Washington Hospital Postpartum 4-2018.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Alcohol, Breastfeeding, and Development at 18 Months
Alcohol, Breastfeeding, and Development at 18 Months Ruth E. Little, ScD*; Kate Northstone, MSc‡; Jean Golding, PhD, ScD‡; and the ALSPAC Study Team‡ ABSTRACT. Objective. We aimed to replicate a pre- literature search, we found only 1 systematic study1 vious study of 1-year-olds that reported a deficit in motor that measured drinking during lactation and subse- development associated with moderate alcohol use dur- quent child development. The authors reported a ing lactation, using a different but comparable popula- decrease in the motor development of infants at 1 tion. year of age, as measured by the Bayley Scales,2 when Methodology. The mental development of 915 18- the lactating mother had as little as 1 drink daily in month-old toddlers from a random sample of a longitu- dinal population-based study in the United Kingdom the first 3 months after delivery. This result was was measured using the Griffiths Developmental Scales. independent of drinking during pregnancy. Frequent self-administered questionnaires during and Lactation is the preferred method of early infant after pregnancy provided maternal data. The dose of feeding, and drinking alcohol is a common social alcohol available to the lactating infant was obtained by custom in most of the western world. Knowing the multiplying the alcohol intake of the mother by the pro- effect on the infant when lactation and alcohol drink- portion of breast milk in the infant’s diet. We compared ing are combined is of high importance, especially in this dose with the Griffiths Scales of Mental Develop- view of the previous report of its adverse effects. -

A Guide to Obstetrical Coding Production of This Document Is Made Possible by Financial Contributions from Health Canada and Provincial and Territorial Governments
ICD-10-CA | CCI A Guide to Obstetrical Coding Production of this document is made possible by financial contributions from Health Canada and provincial and territorial governments. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government. Unless otherwise indicated, this product uses data provided by Canada’s provinces and territories. All rights reserved. The contents of this publication may be reproduced unaltered, in whole or in part and by any means, solely for non-commercial purposes, provided that the Canadian Institute for Health Information is properly and fully acknowledged as the copyright owner. Any reproduction or use of this publication or its contents for any commercial purpose requires the prior written authorization of the Canadian Institute for Health Information. Reproduction or use that suggests endorsement by, or affiliation with, the Canadian Institute for Health Information is prohibited. For permission or information, please contact CIHI: Canadian Institute for Health Information 495 Richmond Road, Suite 600 Ottawa, Ontario K2A 4H6 Phone: 613-241-7860 Fax: 613-241-8120 www.cihi.ca [email protected] © 2018 Canadian Institute for Health Information Cette publication est aussi disponible en français sous le titre Guide de codification des données en obstétrique. Table of contents About CIHI ................................................................................................................................. 6 Chapter 1: Introduction .............................................................................................................. -
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
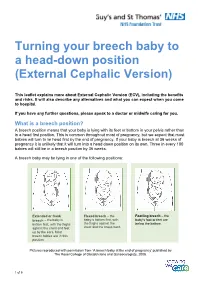
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus). -

Dermatology and Pregnancy* Dermatologia E Gestação*
RevistaN2V80.qxd 06.05.05 11:56 Page 179 179 Artigo de Revisão Dermatologia e gestação* Dermatology and pregnancy* Gilvan Ferreira Alves1 Lucas Souza Carmo Nogueira2 Tatiana Cristina Nogueira Varella3 Resumo: Neste estudo conduz-se uma revisão bibliográfica da literatura sobre dermatologia e gravidez abrangendo o período de 1962 a 2003. O banco de dados do Medline foi consul- tado com referência ao mesmo período. Não se incluiu a colestase intra-hepática da gravidez por não ser ela uma dermatose primária; contudo deve ser feito o diagnóstico diferencial entre suas manifestações na pele e as dermatoses específicas da gravidez. Este apanhado engloba as características clínicas e o prognóstico das alterações fisiológicas da pele durante a gravidez, as dermatoses influenciadas pela gravidez e as dermatoses específi- cas da gravidez. Ao final apresenta-se uma discussão sobre drogas e gravidez Palavras-chave: Dermatologia; Gravidez; Patologia. Abstract: This study is a literature review on dermatology and pregnancy from 1962 to 2003, based on Medline database search. Intrahepatic cholestasis of pregnancy was not included because it is not a primary dermatosis; however, its secondary skin lesions must be differentiated from specific dermatoses of pregnancy. This overview comprises clinical features and prognosis of the physiologic skin changes that occur during pregnancy; dermatoses influenced by pregnancy and the specific dermatoses of pregnancy. A discussion on drugs and pregnancy is presented at the end of this review. Keywords: Dermatology; Pregnancy; Pathology. GRAVIDEZ E PELE INTRODUÇÃO A gravidez representa um período de intensas ções do apetite, náuseas e vômitos, refluxo gastroeso- modificações para a mulher. Praticamente todos os fágico, constipação; e alterações imunológicas varia- sistemas do organismo são afetados, entre eles a pele. -

14. Management of Diabetes in Pregnancy: Standards of Medical
Diabetes Care Volume 42, Supplement 1, January 2019 S165 14. Management of Diabetes in American Diabetes Association Pregnancy: Standards of Medical Care in Diabetesd2019 Diabetes Care 2019;42(Suppl. 1):S165–S172 | https://doi.org/10.2337/dc19-S014 14. MANAGEMENT OF DIABETES IN PREGNANCY The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care. Members of the ADA Professional Practice Committee, a multidisciplinary expert committee, are responsible for updating the Standards of Care annually, or more frequently as warranted. For a detailed description of ADA standards, statements, and reports, as well as the evidence-grading system for ADA’s clinical practice recommendations, please refer to the Standards of Care Introduction. Readers who wish to comment on the Standards of Care are invited to do so at professional.diabetes.org/SOC. DIABETES IN PREGNANCY The prevalence of diabetes in pregnancy has been increasing in the U.S. The majority is gestational diabetes mellitus (GDM) with the remainder primarily preexisting type 1 diabetes and type 2 diabetes. The rise in GDM and type 2 diabetes in parallel with obesity both in the U.S. and worldwide is of particular concern. Both type 1 diabetes and type 2 diabetes in pregnancy confer significantly greater maternal and fetal risk than GDM, with some differences according to type of diabetes. In general, specific risks of uncontrolled diabetes in pregnancy include spontaneous abortion, fetal anomalies, preeclampsia, fetal demise, macrosomia, neonatal hypoglycemia, and neonatal hyperbilirubinemia, among others. -

Maternal Movement and Position Changes to Facilitate Labor Progress Have Been Discussed in the Literature for Decades
ELAINE ZWELLING, PHD, RN, LCCE, FACCE Abstract The benefi ts of maternal movement and position changes to facilitate labor progress have been discussed in the literature for decades. Recent routine interventions such as amniotomy, induction, fetal monitoring, and epidural anesthesia, as well as an increase in maternal obesity, have made position changes during labor challenging. The lack of maternal changes in position throughout labor can contribute to dystocia and increase the risk of cesarean births for failure to progress or descend. This article provides a historical review of the research fi ndings related to the effects of maternal positioning on the labor process and uses six physiological principles as a framework to offer sug- gestions for maternal positioning both before and after epidural anesthesia. Key Words Birth; Childbirth; Labor, fi rst stage; Labor, second stage; Maternity nursing; Obstetrical nursing; Maternal postures; Maternal positioning. Overcoming the Challenges: Maternal Movement 72 volume 35 | number 2 March/April 2010 or centuries laboring women chose to remain dural anesthesia, found that women who were able to mobile and upright, using positions such as change positions regularly or maintain upright positions standing, sitting, kneeling, hands and knees, or during labor were more comfortable and required less Fsquatting (Gupta & Nikodem, 2000; Johnson, pain medication (Atwood, 1976; de Jong et al., 1997; En- Johnson, & Gupta, 1991). Today immobility throughout gelmann, 1977; Johnson et al., 1991). For instance, Ada- the labor process has become a common occurrence for chi, Shimada, and Usul (2003) found in their study of 58 many childbearing women. Increased medical manage- laboring women that a sitting position decreased labor ment, obesity, lack of patient understanding about the pain in contrast with supine positioning. -

Variation in Fetal Presentations and Positions Among Women in Warri, Delta State, Nigeria
World Research Journal of Obstetrics and Gynecology ISSN: 2277-6001, Volume 2, Issue 1, 2013, pp.-10-12. Available online at http://www.bioinfopublication.org/jouarchive.php?opt=&jouid=BPJ0000126 VARIATION IN FETAL PRESENTATIONS AND POSITIONS AMONG WOMEN IN WARRI, DELTA STATE, NIGERIA OLANIYAN O.T.1*, MERAIYEBU A.B.1, ALELE J.Y.1, DARE J.B.2, ATSUKWEI D.1 AND ADELAIYE A.B.1 1Department of Physiology, Bingham University, Karu, Nasarawa, Nigeria. 2Department of Anatomy, Bingham University, Karu, Nasarawa, Nigeria. *Corresponding Author: Email- [email protected] Received: November 21, 2013; Accepted: December 23, 2013 Abstract- This study investigates the various fetal presentations among women in Warri and the various predisposing factors which may have possibly brought about these variations; the major positions considered were cephalic, breech and transverse, with the considered influencing factors being gestational age of the fetus, maternal age, amniotic fluid volume, parity, and method of previous deliveries. A total of 105 ultra- sound fetal biometries with a total of 108 fetuses, between 15-40 weeks of gestational age, and maternal age between 19 and 40 were used for this study. Fetal ultrasound biometry was used to find out information about the fetus including gestational age, amniotic fluid volume, presentation of the fetus and a questionnaire was used to take information about the mother including maternal age, parity, and method of previous delivery (ies). The result showed that a total of 82 fetuses (75.9%) were Cephalic babies, 19 (17.6%) were Breech and 7 (6.5%) are transverse. Out of the 105 women, there were 102 (77.1% cephalic, 18.3% breech, 4.8% transverse) women with adequate amniotic fluid volume and 1 woman (with a cephalic fetus) with average amniotic fluid volume and 2 women (with transverse foetuses) with low amniotic fluid volume. -

3. Physiologic (Spontaneous) Onset of Labor Versus Scheduled Birth
3. Physiologic (Spontaneous) Onset of Labor versus Scheduled Birth A new report, Hormonal Physiology of Childbearing: Evidence and Implications for Women, Babies, and Maternity Care (2015), synthesizes an extensive literature about hormonally-driven processes of parturition and the early postpartum period. The following information is drawn from this report. Many women and babies experience scheduled birth – induced labor and/or prelabor cesarean – annually in the United States.1 This fact sheet highlights key benefits of the spontaneous, physiologic onset of labor at term, including fully experiencing beneficial hormonal actions of late pregnancy and early labor, and identifies practices that support hormonal physiology when scheduled birth is medically necessary. Benefits of hormonal preparations of late pregnancy and of physiologic onset of labor Hormonal processes that lead up to the physiologic onset of labor prepare mother and fetus/newborn for upcoming tasks and phases. For example: Increases in oxytocin2 and prostaglandin3 receptors, at the physiologic onset of labor prime the uterus to promote effective contractions in labor. Increases in brain-based (central) receptors for beta-endorphins prepare endogenous pain-relieving pathways (to date, found in animal studies).4 Elevations in mammary and central oxytocin and prolactin receptors prepare for breastfeeding and maternal-infant biological bonding.5 Rising cortisol supports maturation of the fetal lungs and other organs. Prelabor preparations in oxytocin and catecholamine systems promote fetal protective processes in labor and optimal newborn transition.6 Practices that support beneficial hormonal action when scheduled birth is necessary When scheduled birth and other interventions are medically necessary, childbearing women and newborns can benefit from support of physiologic processes as far as safely possible. -

The American Rescue Plan Act's State Option to Extend Postpartum
The American Rescue Plan Act’s State Option to Extend Postpartum Coverage Authored by Manatt Health April, 2021 Introduction The American Rescue Plan Act of 2021 (ARP) establishes a new state option to extend Medicaid and Children's Health Insurance Program (CHIP) coverage for pregnant women for one year following the baby’s birth.1 Under current law, Medicaid and CHIP pregnant women’s coverage extends only through 60 days postpartum. A woman loses her Medicaid or CHIP coverage at the end of her 60-day postpartum period if she is not eligible for coverage under another Medicaid eligibility category (e.g., the new adult or parent group). ARP’s new state option to extend continuous coverage for one-year postpartum enables states to take a major step towards improving health outcomes for postpartum women and their babies by mitigating coverage loss, providing comprehensive coverage in the postpartum period to address maternal mortality and morbidity, and advancing health equity. There is considerable evidence supporting the policy decision to extend postpartum coverage; about 12 percent of pregnancy-related deaths occur between six weeks and one year postpartum.2 Despite approximately 60 percent of all maternal deaths in the United States (U.S.) being preventable, an estimated 700 women die each year as a result of pregnancy or delivery complications, and women of color are disproportionately affected.3 Black women in 2018, for example, were about 2.5 times more likely to suffer a pregnancy-related death than white women.4 Maternal morbidity in the U.S. has been on the rise since 1993, with women of color similarly experiencing significantly higher rates of severe maternal morbidity than their white counterparts.5 Pregnancy-related complications affecting the mother tend to translate to 1 American Rescue Plan Act of 2021, H.R.1319, § 9812 and § 9822. -

Module Presentation
Module Presentation How to best use the Modules To make the best use of this training we encourage you to complete each Module in order following the format below: 1. Read Module Presentation. Added explanations can be found in the HELPER Guidelines and in the extra information section if there is one. 2. Complete the Extraction/Scenario training exercises. The extraction exercises use de-identified and altered patient medical records. Enter the requested information into the provided section from the Birth Certificate Workbook. The Scenarios are situations you may encounter as you collect information from your patients’ medical records. 3. Check your responses using the answer sheets immediately following the segment completed 4. Complete the Module specific Evaluation, as before the answers are immediately following the Evaluation 5. If not already done, read extra training materials, if available. If you have questions about how to answer any of the requests for information in the NYS Certification of Live Birth Training Modules, please contact Rosemary Varga (585-275-8737). *”Coding” is a convenient although slightly misleading term for entering the needed information in the Statewide Perinatal Data system. True “coding” is the entry of predetermined numbers into a system that can then rate the material. We do not use numbers rather we enter the requested information. Module Three Labor & Delivery Part I Labor & Delivery Fields •Labor & Delivery information is found in the mother’s chart with much of the information on the L & D flowsheet/summary. A copy of this information may also be found in the infant’s chart. 2 Mother Transferred in Antepartum •Only complete these fields if the mother was transferred for medical reasons NYS GUIDELINES 3 Mother’s Weight at Delivery •Mother’s weight at delivery will often be found on the L&D flowsheet If you can’t find mother’s weight at delivery in the L&D information you can use the mother’s weight at her last prenatal visit if the visit was within 2 weeks of delivery. -

HTSP 101: Everything You Want to Know About Healthy Timing and Spacing of Pregnancy
HTSP 101: Everything You Want to Know About Healthy Timing and Spacing of Pregnancy Healthy Timing and Spacing of Pregnancy (HTSP) is an intervention to help women and families delay or space their pregnancies to achieve the healthiest outcomes for women, newborns, infants, and children, within the context of free and informed choice, taking into account fertility intentions and desired family size. Background Over the past few years, the United States Agency Qualitative studies conducted by USAID in for International Development (USAID) has Pakistan, India, Bolivia, and Peru showed that sponsored a series of studies on pregnancy spacing women and couples are interested in the healthiest and health outcomes. The research objective was to time to become pregnant versus when to give birth. assess, from the best available evidence, the effects In this way, HTSP differs from previous birth of pregnancy spacing on maternal, newborn and spacing approaches that refer only to the interval child health outcomes. In June 2005, the World after a live birth and when to give birth. HTSP also Health Organization (WHO) convened a panel of 30 provides guidance on the healthiest age for the first technical experts to review six USAID-sponsored pregnancy. studies. Based on their review of the evidence, the technical experts made two recommendations* to the Thus, HTSP encompasses a broader concept of the WHO, which are included in a report and policy reproductive cycle starting from healthiest age for brief1: the first pregnancy in adolescents, to spacing subsequent pregnancies following a live birth, still • After a live birth, the recommended minimum birth, miscarriage or abortion – capturing all interval before attempting the next pregnancy is pregnancy-related intervals in a woman’s at least 24 months in order to reduce the risk of reproductive life. -

Melasma and Endocrine Disorders
igmentar f P y D l o i a so n r r d Muller and Rees, Pigmentary Disorders 2014, S1 u e r o J s Journal of Pigmentary Disorders DOI: 10.4172/2376-0427.S1-001 ISSN: 2376-0427 Review Article Open Access Melasma and Endocrine Disorders Ilaria Muller* and Aled Rees Centre for Endocrine and Diabetes Sciences, Institute of Molecular & Experimental Medicine, School of Medicine, Cardiff University, UK Abstract Melasma is an acquired and chronic disorder characterized by a localized symmetrical hypermelanosis of the face or, less frequently, involving the neck and forearms. It occurs with a high prevalence during pregnancy, especially during the second half of the gestational period, and in women taking exogenous female hormones. Melasma has also rarely been described in males, especially those affected by primary hypogonadism or taking estrogens for prostatic cancer. Melasma thus appears to be pathologically related to female sex hormones, but this is not consistently reflected in high circulating levels of estrogens or progesterone. This implies that other factors are likely to be relevant, including genetic predisposition, exposure to ultraviolet light, cosmetics and some medications. Melanocortins play a key role in melanogenesis but no cases of melasma have been described in pituitary or adrenal diseases, including those associated with an increase in serum ACTH. An association between melasma and thyroid disorders has been reported only once and not confirmed in subsequent studies. The skin is both a source of, and a target for vitamin D; however, no cases of melasma have been described in association with disordered vitamin D production.