Morbidity Status and Its Social Determinants Among Elderly
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Maladies Quarantenaires — Quarantinable Diseases
— 680 — NOTE SUR LES UNITÉS GÉOGRAPHIQUES — NOTE ON GEOGRAPHIC AREAS Il ne faudrait pas conclure de la présentation adoptée dans le The form of presentation in the Weekly Epidemiological Record Relevé épidémiologique hebdomadaire que l’Organisation Mondiale does not imply official endorsement or acceptance by the World de la Santé admet ou reconnaît officiellement le statut ou les limites Health Organization of the status or boundaries of the territories des territoires mentionnés. Ce mode de présentation n ’a d’autre as listed or described. It has been adopted solely for the purpose objet que de donner un cadre géographique aux renseignements of providing a convenient geographic basis for the information publiés. La même réserve vaut également pour toutes les notes herein. The same qualification applies to all notes and explana et explications relatives aux pays et territoires qui figurent dans tions concerning the geographic units for which data are provided. les tableaux. Les «circonscriptions» (voir définition de ce terme Local areas under the International Sanitary Regulations are dans le Règlement sanitaire international) sont présentées suivant presented as designated by health administrations. les notifications reçues des administrations sanitaires. L, MALADIES QUARANTENAIRES — QUARANTINABLE DISEASES Territoires infectés au 22 décembre 1969 — Infected areas as on 22 December 1969 Notifications reçues aux termes du Règlement sanitaire international Notifications received under the International Sanitary Regulations relating concernant les circonscriptions infectées ou les territoires où la présence to infected local areas and to areas in which the presence of quarantinable de maladies quarantenaires a été signalée (voir page 668). diseases was reported (see page 66$). X = Nouveaux territoires signalés. -

Uu METHODIST Episcopalfichurch; U.S.A
3 9002 07494 4506 0 T^r SECOND i s n i d $ * | « t i OF TH E STATIONS OF THE o f t h e !^ .i u u METHODIST EPISCOPALfiCHURCH; U.S.A. ■CO> ii A - For the Year 1836. 1 ! B d ix £ & A ' j. : V. 2. LUCKNOW: PRISTEP AT THE^i ST MISafOX PRKSS. I- i m I X D IS X .. I. PREFACE, ................... II. STATION REPORTS,— 1.— Bareilly, 2.— Girls’ Orphanage, 3.— Budaon, 4.—Nynee Tal, 5.—Shah j ahanpore, $.— Pilibheet, 7.— Lucknow, S.—Mission Press, 0.—Seetapore and Lukiinpore, 10.— Gondah, ... 11.—Roy-Bareilly, ... 12.—Nawabgunge, ... 13.—Jloradabad and Chandausi, 11.—Amroha and Babukera, ... 15.— Sambhal, 16.— Bijnour, 17.— Gurliwal (PaoH), TTT- APPENDIX A . Conference Statistics. 11 B. .Colportage Statistics, " C. Donors and Subscribers. SECOND » « i l i i e r t i i » i i m i m ï -ô i ««iFiasifis METHODIST EPISCOPAL CHUBOH, U.S.A. For the Year 1866. LUCKNOW: PRINTED AT THE AMERICAN METHODIST MISSION PRESS. 1867. PREFACE. T h e Metii odist E p is c o p a l C i i u ; c h M i s s io n in India now seucis out its second regular annual Eeport. I\iissionaries should not be too much concerned about what a certain class of per sons say in regard to their work, nor be too anxious to convince them of the importance and success of Missions. Generally their objections and criticisms come from a want of sympathy with Christianity, or from a concealed opposition to it, which cannot be easily overcome by any array of facts. -

Determinants of Childhood Immunisation Coverage in Urban Poor Settlements of Delhi, India: a Cross-Sectional Study
Open Access Research BMJ Open: first published as 10.1136/bmjopen-2016-013015 on 26 August 2016. Downloaded from Determinants of childhood immunisation coverage in urban poor settlements of Delhi, India: a cross-sectional study Niveditha Devasenapathy,1 Suparna Ghosh Jerath,1 Saket Sharma,1 Elizabeth Allen,2 Anuraj H Shankar,3 Sanjay Zodpey1 To cite: Devasenapathy N, ABSTRACT Strengths and limitations of this study Ghosh Jerath S, Sharma S, Objectives: Aggregate data on childhood et al. Determinants of immunisation from urban settings may not reflect the ▪ childhood immunisation We report current estimates of childhood com- coverage among the urban poor. This study provides coverage in urban plete immunisation including hepatitis B vaccine poor settlements of Delhi, information on complete childhood immunisation coverage from representative urban poor com- India: a cross-sectional study. coverage among the urban poor, and explores its munities in the Southeast of Delhi. BMJ Open 2016;6:e013015. household and neighbourhood-level determinants. ▪ The sample size was large and therefore our doi:10.1136/bmjopen-2016- Setting: Urban poor community in the Southeast effect estimates for coverage and determinants 013015 district of Delhi, India. were precise. Participants: We randomly sampled 1849 children ▪ We quantify unknown neighbourhood effects on ▸ Prepublication history and aged 1–3.5 years from 13 451 households in 39 this outcome using median ORs which are more additional material is clusters (cluster defined as area covered by a intuitively understood. available. To view please visit community health worker) in 2 large urban poor ▪ Based on the data, representative of only one the journal (http://dx.doi.org/ settlements. -

2I.Xn Visakhapatnam, District
Relevé épidém. hebd. I 1969, 44, 29-52 N° 2 Wkly Epidtm. Rec. | ORGANISATION MONDIALE DE LA SANTÉ WORLD HEALTH ORGANIZATION GENÈVE GENEVA RELEVÉ ÉPIDÉMIOLOGIQUE HEBDOMADAIRE WEEKLY EPIDEMIOLOGICAL RECORD Notifications et informations se rapportant à l’application Notifications under and information on the application of the du Règlement sanitaire international et notes relatives à la International Sanitary Regulations and notes on current incidence fréquence de certaines maladies of certain diseases Service de la Surveillance épidémiologique et de la Quarantaine Epidemiological Surveillance and Quarantine Unit Adresse télégraphique; EPIDNATIONS GENÈVE Telegraphic Address; EPIDNATIONS GENÈVE Télex 22335 Telex 22335 10 JANVIER 1969 44e ANNÉE — 44th YEAR 10 JANUARY 1969 MALADIES QUARANTENAÎRES — QUARANTINABLE DISEASES Territoires infectés au 9 janvier 1969 — Infected areas as on 9 January 1969 Notifications reçues aux termes du Règlement sanitaire international Notifications received under the International Sanitary Regulations relating concernant les circonscriptions infectées ou les territoires où la présence to infected local areas and to areas in which the presence of quarantinaBle de maladies quarantenaires a été signalée (voir page 549). diseases was reported (see page 549). X *= Nouveaux territoires signalés, X = Newly reported areas. ■ = Circonscriptions ou territoires notifiés aux termes de l'article 3 à la ■ — Areas notified under Article 3 on the date indicated. date donnée. Pour les autres territoires, la présence de maladies quarantenaires a été For the other areas, the presence of quarantinaBle diseases was notified notifiée aux termes des articles 4, 5 et 9 a) pour la période se terminant à la under Articles 4, 5 and 9 (a) for the period ending on the date indicated. -

The Private Schooling Phenomenon in India: a Review
DISCUSSION PAPER SERIES IZA DP No. 10612 The Private Schooling Phenomenon in India: A Review Geeta Gandhi Kingdon MARCH 2017 DISCUSSION PAPER SERIES IZA DP No. 10612 The Private Schooling Phenomenon in India: A Review Geeta Gandhi Kingdon IoE, University College London and IZA MARCH 2017 Any opinions expressed in this paper are those of the author(s) and not those of IZA. Research published in this series may include views on policy, but IZA takes no institutional policy positions. The IZA research network is committed to the IZA Guiding Principles of Research Integrity. The IZA Institute of Labor Economics is an independent economic research institute that conducts research in labor economics and offers evidence-based policy advice on labor market issues. Supported by the Deutsche Post Foundation, IZA runs the world’s largest network of economists, whose research aims to provide answers to the global labor market challenges of our time. Our key objective is to build bridges between academic research, policymakers and society. IZA Discussion Papers often represent preliminary work and are circulated to encourage discussion. Citation of such a paper should account for its provisional character. A revised version may be available directly from the author. IZA – Institute of Labor Economics Schaumburg-Lippe-Straße 5–9 Phone: +49-228-3894-0 53113 Bonn, Germany Email: [email protected] www.iza.org IZA DP No. 10612 MARCH 2017 ABSTRACT The Private Schooling Phenomenon in India: A Review* This paper examines the size, growth, salaries, per-pupil-costs, pupil achievement levels and cost-effectiveness of private schools, and compares these with the government school sector. -

Diversity of Waterbirds in Lucknow District, Uttar Pradesh, India
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 Index Copernicus Value (2013): 6.14 | Impact Factor (2013): 4.438 Diversity of Waterbirds in Lucknow District, Uttar Pradesh, India Amita Kanaujia1, Adesh Kumar2, Sonika Kushwaha3, Akhilesh Kumar4 Biodiversity & Wildlife Conservation Lab, Department of Zoology, University of Lucknow, Lucknow- 226007 Uttar Pradesh, India Abstract: For over a century, pioneering naturalists have determined the way in which waterbird conservation has evolved around the world and have been involved in the establishment of international organizations such as IUCN. The term, waterbird or aquatic bird is used to refer the birds that live on or around water bodies; they may be fresh water or marine. The enrichment of organic constituents accountable for the growth of aquatic weeds, phytoplankton and zooplankton therefore the wetlands are good habitat for availability of food stuff to various waterbirds in moderate proportion. This study presents diversity of water bird in Lucknow and adjacent areas where surveys have been conducted for two years (October 2012- September 2014) in different unprotected wetlands of Lucknow having N 26.84700 and E 80.94700 geographical coordinates. Total 71 Species of water bird representing 9 orders and 21 families were recorded from five different localities. Out of these 70 species, 25 species were residential, 14 species were residential/local migratory, 2 species were local migratory, 27 species were migratory while 2 species were residential/migratory. The study reveals that in Lucknow there are maximum populations of Migratory water birds followed by residential, residential/local migratory and residential/migratory species. The present study of wetlands helps to maintain a record of water bird to restore and maintain the present condition of wetland. -

Nv!Me 3 Public Disclosure Authorized
~- - \/nV!me 3 Public Disclosure Authorized COMBINED EXECUTIVE SUMIMARY (LUCKNOW-MIJZAFFARPUR NATIONAL HIGHWAY PROTECT) Public Disclosure Authorized Lucknow-Ayodhya Public Disclosure Authorized Gorakhpur Bypass National Highways Authority of India G-5 & 6, Sector-I 0, Dwarka Public Disclosure Authorized New Delhi-I 10075 ,- 4. v, it.. ; j i-4,vi X t CHAPTER 1 EXECUTIVE SUMMARY Independent Review and Consolidation of EIA, EMP & RAP for Lucknow-Ayodhya section on NH-28 and Gorakhpur Bypass Draft Final Consolidated Resettlement Action Plan F| ] ENXFNTIUE SIIMMARY 1.1 INTRODUCTION India has embarked on a 10-year highway transportation improvement program as a part of the nationa! nplic.v tn cl1nhli7ie it', ecnnnmv and tn increase saifetv an-id efficiency.v in ftridp and busines besides free movement of traffic. To achieve this, National Highways Authority of India (NHAI) an autonomous body under the .7ni0is.Iy of R,soadd Transport (T&Ha.LTA), envisgUth, Lit, litatio of sustainable transportation system in India. With its mandate to develop and maintain an enhanced quali.y 01 I-ighways, 1T1/-I nNaionaluder t1he NaLiolal Highway eVLeJVIlorIIL flail i,NIHL) las embarked on its second phase relating to the creation of a North-South corridor connecting Srinagar with Kanyakumari and of strengthening and enhancing the East-'vVest corr idor of tle country linking Silchar with Porbandar. The Government plans to complete the second phase of NHDP by December 2007, which includes UtAevelopmlent V,0Jhtl olf01 LVV-vo Co_;Aos,I LUOI. Lilth NoT--South+I1101LLIIL.)S.ULIi %-Col--iA-.0 ILLUSJ ah1U.an the-Llt, Eas-WesIt~UL..-)VY t,ai l..VIIIUVJI.Col-ido.A ~_;lOfP1, theLilt, 65-lU0J0_ Q -1Idl NS-EW corridors, 630-km have already been four-laned, while 416-km was under implementation anu tiie conuiacts fo1r tLiie renianing 58ii124,ml w-iill be awarded uiiuteL pilhas -Li. -
CUG No. / Email ID of JAIL OFFICIALS of up Sl.N Name of Institution Designation Mobile N0
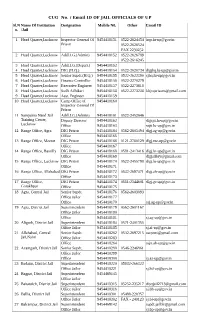
CUG No. / Email ID OF JAIL OFFICIALS OF UP Sl.N Name Of Institution Designation Mobile N0. Other Email ID o. /Jail 1 Head Quarter,Lucknow Inspector General Of 9454418151 0522-2624454 [email protected] Prison 0522-2626524 FAX 2230252 2 Head Quarter,Lucknow Addl.I.G.(Admin) 9454418152 0522-2626789 0522-2616245 3 Head Quarter,Lucknow Addl.I.G.(Depart.) 9454418153 4 Head Quarter,Lucknow DIG (H.Q.) 9454418154 0522-2620734 [email protected] 5 Head Quarter,Lucknow Senior Supdt.(H.Q.) 9454418155 0522-2622390 [email protected] 6 Head Quarter,Lucknow Finance Controller 9454418156 0522-2270279 7 Head Quarter,Lucknow Executive Engineer 9454418157 0522-2273618 8 Head Quarter,Lucknow Sodh Adhikari 9454418158 0522-2273238 [email protected] 9 Head Quarter,Lucknow Asst. Engineer 9454418159 10 Head Quarter,Lucknow Camp Office of 9454418160 Inspector General Of Prison 11 Sampurna Nand Jail Addl.I.G.(Admin) 9454418161 0522-2452646 Training Center, Deputy Director 9454418162 [email protected] Lucknow Office 9454418163 [email protected] 12 Range Office, Agra DIG Prison 9454418164 0562-2605494 [email protected] Office 9454418165 13 Range Office, Meerut DIG Prison 9454418166 0121-2760129 [email protected] Office 9454418167 14 Range Office, Bareilly DIG Prison 9454418168 0581-2413416 [email protected] Office 9454418169 [email protected] 15 Range Office, Lucknow DIG Prison 9454418170 0522-2455798 [email protected] Office 9454418171 16 Range Office, Allahabad DIG Prison 9454418172 0532-2697471 [email protected] Office 9454418173 17 Range Office, DIG Prison 9454418174 0551-2344601 [email protected] Gorakhpur Office 9454418175 18 Agra, Central Jail Senior Supdt. -

Lucknow City – India Groundwater Resource Use & Strategic Planning
Briefing Note Series GW MATE BriefingBriefing Note Note Series Series Groundwater global water partnership associate program Groundwater• world bank Management GW MATE Briefing Note Series global water partnership associate program Advisory Team Management Advisory Team SustainableSustainable GroundwaterGroundwater Management: Management ConceptsLessons and Tools from Practice Case Profile Collection Number 23 Lucknow City – India Groundwater Resource Use & Strategic Planning Needs April 2009 Authors: Stephen Foster and N. K. Choudhary** Project Task Managers: Javier Zuleta & Sanjay Pahuja This Case Profile comprises a diagnosis of the groundwater resource situation in Lucknow City, the Uttar Pradesh (UP) state capital, which can be regarded in many ways as indicative of the position of most rapidly-expanding cities and large towns on the Gangetic Plain. The assessment includes the development of a more strategic approach to improvement of ‘water-supply security’ in the face of continued expansion and of the probable impacts of accelerated climate change, including definition of the further investigation required for this purpose. The work constitutes a contribution to both the World Bank-financed UP Water Sector Restructuring Project and the World Bank-India AAA Study on Political Economy of Groundwater Resource Management – and greatly benefited from effective local arrangements by the UP-Irrigation Department (PACT) and the UP-State Water Resources Agency (SWaRA). EVOLUTION OF URBAN GROUNDWATER USE Hydrogeological Setting of Lucknow City ● Around 85% of the land-area of Lucknow City is situated on the Central Ganga alluvial plain, and stretches across both banks of the Gomti River (Figure 1) – which is an entirely lowland river naturally dependent on groundwater discharge for its dry-weather flow. -
Asserting Rights Accessingentitlements
Asserting Rights Accessing Entitlements A report on the implementation of the Project: “Increasing access to information on the Government Schemes and Entitlements in Backward Districts in Northern India” in Barabanki and Pratapgarh in Uttar Pradesh Asserting Rights, A report on the implementation of the Project: “Increasing access to information on Accessing the Government Schemes and Entitlements in Backward Districts in Northern India” in Entitlements Barabanki and Pratapgarh in Uttar Pradesh Backgound About 13.2% of Pratapgarh’s population and 22.61% of Barabanki’s population is Muslim. And Uttar India’s most populous state, Uttar Pradesh, is often Pradesh has one the largest concentrations of SCs said to be many worlds within one. Barabanki district, in the country. The backwardness of these commu- adjoining Lucknow district and Pratapgarh district al- nities can be measured through many parameters most 150 kilometres to the east of Lucknow city are - their access to healthcare, housing, employment two such worlds. Despite having unique histories and etc. But, let us take the example of literacy. Accord- even more unique roles in contemporary politics, both ing to the 2011 national census, literacy rate among Pratapgarh and Barabanki have not been able to leave the SCs in Uttar Pradesh is 38.29% and among Mus- the list of India’s most backward districts. lims across the state is 42%. The literacy rate of both communities is lower than the district average of In 2014 ActionAid India initiated a project to address 51.90% in Pratapgarh and 61.75% in Barabanki. With the gap between community action for rights and en- such low levels of literacy and living in packed neigh- titlements and also focuses on increasing the abili- bourhoods, these communities have to struggle hard ty of the local state to provide an effective response. -
![Eastern Command, India (1939)]](https://docslib.b-cdn.net/cover/5932/eastern-command-india-1939-2595932.webp)
Eastern Command, India (1939)]
2 October 2020 [EASTERN COMMAND, INDIA (1939)] Meerut District rd (3 Indian Infantry Division) (1) H.Q. King George V’s Own Bengal Sappers and Miners (2) 4th Field Company, King George V’s Own Bengal Sappers and Miners 6th Army Troops Company, King George V’s Own Bengal Sappers and Miners 8th Army Troops Company, King George V’s Own Bengal Sappers and Miners No. 31 Field Troop, King George V’s Own Bengal Sappers and Miners No. 35 Field Troop, King George V’s Own Bengal Sappers and Miners 43rd Divisional H.Q. Company, King George V’s Own Bengal Sappers and Miners Training Battalion, King George V’s Own Bengal Sappers and Miners 7th (Dehra Dun) Infantry Brigade (3) 2nd Bn. 2nd King Edward VII’s Own Gurkha Rifles (The Sirmoor Rifles) 1st Bn. 9th Gurkha Rifles 2nd Bn. 9th Gurkha Rifles 8th (Bareilly) Infantry Brigade (4) 2nd Bn. The Oxfordshire and Buckinghamshire Light Infantry 10th Bn. 4th/9th Regiment (Regimental Centre) 2nd Bn. 18th Royal Garhwal Rifles – Lansdowne 10th Bn. 18th Royal Garhwal Rifles (Regimental Centre) – Lansdowne 11th Bn. 18th Royal Garhwal Rifles (Indian Territorial Force) – Lansdowne ©www.BritishMilitaryHistory.co.uk Page 1 2 October 2020 [EASTERN COMMAND, INDIA (1939)] NOTES: 1. The Meerut District (based just to the north of Delhi); was a ‘First Class’ District, i.e., it also functioned as the embryonic headquarters of the 3rd Indian Infantry Division. The General Officer Commanding from 25 January 1940 until 15 January 1943 was Major General H. M. McDONALD, C.B., C.I.E., D.S.O. -

Prevalence of Porcine Cysticercosis in Bareilly, Northern India
Veterinary World, EISSN: 2231-0916 RESEARCH ARTICLE Available at www.veterinaryworld.org/Vol.7/May-2014/2.pdf Open Access Prevalence of porcine cysticercosis in Bareilly, Northern India B. C. Saravanan1111231 , H. V. Manjunathachar , A. K. Tewari , S. C. Gupta , K. Karthik , P. Tamilmahan and N. R. Sudhakar 1. Division of Parasitology, Indian Veterinary Research Institute, Izatnagar-243122, Uttar Pradesh, India; 2. Division of Bacteriology and Mycology, Indian Veterinary Research Institute, Izatnagar-243122, Uttar Pradesh, India; 3. Division of Surgery, Indian Veterinary Research Institute, Izatnagar-243122, Uttar Pradesh, India Corresponding author: B. C. Saravanan, email: [email protected], Tel.: +91-581-440368 Received:15-03-2014, Revised: 05-04-2014, Accepted: 08-04-2014, Published online: 03-05-2014 doi: 10.14202/vetworld.2014.281-283 How to cite this article: Saravanan BC, Manjunathachar HV, Tewari AK, Gupta SC, Karthik K, Tamilmahan P and Sudhakar NR (2014) Prevalence of porcine cysticercosis in Bareilly, Northern India,Veterinary World 7(5): 281-283. Abstract Aim: The objective of this study was to investigate the prevalence ofTaenia solium cysticercosis in pigs slaughtered at makeshift houses in Bareilly, Northern India. Materials and Methods: Local makeshift slaughter houses were visited weekly in Bareilly to explore the prevalence of the porcine cysticercosis in this area. 175 pigs were screened for cysticercosis and prevalence was correlated to age, sex and breed of pigs. Results: A total of 175 pigs were examined for cysticercosis out of which 9 (5.14%) were found positive for porcine cysticercosis. Sex-wise prevalence of this infection in male and female was recorded as 4.82% (4/83) and 5.43% (5/92), respectively.