2021.06.30.21259439V1.Full.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Main Outcomes of Discussion of WHO Consultation on Nucleic Acid
MAIN OUTCOMES OF DISCUSSION FROM WHO CONSULTATION ON NUCLEIC ACID VACCINES I. Knezevic, R. Sheets 21-23 Feb, 2018 Geneva, Switzerland CONTEXT OF DISCUSSION • WHO Consultation held to determine whether the existing DNA guidelines were due for revision or if they remained relevant with today’s status of nucleic acid vaccine development and maturity towards licensure (marketing authorization) • Presentation will cover alignment to existing guidelines • Current status of development of DNA and RNA vaccines, both prophylactic & therapeutic • Main outcomes of discussion • Next steps already underway & planned STATUS OF DEVELOPMENT OF NUCLEIC ACID VACCINES • First likely candidate to licensure could be a therapeutic DNA vaccine against Human Papilloma Viruses • Anticipated to be submitted for licensure in 3-5 years • Other DNA vaccines are likely to follow shortly thereafter, e.g., Zika prophylaxis • RNA vaccines – less clinical experience, but therapeutic RNAs anticipated in 2021/22 timeframe to be submitted for licensure • For priority pathogens in context of public health emergencies, several candidates under development (e.g., MERS-CoV, Marburg, Ebola) MAIN OUTCOMES - GENERAL • Regulators expressed need for updated DNA guideline for prophylaxis and therapy • Less need at present for RNA vaccines in guideline but need some basic PTC • Flexibility needed now until more experience gained for RNA vaccines that will come in next few years • Revisit need for a more specific guideline at appropriate time for RNA vaccines • Institutional Biosafety Committees are regulated by national jurisdictions & vary considerably • How can WHO assist to streamline or converge these review processes? Particularly, during Public Health Emergency – can anything be done beforehand? MAIN OUTCOMES - DEFINITIONS • Clear Definitions are needed • Proposed definition of DNA vaccine: • A DNA plasmid(s) into which the desired immunogen(s) is (are) encoded and prepared as purified plasmid preparations to be administered in vivo. -

Review of COVID-19 Vaccine Subtypes, Efficacy and Geographical Distributions Andre Ian Francis ,1 Saudah Ghany,1 Tia Gilkes,1 Srikanth Umakanthan2
Review Postgrad Med J: first published as 10.1136/postgradmedj-2021-140654 on 6 August 2021. Downloaded from Review of COVID-19 vaccine subtypes, efficacy and geographical distributions Andre Ian Francis ,1 Saudah Ghany,1 Tia Gilkes,1 Srikanth Umakanthan2 1Department of Clinical Medical ABSTRACT 2021, the Ad26.COV2.S, developed by Janssen Sciences, The Faculty of Medical As of 1 May 2021, there have been 152 661 445 (Johnson & Johnson) and Moderna on 30 April.4 Sciences, The University of the COVAX, coordinated by WHO, Gavi: The West Indies, St. Augustine, Covid-19 cases with 3 202 256 deaths globally. Trinidad and Tobago This pandemic led to the race to discover a vaccine Vaccine Alliance, the Coalition for Epidemic 2Pathology unit, Department to achieve herd immunity and curtail the damaging Preparedness Innovations (CEPI), acts as a of Paraclinical Sciences, The effects of Covid-19. This study aims to discuss the most programme that supports the development of University Of The West Indies, St. COVID-19 vaccine candidates and negotiates their Augustine, Trinidad and Tobago recent WHO-approved Covid-19 vaccine subtypes, their status and geographical scheduled updates as of 4 pricing to ensure low- and- middle- income countries have a fair shot at receiving vaccines.5 Correspondence to May 2021. The keywords “Covid-19, Vaccines, Pfizer, Mr. Andre Ian Francis, The BNT162b2, AstraZeneca, AZD1222, Moderna, mRNA- This article aims at discussing the most recent University of the West Indies, St. 1273, Janssen, Ad26.COV2.S” were typed into PubMed. WHO- approved COVID-19 vaccine subtypes, their Augustine, Trinidad and Tobago; Thirty Two relevant PubMed articles were included in status and geographical scheduled updates as of 4 andre. -

V.5 3/18/2021 1 COVID-19 Vaccine FAQ Sheet
COVID-19 Vaccine FAQ Sheet (updated 3/18/2021) The AST has received queries from transplant professionals and the community regarding the COVID-19 vaccine. The following FAQ was developed to relay information on the current state of knowledge. This document is subject to change and will be updated frequently as new information or data becomes available. What kinds of vaccines are available or under development to prevent COVID-19? There are currently several vaccine candidates in use or under development. In the United States, the Government is supporting six separate vaccine candidates. Several other vaccines are also undergoing development outside of the United States government sponsorship and further information can be found here: NYTimes Coronavirus Vaccine Tracker: https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine- tracker.html Washington Post Vaccine Tracker: https://www.washingtonpost.com/graphics/2020/health/covid-vaccine-update- coronavirus/ v.5 3/18/2021 1 The types of vaccines are as follows (March 1, 2021) 1: Table 1: Vaccines Under Development or Available Through EUA Vaccine Type Compound Name [Sponsor] Clinical Notes Trial Phase mRNA mRNA-1273 [Moderna] Phase 3 Emergency use in U.S., E.U., other countries Approved in Canada BNT162b2 (Comirnaty) [Pfizer] Phase 2/3 Emergency use in U.S., E.U., other countries Also approved in Canada and other countries Replication- AZD1222 (Covishield) Phase 2/3 Emergency use defective [AstraZeneca] in U.K., India, adenoviral other countries vector (not U.S.) JNJ-78326735/Ad26.COV2.S -

An Update on Self-Amplifying Mrna Vaccine Development
Review An Update on Self-Amplifying mRNA Vaccine Development Anna K. Blakney 1,* , Shell Ip 2 and Andrew J. Geall 2 1 Michael Smith Laboratories, School of Biomedical Engineering, University of British Columbia, Vancouver, BC V6T 1Z4, Canada 2 Precision NanoSystems Inc., Vancouver, BC V6P 6T7, Canada; [email protected] (S.I.); [email protected] (A.J.G.) * Correspondence: [email protected] Abstract: This review will explore the four major pillars required for design and development of an saRNA vaccine: Antigen design, vector design, non-viral delivery systems, and manufacturing (both saRNA and lipid nanoparticles (LNP)). We report on the major innovations, preclinical and clinical data reported in the last five years and will discuss future prospects. Keywords: RNA; self-amplifying RNA; replicon; vaccine; drug delivery 1. Introduction: The Four Pillars of saRNA Vaccines In December 2019, the SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) virus emerged, causing a respiratory illness, coronavirus disease 2019 (COVID-19), in Hubei province, China [1,2]. The virus has spread globally, with the World Health Organization (WHO) declaring it a Public Health Emergency of International concern on 30 January 2020 and a pandemic officially on 7 March 2020 [3]. There is a strong consensus globally that a COVID-19 vaccine is likely the most effective approach to sustainably controlling the COVID-19 pandemic [4]. There has been an unprecedented research effort and global Citation: Blakney, A.K.; Ip, S.; Geall, coordination which has resulted in the rapid development of vaccine candidates and A.J. An Update on Self-Amplifying initiation of human clinical trials. -

1 Title: Interim Report of a Phase 2 Randomized Trial of a Plant
medRxiv preprint doi: https://doi.org/10.1101/2021.05.14.21257248; this version posted May 17, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. 1 Title: Interim Report of a Phase 2 Randomized Trial of a Plant-Produced Virus-Like Particle 2 Vaccine for Covid-19 in Healthy Adults Aged 18-64 and Older Adults Aged 65 and Older 3 Authors: Philipe Gobeil1, Stéphane Pillet1, Annie Séguin1, Iohann Boulay1, Asif Mahmood1, 4 Donald C Vinh 2, Nathalie Charland1, Philippe Boutet3, François Roman3, Robbert Van Der 5 Most4, Maria de los Angeles Ceregido Perez3, Brian J Ward1,2†, Nathalie Landry1† 6 Affiliations: 1 Medicago Inc., 1020 route de l’Église office 600, Québec, QC, Canada, G1V 7 3V9; 2 Research Institute of the McGill University Health Centre, 1001 Decarie St, Montreal, 8 QC H4A 3J1; 3 GlaxoSmithKline Biologicals SA (Vaccines), Avenue Fleming 20, 1300 Wavre, 9 Belgium; 4 GlaxoSmithKline Biologicals SA (Vaccines), rue de l’Institut 89, 1330 Rixensart, 10 Belgium; † These individuals are equally credited as senior authors. 11 * Corresponding author: Nathalie Landry, 1020 Route de l’Église, Bureau 600, Québec, Qc, 12 Canada, G1V 3V9; Tel. 418 658 9393; Fax. 418 658 6699; [email protected] 13 Abstract 14 The rapid spread of SARS-CoV-2 globally continues to impact humanity on a global scale with 15 rising morbidity and mortality. Despite the development of multiple effective vaccines, new 16 vaccines continue to be required to supply ongoing demand. -

Revision Rápida
REVISION RÁPIDA EVALUACIÓN DE LAS CARACTERÍSTICAS DE ALMACENAMIENTO, TRANSPORTE Y DISTRIBUCIÓN DE LAS VACUNAS COVID-19 EN ESTUDIO, Y LAS CARACTERÍSTICAS CLÍNICAS DE LA POBLACIÓN CANDIDATA A VACUNACIÓN Noviembre de 2020 El Instituto de Evaluación Tecnológica en Salud – IETS, es una corporación sin ánimo de lucro, de participación mixta y de carácter privado, con patrimonio propio, creado según lo estipulado en la Ley 1438 de 2011. Su misión es contribuir al desarrollo de mejores políticas públicas y prácticas asistenciales en salud, mediante la producción de información basada en evidencia, a través de la evaluación de tecnologías en salud y guías de práctica clínica, con rigor técnico, independencia y participación. Sus miembros son el Ministerio de Salud y Protección Social – MinSalud, el Departamento Administrativo de Ciencia, Tecnología e Innovación – Colciencias, el Instituto Nacional de Vigilancia de Medicamentos y Alimentos – INVIMA, el Instituto Nacional de Salud – INS, la Asociación Colombiana de Facultades de Medicina – ASCOFAME y la Asociación Colombiana de Sociedades Científicas – ACSC. Autores Lucas López Quiceno. Médico y cirujano, Especialista en Epidemiología, Magister en Epidemiología, Magíster en economía de la salud (c). Instituto de Evaluación Tecnológica en Salud - IETS. Jhyld Carolaind Camacho Barbosa, Nutricionista y Dietista, Magister en Epidemiología. Instituto de Evaluación Tecnológica en Salud - IETS. Kelly Estrada-Orozco. Médica, Magister en Epidemiología Clínica, Magister en Neurociencia. Doctorado en Salud Pública (actual). Doctorado en Epidemiología Clínica (actual). Instituto de Evaluación Tecnológica en Salud - IETS. Revisores Cortes-Muñoz, Ani Julieth. Bacterióloga y laboratorista clínica. MSc. Epidemiología. Instituto de Evaluación Tecnológica en salud - IETS. Ospina-Lizarazo, Nathalie. Nutricionista Dietista. MSc. Epidemiología Clínica. Instituto de Evaluación Tecnológica en salud - IETS. -

Covid-19 Messenger Rna Vaccine
COVID-19 MESSENGER RNA VACCINE A Piece of the Coronavirus The SARS-CoV-2 virus is studded with proteins that it uses to enter human cells. These so-called spike proteins make a tempting target for potential vaccines and treatments. Image of Coronavirus and spike proteins. Spike CORONAVIRUS protein Spikes gene Like the Pfizer vaccine, Moderna’s vaccine is based on the virus’s genetic instructions for building the spike protein. mRNA Inside an Oily Shell The vaccine uses messenger RNA, genetic material that our cells read to make proteins. The molecule — called mRNA for short — is fragile and would be chopped to pieces by our natural enzymes if it were injected directly into the body. To protect their vaccine, Pfizer and BioNTech wrap mRNA in oily bubbles made of lipid nanoparticles. Lipid nanoparticles surrounding mRNA Entering a Cell After injection, the vaccine particles bump into cells and fuse to them, releasing mRNA. The cell’s molecules read its sequence and build spike proteins. The mRNA from the vaccine is eventually destroyed by the cell, leaving no permanent trace. Vaccine Particle Translating mRNA fuses into Spike Spike Protien, which beaks it into Protein fragmentsmRNA and then destroyed by the Translatingcell nucleus. mRNA Spike Three spike Proteins Combine Cell Nucleus Spike Proteins and Fragments Protruding Displaying Protein Fragments Spikes Some of the spike proteins form spikes that migrate to the surface of the cell and stick out their tips. The vaccinated cells also break up some of the proteins into fragments, which they present on their surface. These protruding spikes and spike protein fragments can then be recognized by the immune system. -
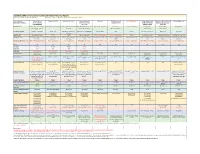
Candidate SARS-Cov-2 Vaccines in Advanced Clinical Trials: Key Aspects Compiled by John D
Candidate SARS-CoV-2 Vaccines in Advanced Clinical Trials: Key Aspects Compiled by John D. Grabenstein, RPh, PhD All dates are estimates. All Days are based on first vaccination at Day 0. Vaccine Sponsor Univ. of Oxford ModernaTX USA BioNTech with Pfizer Johnson & Johnson Novavax Sanofi Pasteur with CureVac with Bayer CanSino Biologics with Sinopharm (China National Sinovac Biotech Co. [with Major Partners] (Jenner Institute) (Janssen Vaccines & GlaxoSmithKline Academy of Military Biotec Group) (Beijing IBP, with AstraZeneca Prevention) Medical Sciences Wuhan IBP) Headquarters Oxford, England; Cambridge, Cambridge, Massachusetts Mainz, Germany; New York, New Brunswick, New Jersey Gaithersburg, Maryland Lyon, France; Tübingen, Germany Tianjin, China; Beijing, China; Beijing, China England, Gothenburg, New York (Leiden, Netherlands) Brentford, England Beijing, China Wuhan, China Sweden Product Designator ChAdOx1 or AZD1222 mRNA-1273 BNT162b2, tozinameran, Ad26.COV2.S, JNJ-78436735 NVX-CoV2373 TBA CVnCoV Ad5-nCoV, Convidecia BBIBP-CorV CoronaVac Comirnaty Vaccine Type Adenovirus 63 vector mRNA mRNA Adenovirus 26 vector Subunit (spike) protein Subunit (spike) protein mRNA Adenovirus 5 vector Inactivated whole virus Inactivated whole virus Product Features Chimpanzee adenovirus type Within lipid nanoparticle Within lipid nanoparticle Human adenovirus type 26 Adjuvanted with Matrix-M Adjuvanted with AS03 or Adjuvanted with AS03 Human adenovirus type 5 Adjuvanted with aluminum Adjuvanted with aluminum 63 vector dispersion dispersion vector AF03 -

Moderna COVID-19 Vaccine Factsheet
MODERNA COVID-19 V A C C I N E F A C T S H E E T Is it possible for the Moderna COVID-19 vaccine to give you COVID-19? This is not possible because the Moderna COVID-19 vaccine is a small portion of the COVID-19 RNA virus. Because it is not a complete virus it cannot cause a COVID-19 infection. The small portion of the RNA from the COVID-19 virus in the Moderna COVID-19 vaccine triggers an immune response in our body, and this reduces the risk of subsequent COVID-19 infection by 94%. This vaccine is a two-dose vaccine that is given 28 days apart. The vaccine will start protecting against COVID-19infection in as early as 14 days. Will the Moderna COVID-19 vaccine cause a positive COVID-19 PCR test? The Moderna COVID-19 vaccine can cause a COVID-19 antibody which signifies previous infection, however it will not cause a positive COVID-19 PCR test unless there is the rare (11 patients out of 14,000 patients) where the vaccine was not completely effective in preventing COVID-19 infection. How long will the Moderna COVID-19 vaccine protect against infection? This is not completely known as the vaccine has only been studied for 4 months. With the information we do know the vaccine has been shown to be 94% protective against COVID-19 infection for 4 months and there is no evidence of the vaccine losing effectiveness at this time. Can a patient with a previous COVID -19 infection be vaccinated with the Moderna COVID -19 vaccine? Yes. -

Vaccines: Self-Amplifying RNA in Lipid Nanoparticles
RESEARCH HIGHLIGHTS VACCINES Self-amplifying RNA in lipid nanoparticles: a next-generation vaccine? Photodisc Vaccines based on nucleic acids but are hampered by anti-vector Proof of concept was demonstrated (both DNA and RNA) have been immunity and safety concerns. in a model of respiratory syncytial investigated for several decades, The authors took advantage of virus (RSV) infection. The LNP–RNA but have not yet resulted in a recent advances in RNA synthesis vaccine potently induced neutralizing commercial product for human use. and nanoparticle technology. antibodies in cotton rats, as well Now, reporting in PNAS, Geall and Encapsulation of RNA in LNPs was as antigen-specific interferon- - colleagues present a new vaccine shown to protect it from enzymatic γ producing CD4+ and CD8+ T cells in platform based on self-amplifying degradation and allowed for efficient mice. These responses were comparable RNA encapsulated in synthetic lipid gene delivery after intramuscular to or exceeding those elicited by VRP nanoparticles (LNPs), which overcomes injection. Importantly, LNPs do not carry delivery of RNA or electroporation of some of the limitations of earlier vector surface proteins and are therefore pDNA and provided protection against nucleic-acid-based approaches. not limited by anti-vector immunity. subsequent RSV infection. The concept of nucleic-acid-encoded The self-amplifying RNA was derived This approach The authors point out that the vaccines was conceived over two from the genome of an alphavirus; the could provide LNP–RNA vaccine is produced in vitro in decades ago when it was found that genes encoding structural proteins were a potentially a cell-free manner, allowing large-scale, injection of mRNA or plasmid DNA replaced by genes coding for the antigen generic platform cost-effective production while (pDNA) into skeletal muscle of mice of interest, whereas the RNA replication for the rapid avoiding safety and manufacturing leads to the expression of the encoded machinery was retained. -

Comirnaty, INN-COVID-19 Mrna Vaccine (Nucleoside-Modified)
19 February 2021 EMA/707383/2020 Corr.1*1 Committee for Medicinal Products for Human Use (CHMP) Assessment report Comirnaty Common name: COVID-19 mRNA vaccine (nucleoside-modified) Procedure No. EMEA/H/C/005735/0000 Note Assessment report as adopted by the CHMP with all information of a commercially confidential nature deleted. 1 * Correction dated 19 February 2021 to clarify ERA statement Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us An agency of the European Union Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 © European Medicines Agency, 2021. Reproduction is authorised provided the source is acknowledged. Table of contents 1. Background information on the procedure .............................................. 8 1.1. Submission of the dossier ...................................................................................... 8 1.2. Steps taken for the assessment of the product ......................................................... 9 2. Scientific discussion .............................................................................. 11 2.1. Problem statement ............................................................................................. 11 2.1.1. Disease or condition ......................................................................................... 11 2.1.2. Epidemiology and risk factors ........................................................................... -

Pfizer-Biontech COVID-19 Vaccine Bnt162b2
DRAFT Prepared by the SAGE Working Group on COVID-19 Vaccines 22 December 2020 mRNA vaccines against COVID-19: Pfizer-BioNTech COVID-19 vaccine BNT162b2 Prepared by the Strategic Advisory Group of Experts (SAGE) on Immunization Working Group on COVID-19 vaccines 22 December 2020 © World Health Organization 2020. All rights reserved. This is a draft. The content of this document is not final, and the text may be subject to revisions before publication. The document may not be reviewed, abstracted, quoted, reproduced, transmitted, distributed, translated or adapted, in part or in whole, in any form or by any means without the permission of the World Health Organization. WHO reference number: WHO/2019-nCoV/vaccines/SAGE_evaluation/BNT162b2/2020.1 1 Background document for the Extraordinary meeting of the Strategic Advisory Group of Experts on Immunization (SAGE) - 5 January 2021 DRAFT Prepared by the SAGE Working Group on COVID-19 Vaccines 22 December 2020 Contents: General considerations on mRNA vaccines ............................................................................................................ 3 COVID-19 vaccine BNT162b2 (Pfizer-BioNTech) vaccine characteristics ................................................................ 3 Development process, contents, formulation ........................................................................................................ 3 Pre-clinical Studies .................................................................................................................................................