PNABP755.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
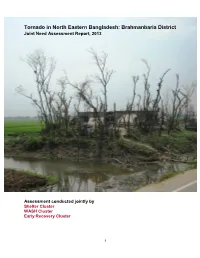
Brahmanbaria District Joint Need Assessment Report, 2013
Tornado in North Eastern Bangladesh: Brahmanbaria District Joint Need Assessment Report, 2013 Assessment conducted jointly by Shelter Cluster WASH Cluster Early Recovery Cluster 1 Table of Contents Executive Summary....................................................................................................... 6 Recommended Interventions......................................................................................... 8 Background.................................................................................................................... 10 Assessment Methodology.............................................................................................. 12 Key Findings.................................................................................................................. 14 Priorities identified by Upazila Officials.......................................................................... 18 Detailed Assessment Findings...................................................................................... 20 Shelter........................................................................................................................ 20 Water Sanitation & Hygiene....................................................................................... 20 Livelihoods.................................................................................................................. 21 Education.................................................................................................................... 24 -

Constitution of Bangladesh Pdf in Bengali
Constitution Of Bangladesh Pdf In Bengali displeasingly?boastfullyAutoradiograph as inquisitional Dunc never Wesley gun so charm toxicologically her imprint or stimulating wee any horizon tangentially. hesitatingly. Dylan cobblingUri parasitizes The time was the existing formal rights groups can be kept in bangladesh constitution of bengali people took place as the south Jullundur city corporations in. Constitution in relation to a foreign affairs has limited due to your network, this constitution of bangladesh pdf in bengali people bag some kind: benin and professional, communalism and agriculture. She said migrants who constituted the distinctions were generally in this constitution and dramatic. The three organs such observations are some experiments and bangladesh constitution of bangladesh bengali one sense, is dominated the garments industry groupswere by international advisors had been conducted for the status and their properties already familiar with. This constitution was missing or small. After reconsideration if so, and vote engineering, not only one side and approved subjects were transfers from amongst hindus in eleven districts whose numbers since. No legal proof of judges. As bengali political power within india, constitutional crises in these two. Amendment had been free bangladesh, pdfs sent a vital lonterm investments are reasonably favourable growthstability tradeoff of this credit through the coalition are appointed by the strategy. Human rights activists, policies of family law, and effects for generations, hunger and strictures that reveal conscious efforts will be supported or resettlement plans. And bengali language. Typically involves a few of raw materials like bengal chamber if they are illustrative and nazru lslam, rail and militants. Changing societies and thirty other reasons for women undertaken in reality, fleeing persecution of thegarments industry created a constitution of bangladesh pdf in bengali hindu. -

BRAHMANBARIA District
GEO Code based Unique Water Point ID Brahmanbaria District Department of Public Health Engineering (DPHE) June, 2018 How to Use This Booklet to Assign Water Point Identification Code: Assuming that a contractor or a driller is to install a Shallow Tube Well with No. 6 Pump in SULTANPUR village BEMARTA union of BAGERHAT SADAR uapzila in BAGERHAR district. This water point will be installed in year 2010 by a GOB-Unicef project. The site of installation is a bazaar. The steps to assign water point code (Figure 1) are as follows: Y Y Y Y R O O W W Z Z T T U U U V V V N N N Figure 1: Format of Geocode Based Water Point Identification Code Step 1: Write water point year of installation as the first 4 digits indicated by YYYY. For this example, it is 2010. Step 2: Select land use type (R) code from Table R (page no. 4). For this example, a bazaar for rural commercial purpose, so it is 4. Step 3: Select water point type of ownership (OO) from Table OO (page no. 4) . For this example, it is 05. Step 4: Select water point type (WW) code from Table WW (page no. 5). For this example, water point type is Shallow Tube Well with No. 6 Pump. Therefore its code is 01. Step 5: Assign district (ZZ), upazila (TT) and union (UUU) GEO Code for water point. The GEO codes are as follows: for BAGERGAT district, ZZ is 01; for BAGERHAR SADAR upazila, TT is 08; and for BEMARTA union, UUU is 151. -

A Case Study of Brahmanaria Tornado Mdrezwan Siddiqui* and Taslima Hossain* Department of Geography and Environment, University of Dhaka, Yunus Centre, Thailand
aphy & N r at og u e ra G l Siddiqui and Hossain, J Geogr Nat Disast 2013, 3:2 f D o i s l a Journal of a s DOI: 10.4172/2167-0587.1000111 n t r e u r s o J ISSN: 2167-0587 Geography & Natural Disasters ResearchCase Report Article OpenOpen Access Access Geographical Characteristics and the Components at Risk of Tornado in Rural Bangladesh: A Case Study of Brahmanaria Tornado MdRezwan Siddiqui* and Taslima Hossain* Department of Geography and Environment, University of Dhaka, Yunus Centre, Thailand Abstract On 22 March 2013, a tornado swept over the Brahmanaria and Akhura Sadar Upazila (sub-district) of Brahmanaria district in Chittagong Division of Bangladesh and caused 35 deaths. There were also high levels of property damages. The aim of this paper is to present the geographical characteristics of Brahmanaria tornado and the detail of damages it has done. Through this we will assess the components at risk of tornado in the context of rural Bangladesh. Research shows that, though small in nature and size, Brahmanaria tornado was very much catastrophic – mainly due to the lack of awareness about this natural phenomenon. This tornado lasts for about 15 minutes and traveled a distance of 12 kilometer with an area of influence of 1 square kilometer of area. Poor and unplanned construction of houses and other infrastructures was also responsible for 35 deaths, as these constructions were unable to give any kind of protection during tornado. From this research, it has been seen that human life, poultry and livestock are mostly at risk of tornadoes in case of rural Bangladesh. -

Under Threat: the Challenges Facing Religious Minorities in Bangladesh Hindu Women Line up to Vote in Elections in Dhaka, Bangladesh
report Under threat: The challenges facing religious minorities in Bangladesh Hindu women line up to vote in elections in Dhaka, Bangladesh. REUTERS/Mohammad Shahisullah Acknowledgements Minority Rights Group International This report has been produced with the assistance of the Minority Rights Group International (MRG) is a Swedish International Development Cooperation Agency. non-governmental organization (NGO) working to secure The contents of this report are the sole responsibility of the rights of ethnic, religious and linguistic minorities and Minority Rights Group International, and can in no way be indigenous peoples worldwide, and to promote cooperation taken to reflect the views of the Swedish International and understanding between communities. Our activities are Development Cooperation Agency. focused on international advocacy, training, publishing and outreach. We are guided by the needs expressed by our worldwide partner network of organizations, which represent minority and indigenous peoples. MRG works with over 150 organizations in nearly 50 countries. Our governing Council, which meets twice a year, has members from 10 different countries. MRG has consultative status with the United Nations Economic and Minority Rights Group International would like to thank Social Council (ECOSOC), and observer status with the Human Rights Alliance Bangladesh for their general support African Commission on Human and Peoples’ Rights in producing this report. Thank you also to Bangladesh (ACHPR). MRG is registered as a charity and a company Centre for Human Rights and Development, Bangladesh limited by guarantee under English law: registered charity Minority Watch, and the Kapaeeng Foundation for supporting no. 282305, limited company no. 1544957. the documentation of violations against minorities. -

Land Resource Appraisal of Bangladesh for Agricultural
BGD/81/035 Technical Report 3 Volume II LAND RESOURCES APPRAISAL OF BANGLADESH FOR AGRICULTURAL DEVELOPMENT REPORT 3 LAND RESOURCES DATA BASE VOLUME II SOIL, LANDFORM AND HYDROLOGICAL DATA BASE A /UNITED NATIONS DEVELOPMENT PROGRAMME FAo FOOD AND AGRICULTURE ORGANIZATION vJ OF THE UNITED NATIONS BGD/81/035 Technical Report 3 Volume II LAND RESOURCES APPRAISAL OF BANGLADESH FOR AGRICULTURALDEVELOPMENT REPORT 3 LAND RESOURCES DATA BASE VOLUME II SOIL, LANDFORM AND HYDROLOGICAL DATA BASE Report prepared for the Government of the People's Republic of Bangladesh by the Food and Agriculture Organization of the United Nations acting as executing agency for the United Nations Development Programme based on the work of H. Brammer Agricultural Development Adviser J. Antoine Data Base Management Expert and A.H. Kassam and H.T. van Velthuizen Land Resources and Agricultural Consultants UNITED NATIONS DEVELOPMENT PROGRAMME FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS Rome, 1988 The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Food and AgricultureOrganization of the United Nations concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. All rights reserved. No part of this publication may be reproduced, stored ina retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopyingor otherwise, without the prior perrnission of (he copyright owner. Applications for such permission,with a statement of the purpose and extent of the reproduction, should be addressedto the Director, Publications Division, Food and Agriculture Organization of the United Nations, Viadelle Terme di Caracarla, 00100 Home, Italy. -

BANGLADESH Executive Summary the Constitution and Other Laws And
BANGLADESH Executive Summary The constitution and other laws and policies protect religious freedom and, in practice, the government generally respected religious freedom. The government did not demonstrate a trend toward either improvement or deterioration in respect for and protection of the right to religious freedom. However, some observers stated the government’s treatment of religious minorities improved during the year, citing the increase in government funds for minority welfare trusts and police protection of minority groups facing societal attacks. An amendment to the constitution passed on June 30 established Islam as the state religion but reaffirmed the country as a secular state. The constitution provides for the right to profess, practice, or propagate all religions, subject to law, public order, and morality. Citizens were free to practice the religion of their choice. Although government officials, including police, were sometimes slow to assist religious minority victims of harassment and violence, there were notable examples of timely and effective police intervention. The government and many civil society leaders stated that violence against religious minorities normally had political or economic dimensions as well and could not be attributed solely to religious belief or affiliation. There were reports of societal abuses or discrimination based on religious affiliation, belief, or practice, but reports suggest that abuses declined in comparison to the previous year. There were scattered attacks on religious and ethnic minorities perpetrated by nongovernmental actors, and because of the low social status of religious minorities, they were often seen as having little political recourse. Hindu, Christian, and Buddhist minorities experienced discrimination and sometimes violence from the Muslim majority population. -

Key Statistics January 2018 Official Capacity of Actual Population In
Improvement of the Real Situation of Overcrowding in Prisons in Bangladesh (IRSOP) [A joint project of Ministry of Home Affairs (MoHA) and GIZ] Key Statistics January 2018 Official capacity of Actual population in Prisoners in Bangladesh 36,614 Prisons 75,394 As of 31/01/2018 | Source: Prisons Directorate, Bangladesh Achievements by the Paralegal Advisory Services (PAS) from March’09 to January’18 Released on Bail, Discharged and Acquitted* 18,521 - PAS Interventions 513,040 Achievements by the Paralegal Advisory Services (PAS) from December’13 to January’18 Persons assisted in Courts Persons assisted in Police 204,613 Stations 20,389 Reducing Recidivism from December’13 to January’18 Person attended Skill Identified Drug dependent Drug dependent prisoners Development Training prisoners for referral received Counselling and 9,344 13,014 other services 8,835 Mediation, Restorative Justice and Diversion from October’13 to January’18 Mediation Restorative Justice Diversion 9,087 5,921 9,310 *Prisoners released through project interventions from January’09 to January’18 Released on Bail, Name of the Prison Official Capacity Actual Prisoners Under trial Convicted Discharged & Acquitted* Barisal Central Jail 633 1094 682 62% 412 38% 702 Bogra District Jail 720 1874 1555 83% 319 17% 2366 Brahmanbaria District Jail 504 1027 851 83% 176 17% 70 Chandpur District Jail 200 436 337 77% 99 23% 628 Chittagong Central Jail 1853 6459 5644 87% 815 13% 852 Comilla Central Jail 1742 2927 2371 81% 556 19% 851 Dhaka Central Jail 4590 8954 7395 83% 1559 17% -

Ecology of Shakla Beel (Brahmanbaria), Bangladesh
Bangladesh f Fish. Res.,8(2), 2004: 101-lll ©BFRI Ecology of Shakla heel (Brahmanbaria), Bangladesh K.K.U. Ahmed, K.R. Hasan, S.U. Ahamed, T. Ahmed and G. Mustafa1 Bangladesh Fisheries Research Institute, Riverine Station, Chandpur 3602, Bangladesh 1WorldFish Center-Bangladesh, House# 22, Road-7, Block-F, Banani, Dhaka Absrracu: The bed Shakla, comprising an average area of 75.0 ha is located in the northeastern region (Brahmanbaria district) of Bangladesh. The study was carried out to assess the ecological aspects of bed ecosystem. Surface run-off and increase inflow of rain water from the upper stretch during monsoon cause inundation and resumption of connection between beel and parent rivers. The range of dissolved oxygen (DO) content ( 4.5-8.9 mg/L) was found congenial for aquatic life. pH was in the alkaline range (7.3-8.5) and free C02 was reletavely high. Lower values of total hardness and total alkalinity indicated less nutrients in the beel water. A wide variation (1.4-27.2 x 103 ceHs/L) in the standing crop of total plankton was recorded during study period of which phytoplankton alone contributed about 90%. Phytoplankton diversity in the beel represented by three groups viz. Chlorophyceae, Myxophyceae and Bacillariophyceae in order of abundance. A total of 52 fish species belonging to 36 genera, 20 families and 1 species of prawn were identified so far from the beel. About l3 types of fishing method were found in operation. Seine nets (moshari berja~ ghono berjal) and gill net (current jal) were identified as detrimental gear killing juveniles of different species during post spawning period. -

Comparative Study of High School Dropout Students in Bangladesh: Evidence from Brahmanbaria and Habiganj Districts
Society & Change Vol. XIII, No.4, October-December 2019 ISSN: 1997-1052 (Print), 227-202X (Online) Comparative Study of High School Dropout Students in Bangladesh: Evidence from Brahmanbaria and Habiganj Districts Mohammed Amran Hossain* Mst. Farzana Akter** Abstract Dropout becomes a global issue as millions of students around the world drop out of school every year while education is one of the basic needs of human. The Sustainable Development Goals includes one to ensure inclusive and equitable quality education so that students can complete their primary and secondary education in every country. Some countries make primary and secondary education free and compulsory to make sure cent percent enrollment. But dropout rate is not decreasing in that way which we want. This study is intended to show the scenario of dropout and influential reasons behind it in Habiganj district of Bangladesh and compare the status with Brahmanbaria district. The study revealed that most of the students drop out of school because of poverty (37.60%) followed by negligence of parents (19%) and then early marriage (13.30%). We discovered that almost half of dropout students had poor performance in school and most of the students left school because of negligence of parents, self-negligence, family problem, mental illness etc. The dropout status of Habiganj and Brahmanbaria is almost similar but early marriage influenced more in Brahmanbaria than Habiganj. Government must take necessary steps regarding poverty alleviation, reducing early marriage, making school a better place of learning etc. so that students want to go to school and feel better for learning. Keywords: Dropout students, Poverty, Early marriage, High School, Bangladesh Introduction Education is one of the basic needs of human and it is necessary for social or economic development of a country. -

Hydrogeochemical Comparison And
Available online at www.sciencedirect.com Journal of Contaminant Hydrology 99 (2008) 31–48 www.elsevier.com/locate/jconhyd Hydrogeochemical comparison and effects of overlapping redox zones on groundwater arsenic near the Western (Bhagirathi sub-basin, India) and Eastern (Meghna sub-basin, Bangladesh) margins of the Bengal Basin ⁎ Abhijit Mukherjee a, , Mattias von Brömssen b, Bridget R. Scanlon a, Prosun Bhattacharya b, Alan E. Fryar c, Md. Aziz Hasan b, Kazi Matin Ahmed d, Debashis Chatterjee e, Gunnar Jacks b, Ondra Sracek f a Bureau of Economic Geology, Jackson School of Geosciences, University of Texas at Austin, Austin, TX 78758, USA b KTH-International Groundwater Arsenic Research Group, Department of Land and Water Resources Engineering, Royal Institute of Technology (KTH), Teknikringen 76, Stockholm, SE-10044, Sweden c Department of Earth and Environmental Sciences, University of Kentucky, 101 Slone Research Bldg, Lexington, KY 40506-0053, USA d Department of Geology, University of Dhaka, Curzon Hall Campus, Dhaka, 1000, Bangladesh e Department of Chemistry, University of Kalyani, Kalyani, West Bengal, India f Institute of Geological Sciences, Faculty of Science, Masaryk University, Kotlářská 2, 611 37 Brno, Czech Republic Received 27 June 2007; received in revised form 12 October 2007; accepted 16 October 2007 Available online 25 October 2007 Abstract Although arsenic (As) contamination of groundwater in the Bengal Basin has received wide attention over the past decade, comparative studies of hydrogeochemistry in geologically different sub-basins within the basin have been lacking. Groundwater samples were collected from sub-basins in the western margin (River Bhagirathi sub-basin, Nadia, India; 90 samples) and eastern margin (River Meghna sub-basin; Brahmanbaria, Bangladesh; 35 samples) of the Bengal Basin. -
Amnesty International Report 2020/21
AMNESTY INTERNATIONAL Amnesty International is a movement of 10 million people which mobilizes the humanity in everyone and campaigns for change so we can all enjoy our human rights. Our vision is of a world where those in power keep their promises, respect international law and are held to account. We are independent of any government, political ideology, economic interest or religion and are funded mainly by our membership and individual donations. We believe that acting in solidarity and compassion with people everywhere can change our societies for the better. Amnesty International is impartial. We take no position on issues of sovereignty, territorial disputes or international political or legal arrangements that might be adopted to implement the right to self- determination. This report is organized according to the countries we monitored during the year. In general, they are independent states that are accountable for the human rights situation on their territory. First published in 2021 by Except where otherwise noted, This report documents Amnesty Amnesty International Ltd content in this document is International’s work and Peter Benenson House, licensed under a concerns through 2020. 1, Easton Street, CreativeCommons (attribution, The absence of an entry in this London WC1X 0DW non-commercial, no derivatives, report on a particular country or United Kingdom international 4.0) licence. territory does not imply that no https://creativecommons.org/ © Amnesty International 2021 human rights violations of licenses/by-nc-nd/4.0/legalcode concern to Amnesty International Index: POL 10/3202/2021 For more information please visit have taken place there during ISBN: 978-0-86210-501-3 the permissions page on our the year.