1 Altitude Training and Its Effects on the Human Body By: Haley Vissers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Fog and Low Clouds As Troublemakers During Wildfi Res
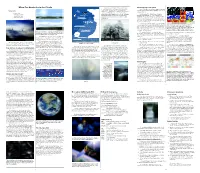
When Our Heads Are in the Clouds Sometimes water droplets do not freeze in below- Detecting fog from space Up to 60,000 ft (18,000m) freezing temperatures. This happens if they do not have Weather satellites operated by the National Oceanic The fog comes a surface (like a dust particle or an ice crystal) upon and Atmospheric Administration (NOAA) collect data on on little cat feet. which to freeze. This below-freezing liquid water becomes clouds and storms. Cirrus Commercial Jetliner “supercooled.” Then when it touches a surface whose It sits looking (36,000 ft / 11,000m) temperature is below freezing, such as a road or sidewalk, NOAA operates two different types of satellites. over harbor and city Geostationary satellites orbit at about 22,236 miles Breitling Orbiter 3 the water will freeze instantly, making a super-slick icy on silent haunches (34,000 ft / 10,400m) Cirrocumulus coating on whatever it touches. This condition is called (35,786 kilometers) above sea level at the equator. At this and then moves on. Mount Everest (29,035 ft / 8,850m) freezing fog. altitude, the satellite makes one Earth orbit per day, just Carl Sandburg Cirrostratus as Earth rotates once per day. Thus, the satellite seems to 20,000 feet (6,000 m) Cumulonimbus hover over one spot below and keeps its “birds’-eye view” of nearly half the Earth at once. Altocumulus The other type of NOAA satellites are polar satellites. Their orbits pass over, or nearly over, the North and South Clear and cloudy regions over the U.S. -

Altitude Training Relevance and Limits
SPORTS SCIENCE IMPROVING ENDURANCE PERFORMANCE WITH ‘LIVE HIGH - TRAIN LOW’ ALTITUDE TRAINING RELEVANCE AND LIMITS – Written by Paul Robach, France and Carsten Lundby, Switzerland Historically, altitude training has been aerobic performance in humans. This failure sport federations to build a substantial defined as the practice adopted by athletes prompted athletes and coaches to implement number of hypoxic facilities worldwide. who train for several weeks in an oxygen- altitude training camps with the objective After several decades and the involvement deprived environment (altitude training to acclimatise to competition at altitude. It of a large number of elite athletes who camp) in order to improve their endurance soon became apparent, however, that alti- sometimes set new world records after performance. By extension, altitude training tude training also could improve endurance returning from altitude, the key question refers to the use of natural or simulated performance upon return to sea level. The arises: does it really work? Unfortunately, altitude conditions during the course of rationale was that on the one hand, total red to date the majority of well-controlled the training process, at rest and/or during blood cell volume is a key factor for endurance scientific studies fail to demonstrate a exercise. Whatever the altitude training performance, as highlighted by experiments systematic positive effect of altitude training strategy, athletes exposed to altitude are incorporating blood manipulations. The on endurance performance in athletes. facing low-oxygen pressure (hypoxia), larger number of red blood cells an athlete Nonetheless, a common observation resulting in a lower blood and tissue has, the faster he will probably be able to is that some athletes do benefit from this oxygenation (hypoxemia). -

Aviation Glossary
AVIATION GLOSSARY 100-hour inspection – A complete inspection of an aircraft operated for hire required after every 100 hours of operation. It is identical to an annual inspection but may be performed by any certified Airframe and Powerplant mechanic. Absolute altitude – The vertical distance of an aircraft above the terrain. AD - See Airworthiness Directive. ADC – See Air Data Computer. ADF - See Automatic Direction Finder. Adverse yaw - A flight condition in which the nose of an aircraft tends to turn away from the intended direction of turn. Aeronautical Information Manual (AIM) – A primary FAA publication whose purpose is to instruct airmen about operating in the National Airspace System of the U.S. A/FD – See Airport/Facility Directory. AHRS – See Attitude Heading Reference System. Ailerons – A primary flight control surface mounted on the trailing edge of an airplane wing, near the tip. AIM – See Aeronautical Information Manual. Air data computer (ADC) – The system that receives and processes pitot pressure, static pressure, and temperature to present precise information in the cockpit such as altitude, indicated airspeed, true airspeed, vertical speed, wind direction and velocity, and air temperature. Airfoil – Any surface designed to obtain a useful reaction, or lift, from air passing over it. Airmen’s Meteorological Information (AIRMET) - Issued to advise pilots of significant weather, but describes conditions with lower intensities than SIGMETs. AIRMET – See Airmen’s Meteorological Information. Airport/Facility Directory (A/FD) – An FAA publication containing information on all airports, seaplane bases and heliports open to the public as well as communications data, navigational facilities and some procedures and special notices. -

Solar Energy Generation Model for High Altitude Long Endurance Platforms
Solar Energy Generation Model for High Altitude Long Endurance Platforms Mathilde Brizon∗ KTH - Royal Institute of Technology, Stockholm, Sweden For designing and evaluating new concepts for HALE platforms, the energy provided by solar cells is a key factor. The purpose of this thesis is to model the electrical power which can be harnessed by such a platform along any flight trajectory for different aircraft designs. At first, a model of the solar irradiance received at high altitude will be performed using the solar irradiance models already existing for ground level applications as a basis. A calculation of the efficiency of the energy generation will be performed taking into account each solar panel's position as well as shadows casted by the aircraft's structure. The evaluated set of trajectories allows a stationary positioning of a hale platform with varying wind conditions, time of day and latitude for an exemplary aircraft configuration. The qualitative effects of specific parameter changes on the harnessed solar energy is discussed as well as the fidelity of the energy generation model results. Nomenclature δ Solar declination ({) EQE Quantum efficiency (%) η Efficiency (%) hg Altitude of the aircraft (m) ◦ Γ Day angle ( ) hO3 Height of max ozone concentration(m) ◦ −2 −1 λg Longitude aircraft ( ) Id Direct irradiance (W:m .µm ) ◦ −2 −1 ! Hour angle ( ) Is Diffuse irradiance (W:m .µm ) ◦ −2 −1 φg Latitude of the aircraft ( ) Itot Total irradiance (W:m .µm ) ◦ −1 ◦ τ Rayleigh optical depth ({) kPmax;T Temperature Coefficient (%: C ) 2 A Solar cell -

1 the Atmosphere of Pluto As Observed by New Horizons G
The Atmosphere of Pluto as Observed by New Horizons G. Randall Gladstone,1,2* S. Alan Stern,3 Kimberly Ennico,4 Catherine B. Olkin,3 Harold A. Weaver,5 Leslie A. Young,3 Michael E. Summers,6 Darrell F. Strobel,7 David P. Hinson,8 Joshua A. Kammer,3 Alex H. Parker,3 Andrew J. Steffl,3 Ivan R. Linscott,9 Joel Wm. Parker,3 Andrew F. Cheng,5 David C. Slater,1† Maarten H. Versteeg,1 Thomas K. Greathouse,1 Kurt D. Retherford,1,2 Henry Throop,7 Nathaniel J. Cunningham,10 William W. Woods,9 Kelsi N. Singer,3 Constantine C. C. Tsang,3 Rebecca Schindhelm,3 Carey M. Lisse,5 Michael L. Wong,11 Yuk L. Yung,11 Xun Zhu,5 Werner Curdt,12 Panayotis Lavvas,13 Eliot F. Young,3 G. Leonard Tyler,9 and the New Horizons Science Team 1Southwest Research Institute, San Antonio, TX 78238, USA 2University of Texas at San Antonio, San Antonio, TX 78249, USA 3Southwest Research Institute, Boulder, CO 80302, USA 4National Aeronautics and Space Administration, Ames Research Center, Space Science Division, Moffett Field, CA 94035, USA 5The Johns Hopkins University Applied Physics Laboratory, Laurel, MD 20723, USA 6George Mason University, Fairfax, VA 22030, USA 7The Johns Hopkins University, Baltimore, MD 21218, USA 8Search for Extraterrestrial Intelligence Institute, Mountain View, CA 94043, USA 9Stanford University, Stanford, CA 94305, USA 10Nebraska Wesleyan University, Lincoln, NE 68504 11California Institute of Technology, Pasadena, CA 91125, USA 12Max-Planck-Institut für Sonnensystemforschung, 37191 Katlenburg-Lindau, Germany 13Groupe de Spectroscopie Moléculaire et Atmosphérique, Université Reims Champagne-Ardenne, 51687 Reims, France *To whom correspondence should be addressed. -

Physical Activity at Moderate and High Altitudes. Cardiovascular and Respiratory Morbidit
Arq Bras Cardiol CamposUpdate & Costa volume 73, (nº 1), 1999 Physical activity at high altitudes Physical Activity at Moderate and High Altitudes. Cardiovascular and Respiratory Morbidit Augusta L. Campos, Ricardo Vivacqua C. Costa Rio de Janeiro, RJ - Brazil In recent decades, sports activities related to nature observed an increase of 5 to 10mmHg in the SBP and a re- have become increasingly popular. As more and more duction of 5mmHg in diastolic BP in 6 individuals during people look for ski resorts in mountainous regions or beco- exercise on a bicycle at a simulated altitude of 4,200m, when me involved with activities such as walking and/or moun- compared with that found at sea level. Malconian et al 11 tain climbing at moderate and high altitudes, diseases found a 10% reduction in the mean BP at maximal effort, in a related to this environmental stress become problems that simulated altitude of 8,848m, corresponding to the summit doctors have to face with an increasing frequency; they of Mount Everest, compared with the values found at sea need, therefore, to know these entities better. In addition, level. D’Este et al 12 performed a submaximal test on 10 nor- many athletic competitions are performed at altitudes above motensive individuals after acute exposure to 2,500m and 2,000 m, such as the Olympic Games of 1968 and the World did not find significant differences in the pressure response Cup Soccer Games of 1970, which took place in Mexico City, compared with the results of the test at sea level. Palatini et Mexico, at 2,240 m. -

Altitude Sickness Fact Sheet
Altitude Sickness Fact Sheet At high elevation, you may experience a potentially life threatening condition called altitude sickness. This is exacerbated if you ascend in elevation quickly. At 8,000 feet, there is only ~75% of the available oxygen at sea level. Oxygen decreases ~3% with each 1000 feet in elevation. Altitude sickness is caused by the body not being able to get enough oxygen. There are three types of altitude sickness: Acute Mountain Sickness, High Altitude Pulmonary Edema, and High Altitude Cerebral Edema. SYMPTOMS Acute Mountain Sickness • Lack of appetite, nausea, or vomiting • Fatigue • Dizziness • Insomnia • Shortness of breath upon exertion • Nosebleed • Persistent rapid pulse • Swelling of hands, feet, and/or face High Altitude Pulmonary Edema (HAPE) • Symptoms similar to bronchitis • Persistent dry cough • Fever • Shortness of breath even at rest High Altitude Cerebral Edema (HACE) • Headache that does not respond to medication • Difficulty walking • Altered mental state (confusion, changes in alertness, disorientation, irrational behavior) • Loss of consciousness • Increased nausea • Blurred vision or retinal hemorrhage PREVENTION If your hike starts at high elevation, spend a few days adjusting to the altitude prior to any major physical exertion. It is best to sleep no more than 1,500 feet (457.2 m) higher than you did the night before. This helps the body adjust gradually to the decreased amount of oxygen. Contact your primary care physician for an evaluation prior to travelling to areas with high elevation. FIRST AID TREATMENT If you have any of these symptoms at altitude, assume that it is altitude sickness until proven otherwise. Do not ascend any further with symptoms. -

Altitude Profiles of CCN Characteristics Across the Indo-Gangetic Plain Prior to the Onset of the Indian Summer Monsoon
5 Altitude profiles of CCN characteristics across the Indo-Gangetic Plain prior to the onset of the Indian summer monsoon Venugopalan Nair Jayachandran1, Surendran Nair Suresh Babu1*, Aditya Vaishya2, Mukunda M. Gogoi1, Vijayakumar S Nair1, Sreedharan Krishnakumari Satheesh3,4, Krishnaswamy Krishna Moorthy3 10 1 Space Physics Laboratory, Vikram Sarabhai Space Centre, ISRO PO, Thiruvananthapuram, India. 2 School of Arts and Sciences, Ahmedabad University, Ahmedabad, India. 3 Centre for Atmospheric and Oceanic Sciences, Indian Institute of Science, Bangalore, India. 4 Divecha Centre for Climate Change, Indian Institute of Science, Bangalore, India. 15 *Correspondence to: Surendran Nair Suresh Babu ([email protected] / [email protected]) 1 5 Abstract Concurrent measurements of the altitude profiles of cloud condensation nuclei (CCN) concentration, as a function of supersaturation (ranging from 0.2% to 1.0%), and aerosol optical properties (scattering and absorption coefficients) were carried out aboard an instrumented aircraft across the Indo-Gangetic Plain (IGP) just prior to the onset of the Indian summer monsoon (ISM) 10 of 2016. The experiment was conducted under the aegis of the SWAAMI - RAWEX campaign. The measurements covered coastal, urban and arid environments. In general, the CCN concentration has been highest in the Central IGP, decreasing spatially from east to west above the planetary boundary layer (PBL), which is ~1.5 km for the IGP during pre-monsoon. Despite this, the CCN activation efficiency at 0.4% supersaturation has been, interestingly, the highest over the 15 eastern IGP (~72%), followed by that in the west (~61%), and has been the least over the central IGP (~24%) within the PBL. -

Journal of Space Law Volume 41 Number 2 2017
Journal of Space Law Volume 41 Number 2 2017 In Memoriam: George S. Robinson Articles The Non Kármán Line: An Urban Legend of the Space Age .............................Thomas Gangale Incentives for Keeping Space Clean: Orbital Debris and Mitigation Waivers.....................................................................Stephen J. Garber The Intersection of U.S Space Policy Goals and National Security Needs: An Argument for a Regulatory Regime Oversight Commission That Balances Space Related Policy Interests....................................................................................Rebekah Rounds Student Article Stakeout from Space: Fourth Amendment Concerns Resulting from the Onset of Satellite Video.............................................Blake Knight Translation 1865 International Telegraph Convention with Translator’s Introduction...........Harrison Parker Bibliography Space Law Bibliography...........................................................................................Kyle Hansen 51 to 315 41 2 1 7 Vol. , No. Journal of Space Law Pages 201 JOURNAL OF SPACE LAW VOLUME 41, NUMBER 2 2017 JOURNAL OF SPACE LAW UNIVERSITY OF MISSISSIPPI SCHOOL OF LAW A JOURNAL DEVOTED TO SPACE LAW AND THE LEGAL PROBLEMS ARISING OUT OF HUMAN ACTIVITIES IN OUTER SPACE. VOLUME 41 2017 NUMBER 2 Editor-in-Chief P.J. Blount, J.D., LL.M., Ph.D. Executive Editor Andrea Harrington, J.D., LL.M., D.C.L. Senior Student Editors Student Editors Nathaniel Celeski Alexis Danielle Banks Haley Grantham Sammy Brown Kyle Hansen Brittney Eakins Blake -

Where Is Space? and Why Does That Matter?
Space Traffic Management Conference 2014 Roadmap to the Stars Nov 5th, 3:15 PM Where is Space? And Why Does That Matter? Bhavya Lal Science and Technology Policy Institute, [email protected] Emily Nightingale Science and Technology Policy Institute, [email protected] Follow this and additional works at: https://commons.erau.edu/stm Part of the Aerospace Engineering Commons, and the Science and Technology Policy Commons Lal, Bhavya and Nightingale, Emily, "Where is Space? And Why Does That Matter?" (2014). Space Traffic Management Conference. 16. https://commons.erau.edu/stm/2014/wednesday/16 This Event is brought to you for free and open access by the Conferences at Scholarly Commons. It has been accepted for inclusion in Space Traffic Management Conference by an authorized administrator of Scholarly Commons. For more information, please contact [email protected]. Where is Space? And Why Does That Matter? Bhavya Lal, Ph.D. Research Staff Member Emily Nightingale, Science Policy Fellow Science and Technology Policy Institute, 1899 Pennsylvania Avenue NW, Washington DC 20006 Abstract Despite decades of debate on the topic, there is no consensus on what, precisely, constitutes the boundary between airspace and outer space. The topic is mired in legal and political conundrums, and the easy solution to-date has been to not agree on a definition of space. Lack of a definition, some experts claim, has not limited space-based activities, and therefore is not a hurdle that must be overcome. There are increasing calls however in light of increasing (and expectations of increasing) space traffic, both orbital and sub- orbital. This paper summarizes the proposed delimitation of space, the current debate on whether or not the boundary should be defined and internationally accepted, and our assessment on the need to define it based on emerging space traffic management needs. -

Inflammation, Peripheral Signals and Redox Homeostasis in Athletes Who Practice Different Sports
antioxidants Review Inflammation, Peripheral Signals and Redox Homeostasis in Athletes Who Practice Different Sports Simone Luti 1 , Alessandra Modesti 1,* and Pietro A. Modesti 2 1 Department of Biomedical, Experimental and Clinical Sciences “Mario Serio”, University of Florence, 50134 Florence, Italy; simone.luti@unifi.it 2 Department of Experimental and Clinical Medicine, University of Florence, 50134 Florence, Italy; pamodesti@unifi.it * Correspondence: alessandra.modesti@unifi.it; Tel.: +39-055-2751237 Received: 17 September 2020; Accepted: 27 October 2020; Published: 30 October 2020 Abstract: The importance of training in regulating body mass and performance is well known. Physical training induces metabolic changes in the organism, leading to the activation of adaptive mechanisms aimed at establishing a new dynamic equilibrium. However, exercise can have both positive and negative effects on inflammatory and redox statuses. In recent years, attention has focused on the regulation of energy homeostasis and most studies have reported the involvement of peripheral signals in influencing energy and even inflammatory homeostasis due to overtraining syndrome. Among these, leptin, adiponectin, ghrelin, interleukin-6 (IL6), interleukin-1β (IL1β) and tumour necrosis factor a (TNFa) were reported to influence energy and even inflammatory homeostasis. However, most studies were performed on sedentary individuals undergoing an aerobic training program. Therefore, the purpose of this review was to focus on high-performance exercise studies performed in athletes to correlate peripheral mediators and key inflammation markers with physiological and pathological conditions in different sports such as basketball, soccer, swimming and cycling. Keywords: cytokines; redox homeostasis; sport performance 1. Introduction In elite athletes, there is large disparity among the training protocols; the effects on oxidative stress (OS) and inflammatory cytokines are still not well known. -

PHAK Chapter 12 Weather Theory
Chapter 12 Weather Theory Introduction Weather is an important factor that influences aircraft performance and flying safety. It is the state of the atmosphere at a given time and place with respect to variables, such as temperature (heat or cold), moisture (wetness or dryness), wind velocity (calm or storm), visibility (clearness or cloudiness), and barometric pressure (high or low). The term “weather” can also apply to adverse or destructive atmospheric conditions, such as high winds. This chapter explains basic weather theory and offers pilots background knowledge of weather principles. It is designed to help them gain a good understanding of how weather affects daily flying activities. Understanding the theories behind weather helps a pilot make sound weather decisions based on the reports and forecasts obtained from a Flight Service Station (FSS) weather specialist and other aviation weather services. Be it a local flight or a long cross-country flight, decisions based on weather can dramatically affect the safety of the flight. 12-1 Atmosphere The atmosphere is a blanket of air made up of a mixture of 1% gases that surrounds the Earth and reaches almost 350 miles from the surface of the Earth. This mixture is in constant motion. If the atmosphere were visible, it might look like 2211%% an ocean with swirls and eddies, rising and falling air, and Oxygen waves that travel for great distances. Life on Earth is supported by the atmosphere, solar energy, 77 and the planet’s magnetic fields. The atmosphere absorbs 88%% energy from the sun, recycles water and other chemicals, and Nitrogen works with the electrical and magnetic forces to provide a moderate climate.