Reticular Hyperpigmentation on the Lower Legs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Phytophotodermatitis
PHYTOPHOTODERMATITIS http://www.aocd.org Phytophotodermatitis (PPD) is a cutaneous phototoxic reaction that occurs following contact with certain plants. The reaction is stimulated by skin exposure to light sensitizing botanical substances known as furanocoumarins followed by exposure to long wave ultraviolet light in sunlight. Furanocoumarins are present in plants such as, lemons, limes, mangos, parsley and many weeds. Psoralen is the active particle in furanocoumarins. Upon UVA radiation exposure from sunlight, psoralens within the skin react with molecular oxygen and form reactive oxygen species that induce destruction of skin cells and cause an inflammatory reaction. PPD is most common in the spring and summer, as psoralen concentrations are the highest and outdoor activities under the sun are increased. Exposure to plants or solutions such as lemon or lime juice, lead to bizarre patterns of distribution. Streaks may be present from brushing against a plant or haphazard lines from juice. Common presentations are on the upper lip from drinking citrus beverages, from spilled beverages, or even from wiping juice onto exposed skin to dry the hands. This is often referred to as “Margarita Rash”. The rash begins within 24 hours and can peak at 72 hours. The distribution of skin reactions is sharply limited to areas exposed to sun. Skin findings can consist of non-pruritic reactions, mild redness with or without erosions, to severe blistering. Redness can persist for weeks to months. Hyperpigmentation appears 1-2 weeks later and can last up to months. The distribution to sun exposed areas and pattern aid in diagnosis. History and a high index of suspicion is key to diagnosing PPD. -

UCSF Fresno, Medical Educakon Program J Heppner MD, H Lee MD
(—THIS SIDEBAR DOES NOT PRINT—) QUICK START (cont.) DESIGN GUIDE Phytophotoderma/s Resul/ng From Citrus Exposure: A Pediatric Case Series from Central California How to change the template color theme This PowerPoint 2007 template produces a 36”x48” You can easily change the color theme of your poster by going to the presentation poster. You can use it to create your research DESIGN menu, click on COLORS, and choose the color theme of your poster and save valuable time placing titles, subtitles, text, J Heppner MD, H Lee MD, P Armenian MD choice. You can also create your own color theme. and graphics. UCSF Fresno, Medical Educaon Program We provide a series of online tutorials that will guide you through the poster design process and answer your poster production questions. To view our template tutorials, go online to PosterPresentations.com and click on HELP DESK. You can also manually change the color of your background by going to Introduc>on Case Series Descripon Case Series Descripon Discussion VIEW > SLIDE MASTER. After you finish working on the master be sure to When you are ready to print your poster, go online to Lisbon Lemon (Citrus limon) Key Lime (Citrus aurantifolia) go to VIEW > NORMAL to continue working on your poster. PosterPresentations.com Psoralens belong to the furocoumarin family, and cause This is a consecutive-patient case series of five girls Few phytophotodermatitis outbreaks demonstrate phytophotodermatitis when coupled with ultraviolet aged 7-11 transferred from an outside facility for such severity in multiple pediatric patients, How to add Text Need assistance? Call us at 1.510.649.3001 light exposure. -

Dermatological Indications of Disease - Part II This Patient on Dialysis Is Showing: A
“Cutaneous Manifestations of Disease” ACOI - Las Vegas FR Darrow, DO, MACOI Burrell College of Osteopathic Medicine This 56 year old man has a history of headaches, jaw claudication and recent onset of blindness in his left eye. Sed rate is 110. He has: A. Ergot poisoning. B. Cholesterol emboli. C. Temporal arteritis. D. Scleroderma. E. Mucormycosis. Varicella associated. GCA complex = Cranial arteritis; Aortic arch syndrome; Fever/wasting syndrome (FUO); Polymyalgia rheumatica. This patient missed his vaccine due at age: A. 45 B. 50 C. 55 D. 60 E. 65 He must see a (an): A. neurologist. B. opthalmologist. C. cardiologist. D. gastroenterologist. E. surgeon. Medscape This 60 y/o male patient would most likely have which of the following as a pathogen? A. Pseudomonas B. Group B streptococcus* C. Listeria D. Pneumococcus E. Staphylococcus epidermidis This skin condition, erysipelas, may rarely lead to septicemia, thrombophlebitis, septic arthritis, osteomyelitis, and endocarditis. Involves the lymphatics with scarring and chronic lymphedema. *more likely pyogenes/beta hemolytic Streptococcus This patient is susceptible to: A. psoriasis. B. rheumatic fever. C. vasculitis. D. Celiac disease E. membranoproliferative glomerulonephritis. Also susceptible to PSGN and scarlet fever and reactive arthritis. Culture if MRSA suspected. This patient has antithyroid antibodies. This is: • A. alopecia areata. • B. psoriasis. • C. tinea. • D. lichen planus. • E. syphilis. Search for Hashimoto’s or Addison’s or other B8, Q2, Q3, DRB1, DR3, DR4, DR8 diseases. This patient who works in the electronics industry presents with paresthesias, abdominal pain, fingernail changes, and the below findings. He may well have poisoning from : A. lead. B. -

Five Cases of Phytophotodermatitis Caused by Fig Leaves and Relevant Literature Review
JH Son, et al pISSN 1013-9087ㆍeISSN 2005-3894 Ann Dermatol Vol. 29, No. 1, 2017 https://doi.org/10.5021/ad.2017.29.1.86 CASE REPORT Five Cases of Phytophotodermatitis Caused by Fig Leaves and Relevant Literature Review Jin-Hwa Son1, Hyunju Jin1, Hyang-Suk You1, Woo-Haing Shim1, Jeong-Min Kim1, Gun-Wook Kim1, Hoon-Soo Kim1, Hyun-Chang Ko1, Moon-Bum Kim1,2, Byung-Soo Kim1,2 1Department of Dermatology, School of Medicine, Pusan National University, 2Biomedical Research Institute, Pusan National University Hospital, Busan, Korea Phytophotodermatitis is a condition caused by sequential ex- INTRODUCTION posure to photosensitizing substances present in plants fol- lowed by ultraviolet light. Several plants (e.g., limes, celery, Phytophotodermatitis is a condition caused by sequential fig, and wild parsnip) contain furocoumarin compounds exposure to certain photosensitizing substance present in (psoralens). It is important for dermatologists to be aware of plants followed by sunlight. Many common plants, includ- phytophotodermatitis because it may be misdiagnosed as ing citrus fruits, celery, and wild parsnip contain such cellulitis, tinea, or allergic contact dermatitis. We present photosensitizers (e.g., furocoumarins). five patients with a sharply defined erythematous swollen Herein, we present five cases of phytophotodermatitis af- patch with bullae on both feet. They described soaking their ter soaking feet in fig leaves decoction. feet in a fig leaves decoction to treat their underlying derma- We present two purposes of this report: the first is to bring tologic diseases. Within 24 hours, all patients had a burning attention to this type of dermatitis. It is important for der- sensation in their feet, and erythema and edema had devel- matologists to recognize phytophotodermatitis as it may oped on the feet dorsa with exception of the portion of the sometimes be misdiagnosed as other skin conditions in- skin covered by the sandals. -

Generalized Hyperpigmentation After Pyrimethamine Use
Our Dermatology Online Case Report GGeneralizedeneralized hhyperpigmentationyperpigmentation aafterfter ppyrimethamineyrimethamine uusese Ann Sterkens1,2, Vasiliki Siozopoulou1,2, Evelyne Mangodt1,2, Julien Lambert1,2, An Bervoets1,2 1Faculty of Medicine, University of Antwerp, Wilrijk, Belgium, 2Dermatology Department, University Hospital Antwerp, Edegem, Belgium Corresponding author: Dr. Ann Sterkens, E-mail: [email protected] ABSTRACT A 44-year old trans woman of Asian origin presented with generalized hyperpigmentation all over her body for four weeks. Six months before, she presented at the emergency department with motor ataxia and further investigation revealed a new diagnosis of HIV, cerebral toxoplasmosis with cerebral edema and latent syphilis. Two months later she presented with encephalitis: CMV and TBC were diagnosed. At that moment, a lot of new medication was started. Skin biopsy was compatible with a medical eruption. Hyperpigmentation was most probably caused by pyrimethamine, which was given for the treatment of toxoplasmosis. Pyrimethamine was stopped and changed into trimethoprim and sulfamethoxazole. Reevaluation after two months showed fading of the hyperpigmentation, especially in the face, which points towards the right diagnosis. Key words: Generalized hyperpigmentation; Toxoplasmosis; Pyrimethamine; HIV, Trimethoprim; Sulfamethoxazole INTRODUCTION patients. Skin biopsy is not a routine examination but can be done when the clinical diagnosis is not clear. Hyperpigmentation is the darkening of the skin. Most of the time it is caused by an increased melanin CASE REPORT deposition, and in rare cases it is due to deposition of pigments like iron or hemosiderin. Hyperpigmentation A 44-year old transwoman of Asian origin, who can be well circumscribed (lentigines, ephilides, recently came to Belgium, presented with generalized maturational hyperpigmentation, melasma, fixed hyperpigmentation all over the body, also in sun- drug eruption,…) or diffuse. -

Fotossensibilidade Induzida Por Fármacos Drug-Induced
Revista SPDV 74(2) 2016; Fotossensibilidade por fármacos; Miguel Gouveia, Ana Gameiro, Inês Coutinho, Margarida Gonçalo. Educação Médica Contínua Fotossensibilidade Induzida por Fármacos Miguel Gouveia1, Ana Gameiro1, Inês Coutinho2, Margarida Gonçalo3 1Médico interno do Internato Complementar de Dermatovenereologia, Serviço de Dermatologia, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal/Resident, Dermatology and Venereology, Centro Hospitalar e Universitário de Coimbra, Portugal 2Assistente Hospitalar de Dermatovenereologia, Serviço de Dermatologia, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal/Consultant of Dermatology, Dermatology Department, Centro Hospitalar e Universitário de Coimbra, Portugal 3Assistente Hospitalar Graduado Sénior de Dermatologia, Serviço de Dermatologia, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal e Professor Auxiliar da Faculdade de Medicina da Universidade de Coimbra, Coimbra, Portugal/Senior Graduate Assistant in Dermatology, Dermatology Department, Centro Hospitalar e Universitário de Coimbra, Portugal and Professor of Dermatology, Dermatology Department, Centro Hospitalar Universitário de Coimbra, Portugal RESUMO – A fotossensibilidade induzida por fármacos traduz uma resposta cutânea anormal à luz em indivíduos expostos a um fár- maco, os quais, na sua ausência, tolerariam o mesmo grau de fotoexposição. Pode ocorrer como uma reação aguda ou retardada, assumindo características clínicas polimórficas que variam desde a queimadura solar exagerada até aspectos de fotoonicólise, pseudo- -porfíria, pigmentação, eczema agudo e lúpus eritematoso cutâneo. Os autores descrevem os fármacos mais frequentemente envol- vidos neste tipo de reações e as formas clínicas mais frequentes e discutem o possível contributo destes fármacos na potenciação da fotocarcinogénese. O reconhecimento d estes padrões clínicos de fotossensibilidade e dos fármacos responsáveis é fundamental para a evicção do fármaco causal e consequente melhoria ou resolução da reação de fotossensibilidade. -

Boards' Fodder
boards’ fodder Plants By Cynthia Chen, DO ALLERGIC CONTACT DERMATITIS Common Name Formal Name Inciting Agents Garlic Alliaceae Chive Alliaceae Diallyl Sulfide, Allylpropyl Disulfide, Allicin Onions Alliaceae, Allium cepa Peruvian lily Alstromeria spp Tuliposide A Poison ivy Anacardiaceae, Toxicodendron genus Poison oak Anacardiaceae, Toxicodendron genus Pentadecacatechol in oleoresin (urushiol) Poison sumac Anacardiaceae, Toxicodendron genus Japanese lacquer tree Anacardiaceae, Toxicodendron verniciflua Mango Anacardiaceae, Mangifera indica Resorcinols Brazilian pepper tree Anacardiaceae, Schinus terebinthifolius Indian marking tree Anacardiaceae, Semecarpus anacardium Ragweed Asteraceae (Compositae), Ambrosia spp Artichokes Asteraceae (Compositae), Cynara scolymus Chrysanthemum Asteraceae (Compositae), Dendranthema cultivars Sesquiterpene lactone Pyrethrum Asteraceae (Compositae), Tanacetum cinerarilifolium Feverfew Asteraceae (Compositae), Tanacetum parthenium Gingko tree Ginkgoaceae Urushiol cross-reacting chemicals Tea tree Melaleuca alternifolia Terpinolene, ascaridol, alpha-terpinene, 1,2,4-trihydroxy menthane Longleaf pine Pinus palustrius Colophony Primrose Primulaceae, Primula obconica Primin Tulips Tulipa spp Tuliposide A, Tuliposide B CHEMICAL IRRITANT DERMATITIS Common Name Formal Name Inciting Agents Century plant Agave Americana Calcium oxalate, saponins (latex throughout plant) Garlic Alliaceae, Allium sativum Thiocyanates Daffodil Amaryllidaceae, Narcissus spp Calcium oxalate Cashew tree Anacardiaceae, Anacardium occidentale -

Skin Rash on the Upper Limbs
CLINICAL Skin rash on the upper limbs Case studies Diogo Pereira Patricia Machado Paulo Morais Two gardeners, a male, 37 years of age Question 3 (patient 1) and his brother, 33 years of age How can we make the correct diagnosis of this (patient 2), presented with a 1-day history of disease? slightly painful, unusual streaks and linear erythematous vesiculobullous plaques, with localised oedema, located on their forearms Question 4 (Figures 1A and 1B). On the previous day, What differential diagnoses would you consider? with blue skies and sunshine, they had been picking parsnips. Question 5 A healthy male bartender, 19 years of age What therapeutic measures would you (patient 3), who was preparing margaritas recommend? at a beach bar, presented with an erythematous vesicular rash, associated with Answer 1 burning sensation, on his right ante-cubital The diagnosis in all these presentations is fossa (Figure 1C). phytophotodermatitis (PPD), a common cutaneous A previously healthy woman, 39 years of age phototoxic inflammatory eruption resulting from (patient 4), presented with erythematous and contact with plant-derived photosensitising mildly hyper-pigmented lesions in a bizarre compounds, generally furocoumarins (psoralens), pattern on her forearms (Figure 1D). A week followed by exposure to sunlight (especially before, she had been preparing lime juice for ultraviolet A 320–380 nm).1,2 her children at a table next to their outdoor swimming pool. On the following days she Answer 2 developed pain, oedema and tense bullae PPD is caused by at least four different plant in that location, with little improvement following application of cream containing families: Apiaceae (formerly Umbelliferae), 1–3 menthol and steroid. -
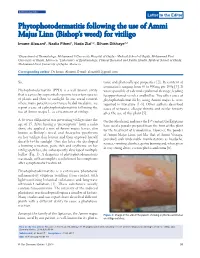
Phytophotodermatitis Following the Use of Ammi Majus Linn (Bishop’S Weed) for Vitiligo
Our Dermatology Online Letter to the Editor PPhytophotodermatitishytophotodermatitis ffollowingollowing tthehe uusese ooff AAmmimmi MMajusajus LLinninn ((Bishop’sBishop’s wweed)eed) fforor vvitiligoitiligo Imane Alouani1, Nadia Fihmi1, Nada Zizi1,2, Siham Dikhaye1,2 1Department of Dermatology, Mohammed 6 University Hospital of Oujda - Medical School of Oujda, Mohammed First University of Oujda, Morocco, 2Laboratory of Epidemiology, Clinical Research and Public Health, Medical School of Oujda, Mohammed First University of Oujda, Morocco Corresponding author: Dr. Imane Alouani, E-mail: [email protected] Sir, toxic and photo-allergic properties [2]. Its content of coumarin is ranging from 50 to 900mg per 100g [3]. It Phytophotodermatitis (PPD) is a well-known entity was responsible of a dermal-epidermal cleavage, leading that is causes by sequential exposure to certain species to apparition of vesicles and bullae. Two other cases of of plants and then to sunlight. In our social context phytophotodermatitis by using Ammi majus L. were where many patients resort to use herbal medicine, we reported in literature [1-4]. Other authors described report a case of a phytophotodermatitis following the cases of urticaria, allergic rhinitis and ocular toxicity use of Ammi majus L. as a treatment of vitiligo. after the use of this plant [5]. A 46 years old patient was presenting vitiligo since the On the other hand, and since the 13th century, the Egyptians age of 15. After having a “prescription” from a radio have used a powder prepared from the fruit of this plant show, she applied a mix of Ammi majus leaves, also for the treatment of leukodermas. However, the powder known as Bishop’s weed, and Anacyclus pyrethrum of Ammi Majus Linn, just like that of Ammi Visnaga, on her vitiligo skin lesions and then exposed herself provoked such undesirable manifestations as headache, directly to the sunlight. -

Phytophotodermatitis Related to Carrot Extract-Containing Sunscreen
Volume 24 Number 1 | January 2018 Dermatology Online Journal || Letter DOJ 24 (1): 20 Phytophotodermatitis related to carrot extract-containing sunscreen SS Bosanac1, AK Clark1, RK Sivamani2,3 MD MS CAT Affiliations: 1School of Medicine, University of California Davis, Sacramento, California, 2Department of Dermatology, University of California Davis, Sacramento, California, 3Department of Biological Sciences, California State University Sacramento, Sacramento, California Corresponding Author: Raja Sivamani MD MS CAT, Department of Dermatology, University of California, Davis, 3301 C Street, Suite 1400, Sacramento, CA 95816, Email: [email protected] Abstract A recent study measured the total furocoumarin concentration in various foods and beverages and Phytophotodermatitis is a clinical diagnosis from showed that grapefruit juice (95341 ng/g), fresh phototoxicity of the skin induced by contact with parsley (23215 ng/g), grapefruits (21858 ng/g), lime plants or their extracts. Phytophotodermatitis may juice (14580 ng/g), limes (9151 ng/g), and lemon present with burning, erythema, patches, plaques, juice (1561 ng/g) had the greatest concentration vesicles, bullae, or hyperpigmented patches in well- of furocoumarins [4]. Additional foods with high demarcated and unusual shapes. Inquiring about furocoumarin concentration included celeriac (also occupation, hobbies, and plant or plant extract known as turnip-rooted celery, celery root, or knob contact is essential to establishing the diagnosis. celery), (396 ng/g), parsnips (335 ng/g), and carrots Herein we present a case of phytophotodermatitis (68 ng/g), [4]. after use of carrot extract-containing sunscreen presenting as a hyperpigmented patch in a geometric Case Synopsis distribution with accentuation of pigment within the A healthy, 32-year-old woman presented to dynamic rhytides. -

Contact Dermatitis: a Great Imitator
CID-07389; No of Pages 17 Clinics in Dermatology (xxxx) xx,xxx Contact dermatitis: a great imitator Ömer Faruk Elmas,MDa,⁎, Necmettin Akdeniz,MDb, Mustafa Atasoy,MDc, Ayse Serap Karadag,MDb aDepartment of Dermatology, Faculty of Medicine, Ahi Evran University, Kırşehir, Turkey bDepartment of Dermatology, Faculty of Medicine, Istanbul Medeniyet University, Istanbul, Turkey cDepartment of Dermatology, Kayseri City Hospital, Health Science University, Kayseri, Turkey Abstract Contact dermatitis (CD) refers to a group of cutaneous diseases caused by contact with allergens or irritants. It is characterized by different stages of an eczematous eruption and has the ability to mimic a wide variety of dermatologic conditions, including inflammatory dermatitis, infectious conditions, cutaneous lymphoma, drug eruptions, and nutritional deficiencies. Irritant CD and allergic CD are the two main presen- tations of the disease. The diagnosis is based on a detailed history, physical examination, and patch testing, if necessary. Knowing the conditions mimicked by CD should improve the accuracy of the diagnosis. Avoid- ing the causative substances and taking preventive measures are necessary for the treatment. © 2019 Elsevier Inc. All rights reserved. Introduction Epidemiology Contact dermatitis (CD) describes a group of skin diseases CD can be seen at any age, and its estimated prevalence caused by contact allergens or irritant substances. CD is ranges from 1.7% to 6.3% in various published studies.3 It is characterized by an eczematous eruption and can imitate many more common in urban areas, with the incidence being higher dermatologic conditions.1,2 Irritant contact dermatitis (ICD) in women and the elderly.3 Many studies, however, suggest and allergic contact dermatitis (ACD) are considered as the that sex and age cannot be considered as independent risk two subgroups of the entity. -

Pediatric Blistering Diseases MSU/Beaumont Health Dermatology Residency Program
Pediatric Blistering Diseases MSU/Beaumont Health Dermatology Residency Program Matthew Laffer, DO & Dustin Portela, DO PGY-4 Chelsea Duggan, DO & Peter Jajou, DO PGY-3 Sonam Rama, DO & Rachel Cetta, DO PGY-2 Steven Grekin, DO Program Director Disclosures • No conflicts of interest to disclose Overview • Infectious Disease • Drug Related Disorders • Hereditary Disorders • Autoimmune Conditions • Miscellaneous Disorders INFECTIOUS Staphylococcus Scalded Skin Syndrome • Clinical Presentation • Fever, skin tenderness and erythema in groin folds, axillary regions, nose, that leads to a generalized superficial exfoliative dermatitis and bullae • +Nikolsky sign. Perioral crusting and fissuring http://medlibes.com/entry/staphylococcal-scalded-skin-syndrome Staphylococcus Scalded Skin Syndrome • Pathogenesis • Staphylococcus aureus group 2 phage (71) infects child at a distant site • Exfoliative toxins/Epidermolytic toxins A and B (ET-A, ET-B) bind to desmoglein-1 superficial bullae within the granular layer (subcorneal) • ET is a unique serine protease that shows lock and key specificity to desmoglein -11-2 • Diagnosis • Mainly clinical • Culture of the bullae will be NEGATIVE. Must culture site of initial infection • Treatment • Supportive care: IVF!! • Dicloxacillin Bullous Impetigo • Clinical Presentation • Flaccid bullae which rupture and leave honey colored crust behind • No surrounding erythema • Can have systemic manifestations such as malaise, diarrhea http://dermatologyoasis.net/bullous-impetigo-2/ http://www.adhb.govt.nz/newborn/TeachingResources/Dermatology/InfectiveLesions.htm