A Study of the Impact of Eyelid Opening and Closing on The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pediatric Orbital Tumors and Lacrimal Drainage System
Pediatric Orbital Tumors and Lacrimal Drainage System Peter MacIntosh, MD University of Illinois • No financial disclosures Dermoid Cyst • Congenital • Keratinized epidermis • Dermal appendage • Trapped during embryogenesis • 6% of lesions • 40-50% of orbital pediatric orbital lesion • Usually discovered in the first year of life • Painless/firm/subQ mass • Rarely presents as an acute inflammatory lesion (Rupture?) • Frontozygomatic (70%) • Maxillofrontal (20%) suture Imaging - CT • Erosion/remodeling of bone • Adjacent bony changes: “smooth fossa” (85%) • Dumbell dermoid: extraorbital and intraorbital components through bony defect Imaging - MRI • Encapsulated • Enhancement of wall but not lumen Treatment Options • Observation • Risk of anesthesia • Surgical Removal • Changes to bone • Rupture of cyst can lead to acute inflammation • Irrigation • Abx • Steroids Dermoid INFANTILE/Capillary Hemangioma • Common BENIGN orbital lesion of children • F>M • Prematurity • Appears in 1st or 2nd week of life • Soft, bluish mass deep to the eyelid • Superonasal orbit • Rapidly expands over 6-12 months • Increases with valsalva (crying) • Clinical findings • Proptosis Astigmatism • Strabismus Amblyopia INFANTILE/Capillary Hemangioma • May enlarge for 1-2 years then regress • 70-80% resolve before age 7 • HIGH flow on doppler • Kasabach-Merritt Syndrome • Multiple large visceral capillary hemangiomas • Sequestration of platelets into tumor • Consumptive thrombocytopenia • Supportive therapy and treat underlying tumor • Complications • DIC • death •Homogenous -

Stage Surgery on Inverted Papilloma Which Invaded Lacrimal Sac, Periorbita, Ethmoid and Frontal Sinus
臨床耳鼻:第 27 卷 第 1 號 2016 ••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••• J Clinical Otolaryngol 2016;27:143-147 증 례 Stage Surgery on Inverted Papilloma which Invaded Lacrimal Sac, Periorbita, Ethmoid and Frontal Sinus Jae-hwan Jung, MD, Minsic Kim, MD, Sue Jean Mun, MD and Hwan-Jung Roh, MD, PhD Department of Otorhinolaryngology-Head & Neck Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea - ABSTRACT - Inverted papilloma of the nasal cavity and the paranasal sinuses is a benign epithelial tumor with a high rate of recurrence, local aggressiveness, and malignant transformation. For these reasons, inverted papilloma has been treated like malignant tumors with extensive surgical resection. With the help of endoscopic sinus surgery tech- nique, it is now available to treat inverted papilloma with stage surgery without severe complications which usu- ally resulted from extensive one stage resection. We report a case of stage surgery on inverted papilloma which invaded lacrimal sac, periorbita, ethmoid and frontal sinus. (J Clinical Otolaryngol 2016;27:143-147) KEY WORDS:Inverted papillomaㆍLacrimal sacㆍPeriorbitaㆍSurgery. Authors present a successful endoscopic stage sur- Introduction gery on IP which invaded lacrimal sac, periorbita, ethmoid and frontal sinus with the literature review. Inverted papilloma (IP) of the nasal cavity and the paranasal sinuses is a benign epithelial tumor with a Case Report high rate of recurrence, local aggressiveness, and ma- lignant transformation.1,2) For these reasons, IP has A 41-year-old female presented in outpatient clinic been treated like malignant tumors with extensive sur- with a complaint of tender swelling mass on the in- gical resection. ner side of her right eye for 5 years which suddenly IP of lacrimal sac and periorbita is rarely reported aggravated 2 months ago. -

New Theory on Facial Beauty: Ideal Dimensions in the Face and Its Application to Your Practice by Dr
New Theory on Facial Beauty: Ideal Dimensions in the Face And its application to your practice By Dr. Philip Young Aesthetic Facial Plastic Surgery 2015 Bellevue, Washington American Brazilian Aesthetic Meeting • Hello my presentation is on studying some further elements of a new theory on facial beauty called the Circles of Prominence. • Specifically we are going to be studying some key dimensions in the face that I think could possibly help your practice. • I’m from Bellevue Washington Home of Bill Gates, Microsoft and Starbucks. Beauty In my opinion Beauty is the most important trait that we have and it is the one trait that can have the most dramatic impact in our lives. Obviously finding the answer for Beauty is essential in our industry. The answers have alluded us: the magic number of Phi, cephalometrics, the neo classical canons by Leonardo Da Vinci, the averageness theory, etc. have all come short in finding what makes a face beautiful. • The Circles of Prominence is a theory that I discovered in 2003-2005 and was published in the Archives of Facial Plastic Surgery in 2006 and Received the Sir Harold Delf Gillies Award from the American Academy of Facial Plastic Surgery. The Circles of Prominence • Original published Archives FPS 2006 • Based on the idea that there is an ideal • Everything on the face has an ideal as well • Because we spend so much time looking at the iris • All dimensions of the face are related to the width of the iris • Obviously with a better definition of beauty our results in plastic surgery can be improved • The circles of prominence is based on the belief that there is an ideal. -

Anatomy of the Periorbital Region Review Article Anatomia Da Região Periorbital
RevSurgicalV5N3Inglês_RevistaSurgical&CosmeticDermatol 21/01/14 17:54 Página 245 245 Anatomy of the periorbital region Review article Anatomia da região periorbital Authors: Eliandre Costa Palermo1 ABSTRACT A careful study of the anatomy of the orbit is very important for dermatologists, even for those who do not perform major surgical procedures. This is due to the high complexity of the structures involved in the dermatological procedures performed in this region. A 1 Dermatologist Physician, Lato sensu post- detailed knowledge of facial anatomy is what differentiates a qualified professional— graduate diploma in Dermatologic Surgery from the Faculdade de Medician whether in performing minimally invasive procedures (such as botulinum toxin and der- do ABC - Santo André (SP), Brazil mal fillings) or in conducting excisions of skin lesions—thereby avoiding complications and ensuring the best results, both aesthetically and correctively. The present review article focuses on the anatomy of the orbit and palpebral region and on the important structures related to the execution of dermatological procedures. Keywords: eyelids; anatomy; skin. RESU MO Um estudo cuidadoso da anatomia da órbita é muito importante para os dermatologistas, mesmo para os que não realizam grandes procedimentos cirúrgicos, devido à elevada complexidade de estruturas envolvidas nos procedimentos dermatológicos realizados nesta região. O conhecimento detalhado da anatomia facial é o que diferencia o profissional qualificado, seja na realização de procedimentos mini- mamente invasivos, como toxina botulínica e preenchimentos, seja nas exéreses de lesões dermatoló- Correspondence: Dr. Eliandre Costa Palermo gicas, evitando complicações e assegurando os melhores resultados, tanto estéticos quanto corretivos. Av. São Gualter, 615 Trataremos neste artigo da revisão da anatomia da região órbito-palpebral e das estruturas importan- Cep: 05455 000 Alto de Pinheiros—São tes correlacionadas à realização dos procedimentos dermatológicos. -

TEAR PRODUCTION and DRAINAGE the Lacrimal Gland Is Located in the Superolateral Aspect of the Eyelid Below the Eyebrow(S)
Anatomy and Physiology 9 The conjunctiva is a mucous membrane that lines the upper and lower eyelids and extends over the sclera to the corneal margin. It contains lym- phoid tissue, which provides some immunology protection. It is innervated by CN V, the trigeminal nerve. The portion of the conjunctiva that covers the sclera is termed the bulbar conjunctiva; the portion covering the inner surface of the eyelids is termed the palpebral conjunctiva. Figure 1. Eyelid Muscles TEAR PRODUCTION AND DRAINAGE The lacrimal gland is located in the superolateral aspect of the eyelid below the eyebrow(s). It secretes watery (aqueous) tears and produces about 0.2 ml of tears in 24 hours. Aqueous tears flow downward and inward toward the tear drainage system at the inner canthus. In addition to aqueous tears, several glands located in the conjunctiva and eyelid margins secrete oily and sticky (mucous) tears. The meibomian glands are located within the tarsal plate of the eyelid and secrete oily tears. The glands of Zeiss, Moll, Wolfing, and Krause secrete sticky tears. These three types of tears provide moisture and protection to the surface of the eye(s). With each blink, tears are pushed across the eye toward the puncta located at the medial junction of the upper and lower eyelids. From the puncta, tears are pushed into the canaliculi and then into the lacrimal sac. 10 Essentials of Ophthalmic Nursing They are drained from the lacrimal sac and nasolacrimal duct to the inside of the nose and down the throat (see Figure 2). Figure 2. Lacrimal System TEAR FILM The tear film has three distinct layers. -

Lacrimal Sac Pseudotumour – a Case Report
Case Report JOJ Ophthal Volume 6 Issue 5 - September 2018 Copyright © All rights are reserved by Anushree Gupta DOI: 10.19080/JOJO.2018.07.555704 Lacrimal Sac Pseudotumour – A Case Report Anushree Gupta* Dr. Radhakrishnan Government Medical College, India Submission: September 04, 2018; Published: September 21, 2018 *Corresponding author: Anushree Gupta, M.B.B.S, D.N.B (Ophthalmology), Dr. Radhakrishnan Government Medical College, Hamirpur, Himachal Pradesh, India, Tel: ; Email: Abstract Lacrimal sac tumors are rare with a clinical presentation that typically mimics chronic dacryocystitis. A full history with clinical and diagnostic workup is essential to plan treatment. Herein we report the case of a 50-year-old woman with inflammatory pseudotumour of the lacrimalKeywords: sac Lacrimal confirmed sac by tumours; histopathological Epiphora; section.Dacryocystitis Abbrevations: CT: Computed Tomography; MPL: Medial Palpebral Ligament Introduction A patient presenting with chronic epiphora and mass in Her best corrected visual acuity was 20/20 in both the eyes. the medial canthal region can be due to many causes, most commonly being chronic dacryocystitis. It is usually associated There was a protrusion superior to medial canthus and a firm, (Figure 1). It was 3 cm x 2 cm in dimensions extending above nontender mass was palpable at the medial side of the left orbit mass typically below the medial canthal tendon. Persistent and below the medial canthal tendon. There was mild erythema with inflammatory signs, purulent discharge and a soft, fluctuant epiphora with an irreducible mass above the medial canthal and ancillary investigations are important to rule out malignancy overlying the swelling. There was no displacement of globe. -

Acquired Etiologies of Lacrimal System Obstructions
5 Acquired Etiologies of Lacrimal System Obstructions Daniel P. Schaefer Acquired obstructions of the lacrimal excretory outfl ow system will produce the symptoms of epiphora, mucopurulent discharge, pain, dacryocystitis, and even cellulitis, prompting the patient to seek the ophthalmologist for evaluation and treatment. Impaired tear outfl ow may be functional, structural, or both. The causes may be primary – those resulting from infl ammation of unknown causes that lead to occlusive fi brosis—or secondary, resulting from infections, infl amma- tion, trauma, malignancies, toxicity, or mechanical causes. Secondary acquired dacryostenosis and obstruction may result from many causes, both common and obscure. Occasionally, the precise pathogenesis of nasolacrimal duct obstruction will, despite years of investigations, be elusive. To properly evaluate and appropriately treat the patient, the ophthal- mologist must have knowledge and comprehension of the lacrimal anatomy, the lacrimal apparatus, pathophysiology, ocular and nasal relationships, ophthalmic and systemic disease process, as well as the topical and systemic medications that can affect the nasolacrimal duct system. One must be able to assess if the cause is secondary to outfl ow anomalies, hypersecretion or refl ex secretion, pseudoepiphora, eyelid malposition abnormalities, trichiasis, foreign bodies and conjunctival concretions, keratitis, tear fi lm defi ciencies or instability, dry eye syn- dromes, ocular surface abnormalities, irritation or tumors affecting the trigeminal nerve, allergy, medications, or environmental factors. Abnormalities of the lacrimal pump function can result from involu- tional changes, eyelid laxity, facial nerve paralysis, or fl oppy eyelid syndrome, all of which displace the punctum from the lacrimal lake. If the cause is secondary to obstruction of the nasolacrimal duct system, the ophthalmologist must be able to determine where the anomaly is and what the cause is, in order to provide the best treatment possible for the patient. -

The Lacrimal System Terms
The Lacrimal System Lynn E. Lawrence, CPOT, ABOC, COA, OSC Terms • Etiology – the cause of a disease or abnormal condition • Dacryocystitis – inflammation of the lacrimal sac • Epiphora – watering of eyes due to excess secretion of tears or obstruction of the lacrimal passage Tear Film Layers oil aqueous snot What functions does each layer of the tear perform? Lacrimal System: Tear Film Layers LIPID DEFICIENCY ‐ evaporates TEAR DEFICIENCY – fails to hydrate properly oil aqueous snot What functions does each layer of the tear perform? What are functions of tears? Tear Components • Lipid Layer – prevents evaporation • Aqueous Layer ‐ hydration • Mucus Layer – sticks tear to the eye • Other components Lacrimal Apparatus • Sometimes a person cannot produce natural tears they might need punctal plugs to prevent the tears from draining off the eye. • Faucet • Action • Drain Obstructive – vs‐ non‐obstructive Tear Production – Secretory • Lacrimal gland – Reflex tearing – Too much tearing…epiphora • Gland of Krause – Superior fornix • Gland of Wolfring – Superior tarsal plate Two Primary Forms of Dry Eye 800 nm 8,000 nm 100 nm The two primary forms of dry eye are Evaporative Dry Eye, also known as Meibomian Gland Dysfunction or MGD and Aqueous Dry Eye. The majority of dry eye sufferers have MGD. Oil & Water Remember science class? Oil floats. Oil does not mix with water, but rather sits on top of water. Oil is what keeps water from evaporating. Need three volunteers TEST TIME http://optometrytimes.modernmedicine.com/optometrytimes/news/treating‐dry‐eye‐ lipid‐based‐eye‐drops Lipid Secretion: Meibomian Glands Left: Transillumination of eyelid showing meibomian glands Right: Secretion of lipid at lid margin • The lipid layer restricts evaporation to 5‐10% of tear flow – Also helps lubricate Mucin Secretion: Goblet Cells Superficial layer of bulbar conjunctiva. -

Inferior Oblique Muscle of the Eye: Its Fetal Development with Special Reference to Understanding of the Frequent Variants in Adults
ONLINE FIRST This is a provisional PDF only. Copyedited and fully formatted version will be made available soon. ISSN: 0015-5659 e-ISSN: 1644-3284 Inferior oblique muscle of the eye: its fetal development with special reference to understanding of the frequent variants in adults Authors: Z. W. Jin, S. Umeki, Y. Takeuchi, M. Yamamoto, G. Murakami, S. Abe, J. F. Rodríguez-Vázquez DOI: 10.5603/FM.a2021.0043 Article type: Original article Submitted: 2021-03-13 Accepted: 2021-04-09 Published online: 2021-04-28 This article has been peer reviewed and published immediately upon acceptance. It is an open access article, which means that it can be downloaded, printed, and distributed freely, provided the work is properly cited. Articles in "Folia Morphologica" are listed in PubMed. Powered by TCPDF (www.tcpdf.org) Inferior oblique muscle of the eye: its fetal development with special reference to understanding of the frequent variants in adults Z.W. Jin et al., Development of the inferior obliquus Z.W. Jin1, S. Umeki2, Y. Takeuchi2, M. Yamamoto2, G. Murakami2, 3, S. Abe2, J.F. Rodríguez-Vázquez4 1Department of Anatomy, Wuxi School of Medicine, Jiangnan University, Wuxi, China 2Department of Anatomy, Tokyo Dental College, Tokyo, Japan 3Division of Internal Medicine, Cupid Clinic, Iwamizawa, Japan 4Department of Anatomy and Embryology, School of Medicine, Complutense University, Madrid, Spain Address for correspondence: Z.W. Jin, MD, PhD, Department of Anatomy, Wuxi School of Medicine, Jiangnan University, 1800 Lihu Avenue, Wuxi, Jiangsu, 214122, China, tel: +86-510-8519-7079, fax: +86-510-8519-3570, e-mail: [email protected] ABSTRACT To provide better understanding of frequent variations of the inferior oblique (IO) of adult extraocular muscles, we observed sagittal and horizontal histological sections of the eye and orbits from 32 fetuses (approximately 7-34 weeks of gestational age; 24-295 mm of crown-rump length). -
Abducens Nerve Lesion • Right LR Is Disabled
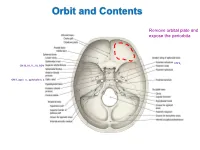
Orbit and Contents Remove orbital plate and expose the periorbita CN V2 CN III, IV, V1, VI, SOV CN II, optic n., ophthalmic a. Orbit and Contents Contents of orbit: • Eyeball and extraocular mm • Nerves to mm and orbital contents • Optic nerve (CN II) – retina; vision • Ciliary ganglion – PS supply to sphincter pupillae and ciliary mm • Ophthalmic artery and veins • Lacrimal gland and ducts • Lacrimal sac and canaliculi • FAT!! Bony Orbit and Walls The orbit is a 4-sided pyramid: Base (orbital margin) – anterolaterally • Frontal, Maxilla, Zygomatic bones Apex - posteromedially Walls: Roof – frontal bone Lateral – zygomatic, greater wing of sphenoid Medial – lesser wing of sphenoid, ethmoid (lamina papyracea), lacrimal, part of maxilla Floor – maxilla (“roof of maxillary sinus”) Three of the four sides are bounded by paranasal sinuses: Superiorly – Frontal sinus (behind eyebrows) Medially – Ethmoidal sinuses (air cells) Inferiorly – Maxillary sinus Bones are thin and vulnerable to “blowout” fractures Bony Orbit and Openings Orbital and Optical Axes and Position of Eyeball in Orbit = visual axis Axes about which movements of the eyeball occur 1. Vertical axis (superior/inferior poles) – rotation of pupil toward nose (=adduction) – rotation of pupil away from nose (=abduction) 2. Transverse axis (mediolateral; at equator) – rotate pupil upward (=elevation) – rotate pupil downward (=depression) 3. Anterior-posterior axis (optical axis, line of sight) – rotate superior pole medially (=intorsion) – rotate superior pole laterally (=extorsion) Only the medial rectus and lateral rectus have pure, singular actions. All others move the eyeball on 3 different axes. Extraocular Muscles Muscle Origin Insertion Innervation Function Levator palpebrae Lesser wing of sphenoid Skin of upper eyelid Oculomotor n. -

Malignant Melanoma of the Lacrimal Sac: Case Report and Major Review with Treatment Update
Journal of Ophthalmology & Visual Neurosciences Case report Malignant Melanoma of the Lacrimal Sac: Case Report and Major Review with Treatment Update This article was published in the following Scient Open Access Journal: Journal of Ophthalmology & Visual Neurosciences Received November 28, 2016; Accepted December 10, 2016; Published December 20, 2016 Lindsay A McGrath1,2 and Stephen B O’Hagan1,3* Abstract 1 Cairns Base Hospital, Ophthalmology Department, Purpose: To present a rare case of Primary Lacrimal Sac Melanoma, and review all Queensland 4870, Australia 2University of Queensland, Brisbane, Queensland reports of this condition in the literature to date. 4072, Australia Methods: In this review the clinical characteristics, presenting symptoms, treatment 3James Cook University, Cairns, Queensland, and morbidity of all patients with lacrimal sac melanoma reported in the literature from 1926 Australia to the present. We have also discussed new approaches available for adjuvant radiotherapy in the context of this frequently recurrent tumour. Results: Primary Melanoma of the Lacrimal Sac is a rare disease which is frequently diagnosed late. Common presenting symptoms include epiphora, blood-stained tears and painless swelling. Intensity modulated radiation therapy appears to hold promise in the adjuvant treatment of this disease, to reduce morbidity and mortality from recurrence and/ or metastasis. Conclusions: Existing case series and reports of Lacrimal Sac Melanoma describe a variety of treatment regimens and poor follow-up - highlighting the lack of a widely accepted strategy to prevent recurrence of disease. This case and review reminds practitioners of presenting signs and symptoms that should raise suspicion of Lacrimal Sac Melanoma, and a contemporary approach to adjuvant radiation therapy. -

Table 1-1 Bones of the Orbit
6 ● Neuro-Ophthalmology Planum sphenoidale Superior orbital fissure Optic canal Tuberculum sella Cavernous Anterior clinoid Pituitary sinus fossa Foramen ovale Carotid canal Foramen spinosum Foramen lacerum Clivus Petrous portion Dorsum sella of temporal bone Figure 1-3 Parasellar bony anatomy demonstrates the relationship of the pituitary fossa to the cavernous sinus, including the foramina of the skull base. The foramen lacerum is filled with cartilage and contains the artery of the pterygoid canal, the nerve of the pterygoid canal, and the venous drainage structures. The carotid artery enters the skull base through the carotid canal. (Courtesy of Albert L. Rhoton Jr, MD.) Frontal bone Lesser wing of sphenoid bone Superior orbital Optic canal fissure Greater wing of Ethmoidal bone sphenoid bone Lacrimal bone Zygomatic bone Lacrimal sac Palatine bone fossa Inferior orbital Maxillary bone fissure Figure 1-4 Anatomy of the orbit. Bony anatomy of the right orbital apex. The optic canal trans- mits the optic nerve, ophthalmic artery, and some oculosympathetic fibers. The superior orbital fissure, between the greater and lesser wings of the sphenoid bone, transmits CNs III, IV, and VI; the ophthalmic division of CN V (CN V1); the oculosympathetics; and the superior ophthalmic vein. (Illustration by Dave Peace.) Table 1-1 Bones of the Orbit Orbital Roof Lateral Wall Orbital Floor Medial Wall Frontal Zygomatic Zygomatic Maxillary Lesser wing of sphenoid Greater wing of sphenoid Maxillary Lacrimal Palatine Ethmoid Lesser wing of sphenoid CHAPTER 1: Neuro- Ophthalmic Anatomy ● 7 The superior orbital rim is made up of the frontal bone, which connects to the zygomatic bone laterally at the frontozygomatic suture.