Neprilysin Inhibition in the Time of Precision Medicine∗
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

What Are the Roles of Metalloproteinases in Cartilage and Bone Damage? G Murphy, M H Lee
iv44 Ann Rheum Dis: first published as 10.1136/ard.2005.042465 on 20 October 2005. Downloaded from REPORT What are the roles of metalloproteinases in cartilage and bone damage? G Murphy, M H Lee ............................................................................................................................... Ann Rheum Dis 2005;64:iv44–iv47. doi: 10.1136/ard.2005.042465 enzyme moiety into an upper and a lower subdomain. A A role for metalloproteinases in the pathological destruction common five stranded beta-sheet and two alpha-helices are in diseases such as rheumatoid arthritis and osteoarthritis, always found in the upper subdomain with a further C- and the irreversible nature of the ensuing cartilage and bone terminal helix in the lower subdomain. The catalytic sites of damage, have been the focus of much investigation for the metalloproteinases, especially the MMPs, have been several decades. This has led to the development of broad targeted for the development of low molecular weight spectrum metalloproteinase inhibitors as potential therapeu- synthetic inhibitors with a zinc chelating moiety. Inhibitors tics. More recently it has been appreciated that several able to fully differentiate between individual enzymes have families of zinc dependent proteinases play significant and not been identified thus far, although a reasonable level of varied roles in the biology of the resident cells in these tissues, discrimination is now being achieved in some cases.7 Each orchestrating development, remodelling, and subsequent family does, however, have other unique domains with pathological processes. They also play key roles in the numerous roles, including the determination of physiological activity of inflammatory cells. The task of elucidating the substrate specificity, ECM, or cell surface localisation (fig 1). -

Negatively Regulated by ADAM15 TRIF-Mediated TLR3 and TLR4
TRIF-Mediated TLR3 and TLR4 Signaling Is Negatively Regulated by ADAM15 Suaad Ahmed, Ashwini Maratha, Aisha Qasim Butt, Enda Shevlin and Sinead M. Miggin This information is current as of September 27, 2021. J Immunol 2013; 190:2217-2228; Prepublished online 30 January 2013; doi: 10.4049/jimmunol.1201630 http://www.jimmunol.org/content/190/5/2217 Downloaded from Supplementary http://www.jimmunol.org/content/suppl/2013/01/30/jimmunol.120163 Material 0.DC1 References This article cites 57 articles, 20 of which you can access for free at: http://www.jimmunol.org/ http://www.jimmunol.org/content/190/5/2217.full#ref-list-1 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on September 27, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2013 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology TRIF-Mediated TLR3 and TLR4 Signaling Is Negatively Regulated by ADAM15 Suaad Ahmed, Ashwini Maratha, Aisha Qasim Butt, Enda Shevlin, and Sinead M. -

ADAM10 Site-Dependent Biology: Keeping Control of a Pervasive Protease
International Journal of Molecular Sciences Review ADAM10 Site-Dependent Biology: Keeping Control of a Pervasive Protease Francesca Tosetti 1,* , Massimo Alessio 2, Alessandro Poggi 1,† and Maria Raffaella Zocchi 3,† 1 Molecular Oncology and Angiogenesis Unit, IRCCS Ospedale Policlinico S. Martino Largo R. Benzi 10, 16132 Genoa, Italy; [email protected] 2 Proteome Biochemistry, IRCCS San Raffaele Scientific Institute, 20132 Milan, Italy; [email protected] 3 Division of Immunology, Transplants and Infectious Diseases, IRCCS San Raffaele Scientific Institute, 20132 Milan, Italy; [email protected] * Correspondence: [email protected] † These authors contributed equally to this work as last author. Abstract: Enzymes, once considered static molecular machines acting in defined spatial patterns and sites of action, move to different intra- and extracellular locations, changing their function. This topological regulation revealed a close cross-talk between proteases and signaling events involving post-translational modifications, membrane tyrosine kinase receptors and G-protein coupled recep- tors, motor proteins shuttling cargos in intracellular vesicles, and small-molecule messengers. Here, we highlight recent advances in our knowledge of regulation and function of A Disintegrin And Metalloproteinase (ADAM) endopeptidases at specific subcellular sites, or in multimolecular com- plexes, with a special focus on ADAM10, and tumor necrosis factor-α convertase (TACE/ADAM17), since these two enzymes belong to the same family, share selected substrates and bioactivity. We will discuss some examples of ADAM10 activity modulated by changing partners and subcellular compartmentalization, with the underlying hypothesis that restraining protease activity by spatial Citation: Tosetti, F.; Alessio, M.; segregation is a complex and powerful regulatory tool. -

Expression of the Disintegrin Metalloprotease, ADAM-10, In
314 Vol. 10, 314–323, January 1, 2004 Clinical Cancer Research Expression of the Disintegrin Metalloprotease, ADAM-10, in Prostate Cancer and Its Regulation by Dihydrotestosterone, Insulin-Like Growth Factor I, and Epidermal Growth Factor in the Prostate Cancer Cell Model LNCaP Daniel R. McCulloch,1 Pascal Akl,1 Conclusions: This study describes for the first time Hemamali Samaratunga,2 Adrian C. Herington,1 the expression, regulation, and cellular localization of and Dimitri M. Odorico1 ADAM-10 protein in PCa. The regulation and membrane 1 localization of ADAM-10 support our hypothesis that Hormone-Dependent Cancer Program, School of Life Sciences, ADAM-10 has a role in extracellular matrix maintenance Queensland University of Technology, Brisbane, Queensland, Australia, and 2Sullivan Nicolaides Pathology, Brisbane, Queensland, and cell invasion, although the potential role of nuclear Australia ADAM-10 is not yet known. INTRODUCTION ABSTRACT The disintegrin metalloproteases ADAMs, like the matrix Purpose: The disintegrin metalloprotease ADAM-10 is metalloproteinases (MMPs), are members of the metzincin a multidomain metalloprotease that is potentially significant (zinc-dependent metalloprotease) superfamily. To date, more in tumor progression due to its extracellular matrix-degrad- than 30 ADAMs have been characterized (1), some of which are ing properties. Previously, ADAM-10 mRNA was detected involved in diverse biological functions such as fertilization, in prostate cancer (PCa) cell lines; however, the presence of neurogenesis (2, 3), and the ectodomain shedding of growth ADAM-10 protein and its cellular localization, regulation, factors such as amyloid precursor protein and tumor necrosis and role have yet to be described. We hypothesized that factor ␣ (4, 5). -
Antibody Target for Therapeutic Inhibition Of
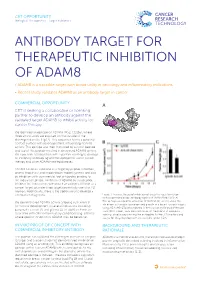
CRT OPPORTUNITY Biological Therapeutics - Target Validation ANTIBODY TARGET FOR THERAPEUTIC INHIBITION OF ADAM8 • ADAM8 is a tractable target with broad utility in oncology and inflammatory indications • Recent study validates ADAM8 as an antibody target in cancer COMMERCIAL OPPORTUNITY A CRT is seeking a collaborative or licensing partner to develop an antibody against the validated target ADAM8 to inhibit activity for cancer therapy. We identified an epitope on ADAM8 (MS2, CD156), where three amino acids are exposed on the outside of the disintegrin domain (Fig 1A). This sequence forms a potential contact surface with several proteins, influencing ADAM8 activity. This epitope was then mimicked by a cyclic peptide and use of this peptide resulted in decreased ADAM8 activity. We now seek collaboration with a partner wanting to develop an inhibitory antibody against the epitope for use in cancer therapy and other ADAM8-related diseases. ADAM8 has been validated as a target by peptide inhibition, several knock-out and knock-down model systems and also by inhibition with commercial tool antibodies binding to the indicated epitope. Inhibition of ADAM8 by our peptide inhibitor BK-1361 comes with data that validates ADAM8 as a cancer target, plus identified targets potentially useful as PD markers. Additionally, there is the opportunity to develop a companion diagnostic. Figure 1: In vivo efficacy of inhibition of breast tumour formation with a commercial tool antibody against ADAM8 (MAb 1031). A) We demonstrated ADAM8 activity as being instrumental The epitope needed for activation of ADAM8. B) and C) show the inhibition of tumour formation and growth in a breast tumour model for tumour development in several indications including using MDA-MB-231 cells injected in the mammary fat pad of female pancreatic cancer [2] and glioma [3]. -

Endogenous Regulators of Angiogenesis –
Cancer and Metastasis Reviews 19: 159–165, 2000. © 2000 Kluwer Academic Publishers. Printed in the Netherlands. Endogenous regulators of angiogenesis – emphasis on proteins with thrombospondin – type I motifs Darren Carpizo and M. Luisa Iruela-Arispe Department of Molecular, Cell and Developmental Biology, Molecular Biology Institute and Jonsson Comprehensive Cancer Center, University of California, Los Angeles, CA, USA Key words: angiogenesis, thrombospondin, proteins Abstract Angiogenesis has been acknowledged as an important requirement for growth and metastasis of tumors. Complete or partial suppression of vascular growth by a number of different strategies has been consistently associated with suppression of tumor expansion and even reduction of tumor burden. Consequently, identification of the molecular pathways of the angiogenic response has been a major focus of interest in academia and industry. The development of tumor-specific anti-angiogenic therapy was also catalyzed by the finding that inhibitors of angiogenesis appeared immune to the development of drug resistance by the tumor cells, a major restrain in current chemotherapy. Although the full identification of players and their cross-talk is still at its infancy, it appears that partial blockade of one of the steps in the angiogenesis cascade, is sufficient to affect capillary morphogenesis. Thus, suppression of specific integrin pathways or vascular endothelial growth factor signaling have been shown effective in the suppression of tumor-mediated angiogenesis and have led to subsequent initiation of clinical trials. In addition to the generation of antibodies or chemical mimetics to interfere with particular steps during vascular organization, several endogenous (or physiological) molecules have also been identified. The list of endogenous modulators of angiogenesis is growing and can offer additional and important tool for the generation of therapies to restrain tumor vascularization. -

The Disintegrin/Metalloproteinase ADAM10 Is Essential for the Establishment of the Brain Cortex
The Journal of Neuroscience, April 7, 2010 • 30(14):4833–4844 • 4833 Development/Plasticity/Repair The Disintegrin/Metalloproteinase ADAM10 Is Essential for the Establishment of the Brain Cortex Ellen Jorissen,1,2* Johannes Prox,3* Christian Bernreuther,4 Silvio Weber,3 Ralf Schwanbeck,3 Lutgarde Serneels,1,2 An Snellinx,1,2 Katleen Craessaerts,1,2 Amantha Thathiah,1,2 Ina Tesseur,1,2 Udo Bartsch,5 Gisela Weskamp,6 Carl P. Blobel,6 Markus Glatzel,4 Bart De Strooper,1,2 and Paul Saftig3 1Center for Human Genetics, Katholieke Universiteit Leuven and 2Department for Developmental and Molecular Genetics, Vlaams Instituut voor Biotechnologie (VIB), 3000 Leuven, Belgium, 3Institut fu¨r Biochemie, Christian-Albrechts-Universita¨t zu Kiel, D-24098 Kiel, Germany, 4Institute of Neuropathology, University Medical Center Hamburg Eppendorf, 20246 Hamburg, Germany, 5Department of Ophthalmology, University Medical Center Hamburg Eppendorf, 20246 Hamburg, Germany, and 6Arthritis and Tissue Degeneration Program, Hospital for Special Surgery, and Departments of Medicine and of Physiology, Systems Biology and Biophysics, Weill Medical College of Cornell University, New York, New York 10021 The metalloproteinase and major amyloid precursor protein (APP) ␣-secretase candidate ADAM10 is responsible for the shedding of ,proteins important for brain development, such as cadherins, ephrins, and Notch receptors. Adam10 ؊/؊ mice die at embryonic day 9.5 due to major defects in development of somites and vasculogenesis. To investigate the function of ADAM10 in brain, we generated Adam10conditionalknock-out(cKO)miceusingaNestin-Crepromotor,limitingADAM10inactivationtoneuralprogenitorcells(NPCs) and NPC-derived neurons and glial cells. The cKO mice die perinatally with a disrupted neocortex and a severely reduced ganglionic eminence, due to precocious neuronal differentiation resulting in an early depletion of progenitor cells. -

Strategies to Target ADAM17 in Disease: from Its Discovery to the Irhom Revolution
molecules Review Strategies to Target ADAM17 in Disease: From Its Discovery to the iRhom Revolution Matteo Calligaris 1,2,†, Doretta Cuffaro 2,†, Simone Bonelli 1, Donatella Pia Spanò 3, Armando Rossello 2, Elisa Nuti 2,* and Simone Dario Scilabra 1,* 1 Proteomics Group of Fondazione Ri.MED, Research Department IRCCS ISMETT (Istituto Mediterraneo per i Trapianti e Terapie ad Alta Specializzazione), Via E. Tricomi 5, 90145 Palermo, Italy; [email protected] (M.C.); [email protected] (S.B.) 2 Department of Pharmacy, University of Pisa, Via Bonanno 6, 56126 Pisa, Italy; [email protected] (D.C.); [email protected] (A.R.) 3 Università degli Studi di Palermo, STEBICEF (Dipartimento di Scienze e Tecnologie Biologiche Chimiche e Farmaceutiche), Viale delle Scienze Ed. 16, 90128 Palermo, Italy; [email protected] * Correspondence: [email protected] (E.N.); [email protected] (S.D.S.) † These authors contributed equally to this work. Abstract: For decades, disintegrin and metalloproteinase 17 (ADAM17) has been the object of deep investigation. Since its discovery as the tumor necrosis factor convertase, it has been considered a major drug target, especially in the context of inflammatory diseases and cancer. Nevertheless, the development of drugs targeting ADAM17 has been harder than expected. This has generally been due to its multifunctionality, with over 80 different transmembrane proteins other than tumor necrosis factor α (TNF) being released by ADAM17, and its structural similarity to other metalloproteinases. This review provides an overview of the different roles of ADAM17 in disease and the effects of its ablation in a number of in vivo models of pathological conditions. -

Regulation of Profibrotic Responses by ADAM17 Activation in High Glucose Requires Its C-Terminus and FAK Renzhong Li, Tony Wang, Khyati Walia, Bo Gao and Joan C
© 2018. Published by The Company of Biologists Ltd | Journal of Cell Science (2018) 131, jcs208629. doi:10.1242/jcs.208629 RESEARCH ARTICLE Regulation of profibrotic responses by ADAM17 activation in high glucose requires its C-terminus and FAK Renzhong Li, Tony Wang, Khyati Walia, Bo Gao and Joan C. Krepinsky* ABSTRACT and amphiregulin have been implicated in the pathogenesis of Glomerular matrix accumulation is the hallmark of diabetic diabetic kidney disease (Kefaloyianni et al., 2016; Melenhorst et al., nephropathy. The metalloprotease ADAM17 mediates high glucose 2009; Uttarwar et al., 2011). Cleavage of the renoprotective (HG)-induced matrix production by kidney mesangial cells through exopeptidase ACE2 by ADAM17 is also thought to contribute to release of ligands for the epidermal growth factor receptor. Here, diabetic kidney tubular injury (Salem et al., 2014). In diabetic mice, we study the mechanism by which HG activates ADAM17. We find a nonselective metalloprotease inhibitor decreased glomerular that the C-terminus is essential for ADAM17 activation and the sclerosis, although effects cannot be specifically attributed to profibrotic response to HG. In the C-terminus, Src-mediated Y702 inhibition of ADAM17 (Ford et al., 2013). More specific ADAM17 phosphorylation and PI3K–MEK–Erk-mediated T735 phosphorylation inhibitors, however, have been associated with adverse effects, are crucial for ADAM17 activation, both are also required for the preventing their long-term use in the treatment of diabetic HG-induced increase in cell surface -

Expression of the Disintegrin Metalloprotease, ADAM-10, In
314 Vol. 10, 314–323, January 1, 2004 Clinical Cancer Research Expression of the Disintegrin Metalloprotease, ADAM-10, in Prostate Cancer and Its Regulation by Dihydrotestosterone, Insulin-Like Growth Factor I, and Epidermal Growth Factor in the Prostate Cancer Cell Model LNCaP Daniel R. McCulloch,1 Pascal Akl,1 Conclusions: This study describes for the first time Hemamali Samaratunga,2 Adrian C. Herington,1 the expression, regulation, and cellular localization of and Dimitri M. Odorico1 ADAM-10 protein in PCa. The regulation and membrane 1 localization of ADAM-10 support our hypothesis that Hormone-Dependent Cancer Program, School of Life Sciences, ADAM-10 has a role in extracellular matrix maintenance Queensland University of Technology, Brisbane, Queensland, Australia, and 2Sullivan Nicolaides Pathology, Brisbane, Queensland, and cell invasion, although the potential role of nuclear Australia ADAM-10 is not yet known. INTRODUCTION ABSTRACT The disintegrin metalloproteases ADAMs, like the matrix Purpose: The disintegrin metalloprotease ADAM-10 is metalloproteinases (MMPs), are members of the metzincin a multidomain metalloprotease that is potentially significant (zinc-dependent metalloprotease) superfamily. To date, more in tumor progression due to its extracellular matrix-degrad- than 30 ADAMs have been characterized (1), some of which are ing properties. Previously, ADAM-10 mRNA was detected involved in diverse biological functions such as fertilization, in prostate cancer (PCa) cell lines; however, the presence of neurogenesis (2, 3), and the ectodomain shedding of growth ADAM-10 protein and its cellular localization, regulation, factors such as amyloid precursor protein and tumor necrosis and role have yet to be described. We hypothesized that factor ␣ (4, 5). -

Functional and Structural Studies of the Presequence Protease, Prep
Functional and structural studies of the Presequence protease, PreP Licentiate thesis Hans G Bäckman Supervisor: Elzbieta Glaser Department of Biochemistry and Biophysics Stockholm University 2014 2 Contents Abstract ................................................................................................................................. 5 Publications ........................................................................................................................... 6 The thesis is based on the following publications ............................................................................... 6 Abbreviations ........................................................................................................................ 7 Mitochondria and chloroplasts ............................................................................................... 8 The mitochondrial genome ................................................................................................................. 9 Function and structure of mitochondria ............................................................................................. 9 The chloroplast genome .................................................................................................................... 10 Function and structure of chloroplasts ............................................................................................. 10 Protein targeting and import into the mitochondrial matrix ........................................................... -

Angiotensin Receptor Neprilysin Inhibition in Heart Failure: Mechanistic Action and Clinical Impact
Journal of Cardiac Failure Vol. 21 No. 9 2015 Review Article Angiotensin Receptor Neprilysin Inhibition in Heart Failure: Mechanistic Action and Clinical Impact JONATHAN BUGGEY, MD,1 ROBERT J. MENTZ, MD,1,2 ADAM D. DEVORE, MD,1,2 AND ERIC J. VELAZQUEZ, MD1,2 Durham, North Carolina ABSTRACT Heart failure (HF) is an increasingly common syndrome associated with high mortality and economic burden, and there has been a paucity over the past decade of new pharmacotherapies that improve outcomes. However, recent data from a large randomized controlled trial compared the novel agent LCZ696, a dual-acting angiotensin receptor blocker and neprilysin inhibitor (ARNi), with the well estab- lished angiotensin-converting enzyme (ACE) inhibitor enalapril and found significant reduction in mortal- ity among the chronic reduced ejection fraction HF population. Preclinical and clinical data suggest that neprilysin inhibition provides beneficial outcomes in HF patients by preventing the degradation of natriuretic peptides and thereby promoting natriuresis and vasodilatation and counteracting the negative cardiorenal effects of the up-regulated renin-angiotensin-aldosterone system. Agents such as omapatrilat combined neprilysin and ACE inhibition but had increased rates of angioedema. Goals of an improved safety profile provided the rationale for the development of the ARNi LCZ696. Along with significant reductions in mortality and hospitalizations, clinical trials suggest that LCZ696 may improve surrogate markers of HF severity. In this paper, we review the preclinical and clinical data that led to the develop- ment of LCZ696, the understanding of the underlying mechanistic action, and the robust clinical impact that LCZ696 may have in the near future.