DUTREBIS™ (Lamivudine and Raltegravir)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

United States Patent (19) 11 Patent Number: 5,993,812 Tsoukas Et Al
USOO5993812A United States Patent (19) 11 Patent Number: 5,993,812 TSOukas et al. (45) Date of Patent: Nov.30, 1999 54 METHOD OF DELAYING THE Brunkhorst et al., Infection 18:28-32, 1990. PROGRESSION OF AN INFECTION WITH Coyle et al., Changes in the Lymphocyte Count and Lym THE HUMAN IMMUNODEFICIENCY VIRUS phocyte Subsets After Splenectomy in Human Immunode ficiency Virus Infection, Letters and Correspondence, pp. 75 Inventors: Christos M. Tsoukas, Montreal; Barry 144-146. Michael Woloski, Winnipeg, both of DeSimone et al., Immunopharma. and Immunotoxic., Canada 13:447-458, 1991. Gringeri et al., British Journal of Haemotology, 80:337-340, 73 Assignee: Cangene Corporation, Winnipeg, 1992. Canada Gingör et al., Eur. J. Pediatr., 152:650–654, 1993. Mofenson and Moye, Pediatric Research, 33:80-S89, 1993. 21 Appl. No.: 08/835,400 Mofenson et al., Journal of Acquired Immune Deficiency 22 Filed: Apr. 7, 1997 Syndrome, 6:1103-1113, 1993. Schrappe-Bächer et al., Vox Sang, 59:3-14, 1990. Related U.S. Application Data Shearer et al., Ann. N.Y. Acad. Sci., pp. 35-51. Wagner et al., Arch. of Disease in Childhood., 63 Continuation-in-part of application No. 08/713,765, Sep. 13, 67:1267-1271, 1992. 1996, abandoned. Watson, et al., “Recombinant DNA”, Scientific American 60 Provisional application No. 60/003,756, Sep. 14, 1995. Books, Chapter 25. 51) Int. Cl. ............................ A61K 39/395; CO7K 1/00 Okesenhendeler, et al., “Anti-RH immunoglobulin therapy 52 U.S. Cl. ................... 424/130.1; 530/350, 530/388.7; for human immunodeficiency virus-related immune throm 424/142.1; 424/141.1; 424/153.1 bocytopenic purpura’, Blood, 71 (5) 1499-502. -

VIDEX (Didanosine) Chewable/Dispersible Buffered Tablets
Rx only VIDEXâ (didanosine) â VIDEX (didanosine) Chewable/Dispersible Buffered Tablets â VIDEX (didanosine) Buffered Powder for Oral Solution â VIDEX (didanosine) Pediatric Powder for Oral Solution (Patient Information Leaflet Included) WARNING FATAL AND NONFATAL PANCREATITIS HAVE OCCURRED DURING THERAPY WITH VIDEX USED ALONE OR IN COMBINATION REGIMENS IN BOTH TREATMENT-NAIVE AND TREATMENT-EXPERIENCED PATIENTS, REGARDLESS OF DEGREE OF IMMUNOSUPPRESSION. VIDEX SHOULD BE SUSPENDED IN PATIENTS WITH SUSPECTED PANCREATITIS AND DISCONTINUED IN PATIENTS WITH CONFIRMED PANCREATITIS (SEE WARNINGS). LACTIC ACIDOSIS AND SEVERE HEPATOMEGALY WITH STEATOSIS, INCLUDING FATAL CASES, HAVE BEEN REPORTED WITH THE USE OF NUCLEOSIDE ANALOGUES ALONE OR IN COMBINATION, INCLUDING DIDANOSINE AND OTHER ANTIRETROVIRALS. FATAL LACTIC ACIDOSIS HAS BEEN REPORTED IN PREGNANT WOMEN WHO RECEIVED THE COMBINATION OF DIDANOSINE AND STAVUDINE WITH OTHER ANTIRETROVIRAL AGENTS. THE COMBINATION OF DIDANOSINE AND STAVUDINE SHOULD BE USED WITH CAUTION DURING PREGNANCY AND IS RECOMMENDED ONLY IF THE POTENTIAL BENEFIT CLEARLY OUTWEIGHS THE POTENTIAL RISK. (SEE WARNINGS AND PRECAUTIONS: PREGNANCY.) Page 4 of 39 DESCRIPTION â VIDEX (didanosine) is a brand name for didanosine (ddI), a synthetic purine nucleoside analogue active against the Human Immunodeficiency Virus (HIV). VIDEX Chewable/Dispersible Buffered Tablets are available for oral administration in strengths of 25, 50, 100, 150, and 200 mg of didanosine. Each tablet is buffered with calcium carbonate and magnesium hydroxide. VIDEX tablets also contain aspartame, sorbitol, microcrystalline cellulose, polyplasdone, mandarin-orange flavor, and magnesium stearate. VIDEX Buffered Powder for Oral Solution is supplied for oral administration in single- dose packets containing 100, 167, or 250 mg of didanosine. Packets of each product strength also contain a citrate-phosphate buffer (composed of dibasic sodium phosphate, sodium citrate, and citric acid) and sucrose. -

Vitekta Pi.Pdf
HIGHLIGHTS OF PRESCRIBING INFORMATION -----------------------DOSAGE FORMS AND STRENGTHS-------------------- These highlights do not include all the information needed to use Tablets: 85 mg and 150 mg (3) VITEKTA safely and effectively. See full prescribing information for VITEKTA. --------------------------------CONTRAINDICATIONS------------------------------ VITEKTA® (elvitegravir) tablets, for oral use There are no contraindications to VITEKTA. (4) Initial U.S. Approval: 2012 Due to the need to use VITEKTA with a protease inhibitor coadministered with ritonavir, consult prescribing information of -------------------------------INDICATIONS AND USAGE------------------------- coadministered protease inhibitor and ritonavir for their VITEKTA is a human immunodeficiency virus type 1 (HIV-1) integrase contraindications. (4) strand transfer inhibitor used in combination with an HIV protease inhibitor coadministered with ritonavir and with other antiretroviral -------------------------WARNINGS AND PRECAUTIONS---------------------- drug(s) indicated for the treatment of HIV-1 infection in antiretroviral Do not use with protease inhibitors coadministered with cobicistat. treatment-experienced adults. (1) (5.2) Do not use with other elvitegravir-containing drugs, including Limitations of Use: STRIBILD. (5.2) There are no comparative pharmacokinetic or clinical data Immune reconstitution syndrome: May necessitate further evaluation evaluating VITEKTA with cobicistat as single entities compared to and treatment. (5.3) STRIBILD®. (1) --------------------------------ADVERSE REACTIONS----------------------------- VITEKTA coadministered with protease inhibitors and cobicistat is The most common adverse drug reaction to VITEKTA (all grades) is not recommended. (1) diarrhea. (6.1) Coadministration of VITEKTA with dosage regimens or HIV-1 protease inhibitors other than those presented in Table 1 is not To report SUSPECTED ADVERSE REACTIONS, contact Gilead recommended. (1) Sciences, Inc. at 1-800-GILEAD-5 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. -
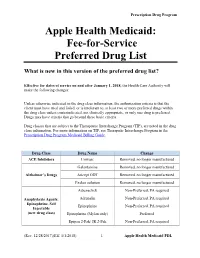
Fee-For-Service Preferred Drug List
Prescription Drug Program Apple Health Medicaid: Fee-for-Service Preferred Drug List What is new in this version of the preferred drug list? Effective for dates of service on and after January 1, 2018, the Health Care Authority will make the following changes: Unless otherwise indicated in the drug class information, the authorization criteria is that the client must have tried and failed, or is intolerant to, at least two or more preferred drugs within the drug class unless contraindicated, not clinically appropriate, or only one drug is preferred. Drugs may have criteria that go beyond these basic criteria. Drug classes that are subject to the Therapeutic Interchange Program (TIP), are noted in the drug class information. For more information on TIP, see Theraputic Interchange Program in the Prescription Drug Program Medicaid Billing Guide. Drug Class Drug Name Change ACE Inhibitors Univasc Removed, no longer manufactured Galantamine Removed, no longer manufactured Alzheimer’s Drugs Aricept ODT Removed, no longer manufactured Exelon solution Removed, no longer manufactured Adrenaclick Non-Preferred, PA required Anaphylaxis Agents: Adrenalin Non-Preferred, PA required Epinephrine, Self Epinephrine Non-Preferred, PA required Injectable (new drug class) Epinephrine (Mylan only) Preferred Epipen 2-Pak/ JR 2-Pak Non-Preferred, PA required (Rev. 12/28/2017)(Eff. 1/1/2018) – 1 – Apple Health Medicaid PDL Prescription Drug Program Renamed drug class “Anticoagulants: Anticoagulants Entire class Factor XA and Thrombin Inhibitors.” Anticoagulants: -

Managing Drug Interactions in the Treatment of HIV-Related Tuberculosis
Managing Drug Interactions in the Treatment of HIV-Related Tuberculosis National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination Managing Drug Interactions in the Treatment of HIV-Related Tuberculosis Centers for Disease Control and Prevention Office of Infectious Diseases National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination June 2013 This document is accessible online at http://www.cdc.gov/tb/TB_HIV_Drugs/default.htm Suggested citation: CDC. Managing Drug Interactions in the Treatment of HIV-Related Tuberculosis [online]. 2013. Available from URL: http://www.cdc.gov/tb/TB_HIV_Drugs/default.htm Table of Contents Introduction 1 Methodology for Preparation of these Guidelines 2 The Role of Rifamycins in Tuberculosis Treatment 4 Managing Drug Interactions with Antivirals and Rifampin 5 Managing Drug Interactions with Antivirals and Rifabutin 9 Treatment of Latent TB Infection with Rifampin or Rifapentine 10 Treating Pregnant Women with Tuberculosis and HIV Co-infection 10 Treating Children with HIV-associated Tuberculosis 12 Co-treatment of Multidrug-resistant Tuberculosis and HIV 14 Limitations of these Guidelines 14 HIV-TB Drug Interaction Guideline Development Group 15 References 17 Table 1a. Recommendations for regimens for the concomitant treatment of tuberculosis and HIV infection in adults 21 Table 1b. Recommendations for regimens for the concomitant treatment of tuberculosis and HIV infection in children 22 Table 2a. Recommendations for co-administering antiretroviral drugs with RIFAMPIN in adults 23 Table 2b. Recommendations for co-administering antiretroviral drugs with RIFAMPIN in children 25 Table 3. Recommendations for co-administering antiretroviral drugs with RIFABUTIN in adults 26 ii Introduction Worldwide, tuberculosis is the most common serious opportunistic infection among people with HIV infection. -

Review CCR5 Antagonists: Host-Targeted Antiviral Agents for the Treatment of HIV Infection, 4 Years On
Antiviral Chemistry & Chemotherapy 2010 20:179–192 (doi: 10.3851/IMP1507) Review CCR5 antagonists: host-targeted antiviral agents for the treatment of HIV infection, 4 years on Mike Westby1* and Elna van der Ryst1 1Pfizer Global Research and Development, Sandwich, Kent, UK *Corresponding author: e-mail: [email protected] The chemokine coreceptor 5 (CCR5) antagonists are anti- are in various stages of clinical development. In 2005, we retroviral agents with an extracellular, host-targeted reviewed the limited clinical data then available on CCR5 mechanism of action against HIV. Maraviroc, the first- antagonists. In this follow-up review, we revisit the field and in-class CCR5 antagonist, received regulatory approval in assess the clinical and virological data that have emerged 2007, becoming the first oral antiretroviral from a new in the 4 years since, with particular reference to maraviroc class in more than 10 years. Other compounds in this class for which the most comprehensive data currently exist. Introduction Chemokine coreceptor 5 (CCR5) antagonists are a new supporting the current and future role of small-molecule class of antiretroviral agents that inhibit HIV replica- CCR5 antagonists in the treatment of HIV infection. tion by binding to CCR5 on the surface of host target cells and preventing entry of viral strains reliant on this Status of CCR5 antagonists in clinical coreceptor for infection. The first and only currently development in 2005 approved agent within this class, maraviroc, received marketing authorisation in the USA, Europe and other Of the three small-molecule CCR5 antagonists in regions of the world in 2007, with an indication for clinical development in 2005, only maraviroc (Figure treatment-experienced adult patients with only CCR5- 1A) is currently approved for clinical use. -

Non-Anntoated Product Monograph
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION PrTRIUMEQ dolutegravir, abacavir, and lamivudine tablets 50 mg dolutegravir (as dolutegravir sodium), 600 mg abacavir (as abacavir sulfate) and 300 mg lamivudine Antiretroviral Agent ViiV Healthcare ULC 245, boulevard Armand-Frappier Laval, Quebec H7V 4A7 Date of Revision: January 31, 2020 Submission Control No: 233245 © 2020 ViiV Healthcare group of companies or its licensor Trademarks are owned by or licensed to the ViiV Healthcare group of companies Page 1 of 61 TABLE OF CONTENTS PAGE PART I: HEALTH PROFESSIONAL INFORMATION ........................................................ 3 SUMMARY PRODUCT INFORMATION ................................................................... 3 INDICATIONS AND CLINICAL USE ........................................................................ 3 CONTRAINDICATIONS ........................................................................................... 4 WARNINGS AND PRECAUTIONS............................................................................ 4 ADVERSE REACTIONS.......................................................................................... 11 DRUG INTERACTIONS .......................................................................................... 19 DOSAGE AND ADMINISTRATION ........................................................................ 24 OVERDOSAGE....................................................................................................... 26 ACTION AND CLINICAL PHARMACOLOGY........................................................ -

Of 43 Reference ID: 4711890 FULL PRESCRIBING INFORMATION: CONTENTS*
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use DOLUTEGRAVIR, EMTRICITABINE and TENOFOVIR -----------------------WARNINGS AND PRECAUTIONS------------------------ ALAFENAMIDE TABLETS safely and effectively. See full prescribing • Hypersensitivity reactions characterized by rash, constitutional findings, information for DOLUTEGRAVIR, EMTRICITABINE and and sometimes organ dysfunction, including liver injury have been TENOFOVIR ALAFENAMIDE TABLETS. reported. Discontinue dolutegravir, emtricitabine and tenofovir alafenamide tablets and other suspect agents immediately if signs or DOLUTEGRAVIR, EMTRICITABINE and TENOFOVIR symptoms of hypersensitivity reactions develop. (5.2) ALAFENAMIDE tablets, for oral use • Hepatotoxicity has been reported in patients receiving a dolutegravir- containing regimen. Monitoring for hepatotoxicity is recommended. WARNING: POST-TREATMENT ACUTE EXACERBATION OF (5.3) HEPATITIS B • Embryo-fetal toxicity may occur when used at the time of conception and in early pregnancy. An alternative treatment to dolutegravir, See full prescribing information for complete boxed warning. emtricitabine and tenofovir alafenamide tablets should be considered at the time of conception through the first trimester of pregnancy due to the Severe acute exacerbations of hepatitis B virus (HBV) have been reported risk of neural tube defects. Counsel adolescents and adults of in HBV-infected patients who have discontinued products containing childbearing potential to use effective contraception. -

MSF Comment on Raltegravir
International Office Rue de Lausanne 78 CP 116 1211 Geneva 21 Switzerland Phone: +41 (0)22 8498400 Fax: +41 (0) 22 849 84 04 www.msf.org Raltegravir (granules for oral suspension, 100 mg/packet) MSF supports the inclusion of raltegravir granules for oral suspension, 100 mg/packet, as a new formulation in both the WHO Essential Medicines List and the WHO Essential Medicines List for Children, for treatment of HIV among infants and children and living with HIV/AIDS. Raltegravir was the first approved drug in the pharmacological class of integrase inhibitors. In the current WHO Essential Medicines List, raltegravir is included as 400 mg tablet, 25 mg and 100 mg chewable tablet. Raltegravir granules for oral suspension was approved by the US FDA for use in neonates and young infants in December 2013 and by the EMA in June 2018. Raltegravir granules for oral suspension can be used from birth to 4 weeks of age and in young infant beginning antiretroviral treatment. In the 2018 WHO HIV Interim Guidelines “Updated Recommendations on First-Line and Second-Line Antiretroviral Regimens and Post-Exposure Prophylaxis and Recommendations on Early Infant Diagnosis of HIV”, a raltegravir-based regimen may be recommended as an alternative first-line regimen for infants and children for whom approved dolutegravir dosing is not available and a raltegravir-based regimen is recommended as the preferred first-line regimen for neonates. In the 2018 Optimal Formulary and Limited-use List for Paediatric ARVs, raltegravir-based regimens are recommended as preferred first-line treatment (with zidovudine + lamivudine) for neonates, as an alternative first-line treatment for infants (with abacavir + lamivudine), and used “for the shortest time possible, until a solid formulation of lopinavir + ritonavir or dolutegravir can be used.” Raltegravir granules for oral suspension, as preferred first-line treatment for neonates, was also added to Limit-use List for this time-limited purpose. -
Clinician's Reference Guide to Curanderismo
Clinician’s Reference Guide to Curanderismo Reference Guide Focus Scope of reference guide – to provide a basic introduc‐ tion to “curanderismo” to enhance the provider’s ability to confidently initiate conversations with patients who practice this form of traditional healing/complementary and alternative medicine (TCAM). This reference guide will 1) demystify common myths about curanderismo by clarifying what it is/is not, 2) review benefits of knowing about curanderismo to improve communication be‐ tween patient and provider; and 3) highlight some use‐ ful terminology for use with patients who practice forms of curanderismo. Goal – To improve health outcomes among Latino/as living with HIV disease, the health care provider and patient/client will collaborate on a more culturally ap‐ propriate treatment plan through a better understand‐ ing of the patient’s 1) core health beliefs and practices, 2) reasons Latino/a patients may use curanderismo and highlights of risks and 3) how the practices may inter‐ fere with conventional medical practices. Target audience – health care providers including: physi‐ cians, physician assistants, advanced practice nurses, nurses, pharmacists, oral health professionals as well as substance abuse counselors and mental health counsel‐ ors. TABLE OF CONTENTS: Introduction What Is and What Isn't Curanderismo Benefits to Knowing about Curanderismo Useful Terminology Commonly Used Herbs, Spices, & Other Items Why It Is Important to ask Introduction According to the World Health Organization, traditional medicine continues to be used in Latin America, Africa, and Asia to meet primary health care needs. In many developed countries, up to 80% of the population have used some form of traditional healing, complementary or alternative medi‐ cine ‐ TCAM (e.g. -
![1-Acetyl-17-{2-Hydroxy-3-[4-(2-Methoxyphenyl)Piperazin-1- Yl]Propyl}-17-Azapentacyclo[6.6.5.0 2,7 .0 9,14 .0 15,19 ]Nonadeca- 2,4,6,9,11,13-Hexaene-16,18-Dione](https://docslib.b-cdn.net/cover/2983/1-acetyl-17-2-hydroxy-3-4-2-methoxyphenyl-piperazin-1-yl-propyl-17-azapentacyclo-6-6-5-0-2-7-0-9-14-0-15-19-nonadeca-2-4-6-9-11-13-hexaene-16-18-dione-1512983.webp)
1-Acetyl-17-{2-Hydroxy-3-[4-(2-Methoxyphenyl)Piperazin-1- Yl]Propyl}-17-Azapentacyclo[6.6.5.0 2,7 .0 9,14 .0 15,19 ]Nonadeca- 2,4,6,9,11,13-Hexaene-16,18-Dione
Molbank 2010 , M697; doi:10.3390/M697 OPEN ACCESS molbank ISSN 1422-8599 www.mdpi.com/journal/molbank Short Note 1-Acetyl-17-{2-hydroxy-3-[4-(2-methoxyphenyl)piperazin-1- yl]propyl}-17-azapentacyclo[6.6.5.0 2,7 .0 9,14 .0 15,19 ]nonadeca- 2,4,6,9,11,13-hexaene-16,18-dione Magdalena Pakosi ńska-Parys *, Jerzy Kossakowski and Marta Struga Chair and Department of Medical Chemistry, 1 st Faculty of Medicine, Medical University of Warsaw, 3 Oczki Street, 02-007 Warsaw, Poland * Author to whom correspondence should be addressed; E-Mail: [email protected] Received: 5 August 2010 / Accepted: 14 September 2010 / Published: 17 September 2010 Abstract: The title compound was synthesized by condensation of an oxiran imide derivative with an appropriate amine and its IR, 1H NMR, 13 C NMR and mass spectroscopic data are reported. The synthesized compound was evaluated for its cytotoxicity and anti-HIV-1 activity in MT-4 cells. Keywords: 1-acetyl-17-{2-hydroxy-3-[4-(2-methoxyphenyl)piperazin-1-yl]propyl}-17- azapentacyclo[6.6.5.0 2,7 .0 9,14 .0 15,19 ]nonadeca-2,4,6,9,11,13-hexaene-16,18-dione; cytotoxicity Introduction Currently available drugs for the treatment of HIV infections are based on combination of two types of anti-HIV-1 agents: nucleoside reverse transcriptase inhibitors (RTIs) and protease inhibitors [1]. The RTIs can be divided into nucleoside (NI) and non-nucleoside RT inhibitors (NNRTI). Several non-nucleoside inhibitors have been described, including nevirapine, thiobenzimidazolone (TIBO) derivatives, pyridinone derivatives and the bis(heteroaryl)piperazines (BHAPs), such as delavirdine and atevirdine [2]. -

ISENTRESS (Raltegravir) for Oral Suspension ------CONTRAINDICATIONS ------Initial U.S
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use --------------------- DOSAGE FORMS AND STRENGTHS --------------------- ISENTRESS safely and effectively. See full prescribing information Film-Coated Tablets: 400 mg (3). for ISENTRESS. Film-Coated Tablets: 600 mg (3). ISENTRESS® (raltegravir) film-coated tablets, for oral use Chewable Tablets: 100 mg scored and 25 mg (3). ® ISENTRESS HD (raltegravir) film-coated tablets, for oral use For Oral Suspension: Single-use packet of 100 mg (3). ISENTRESS® (raltegravir) chewable tablets, for oral use ® ISENTRESS (raltegravir) for oral suspension ------------------------------- CONTRAINDICATIONS ------------------------------- Initial U.S. Approval: 2007 None (4). ----------------------------INDICATIONS AND USAGE ---------------------------- ----------------------- WARNINGS AND PRECAUTIONS ----------------------- Adult Patients: Severe, potentially life-threatening and fatal skin reactions have been ISENTRESS and ISENTRESS HD are human immunodeficiency virus reported. This includes cases of Stevens-Johnson syndrome, integrase strand transfer inhibitors (HIV-1 INSTI) indicated in hypersensitivity reaction and toxic epidermal necrolysis. Immediately combination with other antiretroviral agents for the treatment of HIV-1 discontinue treatment with ISENTRESS or ISENTRESS HD and infection in adult patients (1). other suspect agents if severe hypersensitivity, severe rash, or rash Pediatric Patients: with systemic symptoms or liver aminotransferase