31.9%, Dia: 10%; Hyp: among adult women (Estimated as elevated blood NCD-RF, every 2 years BDHS 2011 30% sugar and blood pressure among women and men aged 35 years or older) GI 7. Percentage of public facilities with key BHFS, every 2 years FP: 38.2; ANC 7.8%; CH FP: 70%; ANC service readiness as per approved Essential 6.7%, BHFS 2014 50%; CH 50% Service Package (Defined as facilities (excluding CCs) having: a. for FP: guidelines, trained staff, BP machine, OCP, and condom; b. for ANC: Health Bulletin 2019 Health guidelines, trained staff, BP machine, hemoglobin, and urine protein testing capacity, Fe/folic acid tablets; c. for CH: IMCI guideline and trained staff, child scale, thermometer, growth chart, ORS, zinc, Amoxicillin, Paracetamol, Anthelmintic) Program -
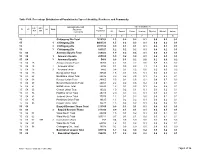
Chittagong C09.Pdf
Table C-09: Percentage Distribution of Population by Type of disability, Residence and Community Administrative Unit Type of disability (%) UN / MZ / Total ZL UZ Vill RMO Residence WA MH Population Community All Speech Vision Hearing Physical Mental Autism 1 2 3 4 5 6 7 8 9 10 15 Chittagong Zila Total 7616352 1.3 0.2 0.2 0.1 0.5 0.2 0.1 15 1 Chittagong Zila 4463723 1.5 0.2 0.3 0.1 0.6 0.2 0.1 15 2 Chittagong Zila 2971102 0.9 0.1 0.1 0.1 0.4 0.1 0.1 15 3 Chittagong Zila 181527 1.2 0.2 0.2 0.1 0.4 0.2 0.1 15 04 Anowara Upazila Total 259022 1.9 0.2 0.4 0.1 0.8 0.3 0.1 15 04 1 Anowara Upazila 253556 1.9 0.2 0.4 0.1 0.8 0.3 0.1 15 04 3 Anowara Upazila 5466 0.8 0.1 0.2 0.0 0.2 0.0 0.2 15 04 15 Anowara Union Total 10260 4.2 0.3 2.2 0.6 0.8 0.2 0.2 15 04 15 1 Anowara Union 4794 8.1 0.5 4.5 1.1 1.5 0.3 0.3 15 04 15 3 Anowara Union 5466 0.8 0.1 0.2 0.0 0.2 0.0 0.2 15 04 19 Bairag Union Total 30545 1.8 0.1 0.5 0.1 0.6 0.3 0.1 15 04 28 Barakhain Union Total 28836 3.0 0.2 0.5 0.1 1.8 0.3 0.1 15 04 38 Barasat Union Total 28865 2.5 0.2 0.6 0.2 0.8 0.7 0.2 15 04 47 Burumchhara Union Total 20061 2.2 0.2 0.6 0.2 1.0 0.1 0.1 15 04 57 Battali Union Total 23630 1.3 0.1 0.2 0.1 0.5 0.2 0.1 15 04 66 Chatari Union Total 19022 1.0 0.2 0.1 0.1 0.3 0.2 0.1 15 04 76 Haildhar Union Total 25315 2.0 0.4 0.3 0.1 0.7 0.3 0.1 15 04 81 Juidandi Union Total 17575 1.2 0.1 0.2 0.0 0.6 0.1 0.1 15 04 85 Paraikora Union Total 19635 1.3 0.2 0.2 0.1 0.6 0.2 0.1 15 04 95 Roypur Union Total 35278 1.5 0.2 0.2 0.1 0.6 0.2 0.1 15 06 Bayejid Bostami Thana Total 211355 0.9 0.1 0.1 0.1 0.4 0.1 0.1 15 06 2 Bayejid Bostami Thana 211355 0.9 0.1 0.1 0.1 0.4 0.1 0.1 15 06 01 Ward No-01 Total 29209 1.5 0.1 0.2 0.1 0.9 0.1 0.1 15 06 02 Ward No-02 Total 103314 0.7 0.1 0.1 0.0 0.3 0.1 0.1 15 06 02 998 2 Cantonment (Part) 758 0.4 0.0 0.0 0.0 0.1 0.0 0.3 15 06 03 Ward No-03 Total 68794 1.2 0.1 0.2 0.1 0.5 0.2 0.1 15 06 98 Chittagang Cnt.