Prevalence of Anemia in Pregnancy at District Shaheed Benazir Abad, Sindh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Sustainable Development of the China Pakistan Economic Corridor: Synergy Among Economic, Social, and Environmental Sustainability
sustainability Article The Sustainable Development of the China Pakistan Economic Corridor: Synergy among Economic, Social, and Environmental Sustainability Muhammad Awais 1 , Tanzila Samin 2 , Muhammad Awais Gulzar 3,* and Jinsoo Hwang 4,* 1 Department of Data Science & Engineering Management, School of Management, Zhejiang University, Hangzhou 310058, China; [email protected] 2 School of Business Management, NFC Institute of Engineering & Fertilizer Research, Faisalabad 38000, Pakistan; [email protected] 3 Waikato Management School, The University of Waikato, Hamilton 3240, New Zealand 4 Department of Food Service Management, Sejong University, Seoul 143-747, Korea * Correspondence: [email protected] (M.A.G.); [email protected] (J.H.); Tel.: +8615558031661 (M.A.G.); +82-2-3408-4072 (J.H.) Received: 11 October 2019; Accepted: 3 December 2019; Published: 9 December 2019 Abstract: This case study focuses on how economic, social and environmental factors synergize for sustainable development, and relates to fundamental speculations, looking to unclutter a query-encompassing view of the China Pakistan Economic Corridor (CPEC). This study is explanatory in nature, and identifies, recognizes, and discusses the social dispositions and fundamental sustainability dimensions related to sustainable development. Three fundamental sustainability dimensions—economic, social and environmental—are incorporated in connection with the CPEC to explore sustainable development. We submit an inclusive viewpoint of the CPEC, towards the -
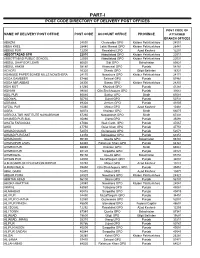
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

Spatio-Temporal Changes in Economic Development: a Case Study of Sindh Province
Karachi University Journal of Science, 2012, 40, 25-30 25 Spatio-temporal Changes in Economic Development: A case study of Sindh Province Razzaq Ahmed1 and Khalida Mahmood2,* 1Department of Geography, Federal Urdu University of Arts Sciences and Technology, Karachi and 2Department of Geography, University of Karachi, Karachi, Pakistan Abstract: This study has been conducted at a time when Pakistan is passing through an important phase of economic development and reconstruction. Devolution has become an important aspect of the planning and decision making process. Decentralization is being emphasized by both public and private sectors of development. In such a situation, present study focuses on the evaluation of the past and present patterns of the levels of development in various districts of the province of Sindh. This research will certainly contribute to an understanding of the development patterns in the province. Key Words: composite index, level of development, ranking, socio-economic inequality, Z-score. INTRODUCTION METHODOLOGICAL FRAMEWORK Sindh has experienced considerable urbanization since To measure the level of development of the districts of independence in 1947, which has resulted in the explosive Sindh, twelve variables have been employed on thirteen 1 growth of urban centers like Karachi, Hyderabad and districts of 1981 and sixteen districts of 1998 . These Sukkur. The growth of Karachi in particular has been variables are non-agricultural labor force, employment in phenomenal. Its exceptional growth as compared to the rest manufacturing, immigration, own farm, cultivated area, of Sindh, which is basically rural in nature, brings out unique population potential, manufacturing value added (rupees per patterns of socio-economic inequality. -

Spatio-Temporal Distribution of Aerosol and Cloud Properties Over Sindh Using MODIS Satellite Data and a HYSPLIT Model
Aerosol and Air Quality Research, 15: 657–672, 2015 Copyright © Taiwan Association for Aerosol Research ISSN: 1680-8584 print / 2071-1409 online doi: 10.4209/aaqr.2014.09.0200 Spatio-Temporal Distribution of Aerosol and Cloud Properties over Sindh Using MODIS Satellite Data and a HYSPLIT Model Fozia Sharif1, Khan Alam2,3*, Sheeba Afsar1 1 Department of Geography, University of Karachi, Karachi 75270, Pakistan 2 Institute of Space and Planetary Astrophysics, University of Karachi, Karachi 75270, Pakistan 3 Department of Physics, University of Peshawar, Peshawar 25120, Pakistan ABSTRACT In this study, aerosols spatial, seasonal and temporal variations over Sindh, Pakistan were analyzed which can lead to variations in the microphysics of clouds as well. All cloud optical properties were analyzed using Moderate Resolution Imaging Spectroradiometer (MODIS) data for 12 years from 2001 to 2013. We also monitored origin and movements of air masses that bring aerosol particles and may be considered as the natural source of aerosol particles in the region. For this purpose, the Hybrid Single Particle Lagrangian Integrated Trajectory (HYSPLIT) model was used to make trajectories of these air masses from their sources. Aerosol optical depth (AOD) high values were observed in summer during the monsoon period (June–August). The highest AOD values in July were recorded ranges from 0.41 to 1.46. In addition, low AOD values were found in winter season (December–February) particularly in December, ranges from 0.16 to 0.69. We then analyzed the relationship between AOD and Ångström exponent that is a good indicator of the size of an aerosol particle. -

Panel Hospitals
LAHORE HOSPITALS SERIAL NAME OF HOSPITAL ADDRESS TELEPHONE # NO. 1 Akram Eye Hospital Main Boulevard Defence Road Lahore. 042-36652395-96 2 CMH Hospital CMH Lahore Cantt., Lahore 042-6699111-5 3 Cavalry Hospital 44-45, Cavalry Ground Lahore Cantt. 042-36652116-8 4 Family Hospital 4-Mozang Road Lahore 042-37233915-8 5 Farooq Hospital 2 Asif Block, Main Boulevard Iqbal Town, Lahore 042-37813471-5 6 Fauji Foundation Bedian Road Lahore Cantt. 042-99220293 7 Gulab Devi Hospital Ferozepur Road Lahore 042-99230247-50 8 Ittefaq Hospital Near H. Block Model Town, Lahore 042-35881981-8 9 Masood Hospital 99, Garden Block, Garden Town, Lahore 042-35881961-3 10 Prime Care Hospital Main Boulevard Defence Lahore 042-36675123-4 11 Punjab Institute of Cardiology Jail Road Lahore. 042-99203051-8 12 Punjab Medical Centre 5, Main boulevard, Jail Road, Lahore 042-35753108-9 13 Laser Vision Eye Hospital 95-K, Model Town, Lahore 042-35868844-35869944 14 Sarwat Anwar Hospital 2, Tariq block Garden Town, Lahore 042-35869265-6 15 Shalimar Hospital Shalimar Link Road, Mughalpura Lahore 042-36817857-60, 111205205 16 Rasheed Hospital Branch 1, Main Boulevard Defence Lahore 042-336673192-33588898 Branch 2, Garden Town Lahore. 17 Orthopedic Medical Complex & Hospital Opposite Kinnarid College Jail Road, Lahore 042-37551335-7579987 18 National Hospital & Medical Centre 132/3, L-Block, LCCHS Lahore Cantt. 042-35728759-60 F: 042-35728761 19 Army Cardiac Centre Lahore Cantt. 20 Dental Aesthetics Clinic 187-Y, Block D.H.A., Lahore – Pakistan 042-35749000 21 Sana Dental Aesthetics 153-DD, CCA Phase-IV, DHA Lahore 042-37185861-2 CONSULTANTS 1 Cavalry Dental Clinic 26, Commercial Area, Cavalry Ground Lahore 042-36610321 2 Dr. -

Federal Capital, Islamabad Punjab Province
APPROVED PUBLIC SECTOR UNIVERSITIES / COLLEGES & THEIR CAMPUSES* Federal Capital, Islamabad Sr. # Universities / Colleges Designated Branches 1 Air University, Islamabad. Foreign Office Branch Islamabad 2 Bahria University, Islamabad. Foreign Office Branch Islamabad 3 COMSATS Institute of Information Technology, Islamabad. Foreign Office Branch Islamabad 4 Federal Urdu University of Arts, Sci. & Tech., Islamabad. Foreign Office Branch Islamabad 5 International Islamic University, Islamabad Foreign Office Branch Islamabad 6 National University of Medical Sciences, Islamabad Foreign Office Branch Islamabad 7 National University of Modern Languages, Islamabad. Foreign Office Branch Islamabad 8 National University of Science & Technology, Islamabad Foreign Office Branch Islamabad 9 National Defence University, Islamabad Foreign Office Branch Islamabad 10 Pakistan Institute of Engineering & Applied Sciences, Islamabad Foreign Office Branch Islamabad 11 Pakistan Institute of Development Economics (PIDE) Islamabad Foreign Office Branch Islamabad 12 Quaid-e-Azam University, Islamabad Foreign Office Branch Islamabad 13 Institute of Space Technology, Islamabad. Foreign Office Branch Islamabad 14 Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad Foreign Office Branch Islamabad Punjab Province 1 Allama Iqbal Medical College, Lahore Main Branch Lahore. 2 Fatima Jinnah Medical College for Women, Lahore Main Branch Lahore. 3 Government College University, Lahore Main Branch Lahore. 4 King Edward Medical College, Lahore Main Branch Lahore. 5 Kinnaird College for Women, Lahore Main Branch Lahore. 6 Lahore College for Women University, Lahore. Main Branch Lahore. 7 National College of Arts, Lahore. Main Branch Lahore. 8 University of Education, Lahore. Main Branch Lahore. 9 University of Health Sciences, Lahore Main Branch Lahore. 10 University of Veterinary and Animal Sciences, Lahore. Main Branch Lahore. Sr. # Universities / Colleges Designated Branches 11 Virtual University of Pakistan, Lahore. -

Public Sector Development Programme 2021-22
GOVERNMENT OF PAKISTAN PUBLIC SECTOR DEVELOPMENT PROGRAMME 2021-22 PLANNING COMMISSION MINISTRY OF PLANNING, DEVELOPMENT & SPECIAL INITIATIVES June, 2021 PREFACE Public Sector Development Programme (PSDP) is an important policy instrument aiming to achieve sustainable economic growth and socioeconomic objectives of the government. The outgoing fiscal year PSDP was made with a particular focus on strengthening the health sector and creating economic opportunities to combat widespread disruptions caused by COVID-19 pandemic. As a result of efficient and well-coordinated management of the pandemic, the economy showed signs of recovery and economic growth stood at 3.94% during FY 2020-21. In the upcoming year 2021-22, the priority of the Government is to further spur economic activities. Therefore, the PSDP in 2021-22 has been enhanced by 38% from Rs 650 billion in FY 2020-21 to Rs. 900 billion (including foreign aid of Rs 100 billion). The focus of PSDP 2021-22 is on improving transport and communication facilities with special emphasis on inter-provincial and regional connectivity, investment on building large dams and water conservation systems as per the National Water Policy, augmenting and strengthening health sector infrastructure and service delivery, improving access to higher education, social protection, increasing employment and livelihood opportunities, reducing regional disparities, mitigating effects of climate change, building knowledge economy, enhancing agricultural productivity & ensuring food security and supporting Public Private Partnership initiatives through providing Viability Gap funding. Special Development Packages have been initiated under the Regional Equalization Programme to ensure the development of the deprived areas to bring them at par with other developed regions of the country. -

PESA-DP-Shaheed Benazirabad.Pdf
Dalel Dero Fort, District Shaheed Benazirabad, Sindh “Disaster risk reduction has been a part of USAID’s work for decades. ……..we strive to do so in ways that better assess the threat of hazards, reduce losses, and ultimately protect and save more people during the next disaster.” Kasey Channell, Acting Director of the Disaster Response and Mitigation Division of USAID’s Office of U.S. Foreign Disas ter Ass istance (OFDA) PAKISTAN EMERGENCY SITUATIONAL ANALYSIS District Shaheed Benazirabad September 2014 “Disasters can be seen as often as predictable events, requiring forward planning which is integrated in to broader de velopment programs.” Helen Clark, UNDP Administrator, Bureau of Crisis Preven on and Recovery. Annual Report 2011 Disclaimer iMMAP Pakistan is pleased to publish this district profile. The purpose of this profile is to promote public awareness, welfare, and safety while providing community and other related stakeholders, access to vital information for enhancing their disaster mitigation and response efforts. While iMMAP team has tried its best to provide proper source of information and ensure consistency in analyses within the given time limits; iMMAP shall not be held responsible for any inaccuracies that may be encountered. In any situation where the Official Public Records differs from the information provided in this district profile, the Official Public Records should take as precedence. iMMAP disclaims any responsibility and makes no representations or warranties as to the quality, accuracy, content, or completeness of any information contained in this report. Final assessment of accuracy and reliability of information is the responsibility of the user. iMMAP shall not be liable for damages of any nature whatsoever resulting from the use or misuse of information contained in this report. -

Pakistan • Monsoon Floods Situation Report #12 14 August 2010
Pakistan • Monsoon Floods Situation Report #12 14 August 2010 This report was issued by UNOCHA Pakistan. It covers the period from 12 to 14 August. The next report will be issued on or around 16 August. I. HIGHLIGHTS/KEY PRIORITIES • Rates of diarrheal disease continue to increase in affected areas; ensuring access to clean water is a top priority • The situation in Sindh has continued to worsen, with 300,000 people evacuated from Jacobabad district on 13 August in advance of a second surge of floodwaters • Though the scale of the floods disaster continues to expand, just 20% of funding requirements set out in the Pakistan Initial Floods Response Emergency Plan have so far been covered II. Situation Overview Latest Government estimates put the number of people affected by the floods at almost 14.5 million (National and Provincial Disaster Management Authorities, 13 August). Assessments to establish the degree to which affected populations are in need of immediate humanitarian assistance continue. The official death toll has risen to 1,384, with 1,680 people reported as injured. Over 722,000 houses have been either damaged or destroyed. The situation in Sindh Province in the South has deteriorated, with both the first and second waves of floods along the Indus River now moving through parts of the province. Latest Government estimates indicate that 1.5 million people have been affected. This number is expected to rise further. Large parts of Upper Sindh are underwater. The Pakistan Meteorological Department has warned of exceptionally high flood levels on the Indus at Guddu and Sukkur, threatening renewed inundation in Khairpur, Jacobabad, Ghotki, Sukker, Larkana, Nawabshah, Hyderabad and Naushahro Feroze districts, all of which have been badly affected by the first wave of flooding. -

Pakistan Bait-Ul-Mal
PAKISTAN BAIT-UL-MAL National Center(s) for Rehabilitation of Child Labour (NCsRCL) Province Khyber Pakhtunkhwa S# District Address of NCsRCL 1 Peshawar Pattan Colony, Near Ghalla Godown, Kohat Road Tel:0332-9211201 2 Nowshera Near Shah Gul Baba Arat, Mardan Road, Nowshera Klan Tel:0321-9697141 3 Charsadda Quaidabad, Mardan Road, Charsadda Tel:0301-8908382 4 Mardan City Moh. Muslim Abad, Kas Korona, Mardan Tel:0345-9239479 5 Takht Bhai Mohallah Mira Khan. Malakand Road, Takht Bhai, Mardan Tel:0301-8767752 6 Hari Pur Sector #2, Kangra Colony, Hari Pur Tel:0300-5619286 7 Swabi Swatiano Mohallah, Topi Tel:0300-5653660 8 Kohat Happy Valley, KCB-1/93, Peshawar Road. Tel:0922-515472 9 Hangu House No. 1141, Mohallah Ganjiano Killi, Hangu Tel:0332-9643770 10 Abbottabad House No. 2719 M/C 2099, Link Road, Abbottabad. Tel:- 11 Mansehra Village Bhar Kand, Uggi Road, Tehsil & District Mansehra. Tel:0331-9284380 12 Tank Tank City, Tank Tel:0343-9296314 13 D.I.Khan Quaid-e-Azam Road, Banglow No. 1, Cantt. D.I. Khan Tel:0333-9954370 14 Bannu Hinjal, Bannu City Tel:0301-8085965 15 Pir Baba Near Pir Baba, Main Bazar, Buner Tel:0333-9690736 16 Swari Dewana baba road, Swari Buner Tel:0333-9690736 17 Swat St. No.1, Sharif Abad, Mingora, District Swat Tel:0344-9603081 18 Shangla Alpuri Village, Shanglapar Tel:0996-850813 19 Chitral Jung Bazar Payan, Near Polo Ground, Chitral Tel:0302-3161977 20 Mohmand Agency Chanda Bazar Ghalanai Tel:0346-9858682 21 Orakzai Agency Main Bazar Kalaya, Orakzai Agency Tel:0334-8287908 22 Bajaur Agency Near Old Hospital, Sabzi Mandi, Khar Tel:0303-8260940 23 Landi Kotal Main Landi Kotal Bazar, Khyber Agency Tel:0346-9720072 24 Jamrud Tidi, New Abadi, Jamrud, Khyber Agency Tel:0344-9846468 Province Punjab S# District Name Address of NCsRCL 1 Rawalpindi Bait-us-Sada Colony, Misrial Road, Rawalpindi Cantt Tel:0301-5867911 2 Dhoke Fateh, Kamal Pur Sayedan, near tube well District Attock Tel:0336-5778910 Attock Hassanabdal Mohallah Iqbnal Nagar Tehsil Hassan abdaal District Attock Tel:0322- 3 5715770/ 0322-5722019 H. -

Sindh: Public Expenditure Public Disclosure Authorized Review
Report No. Public Disclosure Authorized Public Disclosure Authorized PAKISTAN Sindh: Public Expenditure Public Disclosure Authorized Review SOUTH ASIAN REGION JUNE 2017 THE WORLD BANK GROUP Public Disclosure Authorized Sindh: Public Expenditure Review 2017 STANDARD DISCLAIMER This volume is a product of the staff of the International Bank for Reconstruction and Development/The World Bank. The findings, interpretations, and conclusions expressed in this paper do not necessarily reflect the views of the Executive Directors of The World Bank or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. COPYRIGHT STATEMENT The material in this publication is copyrighted. Copying and/or transmitting portions or all of this work without permission may be a violation of applicable law. The International Bank for Reconstruction and Development/The World Bank encourages dissemination of its work and will normally grant permission to reproduce portions of the work promptly. For permission to photocopy or reprint any part of this work, please send a request with complete information to the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, USA, telephone 978-750-8400, fax 978-750-4470, http://www.copyright.com/. All other queries -

Pakistan Red Crescent Society Sindh Provincial Branch
PAKISTAN RED CRESCENT SOCIETY SINDH PROVINCIAL BRANCH MONSOON 2011 Update th 8 September,04 -09 -2011 2011 Situation : Heavy rain falls in Sindh have been occurring since 9 th August, 2011. In response to the effects of flooding caused by these rains the PRCS has been providing relief assistance to the affectees since 14 th August, 2011. The recent spell of heavy rainfall that occurred during 29 th August and 3 rd September 2011 has resulted into flooding in some low-lying districts in Sindh Province. District Badin, Mirpurkhas, Dadu, Khairpur and Nawabshah are amongst the severely hit districts resulting in death of over 80 people and millions have been displaced. Various breaches in canals and drains connected with Left Bank Outfall Drain (LBOD) have left number of villages inundated. A large number of people, including women & children have been affected and huge losses to the crops, livestock, infrastructure, houses have been reported. It is estimated that at least 52 people were killed and dozens of others injured in three days of incessant rains in Sindh and parts of Balochistan and Punjab. The rains have also brought huge damage to properties, besides causing extensive destruction of standing crops. Interior Sindh is the most affe cted region where several villages were inundated and cut off from other areas. The relentless spell wiped out a big number of villages after breaches in canals and saline drains left them at the mercy of the rampaging waters. (Source Relief web - 03/09/2011 Media reports indicate that District Nawabshah (Benazirabad) has been declared as calamity hit due to widespread rains.