First Metatarsophalangeal Joint Fusion with Minimal Fixation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ankylosing Spondylitis
Page 1 of 4 Ankylosing Spondylitis Ankylosing spondylitis (AS) is a form of arthritis. It mainly affects the lower back. Other joints and other parts of the body are sometimes affected. Treatment includes regular exercise and anti-inflammatory drugs. The severity of AS varies from mild to severe. It is mild or moderate in most cases. What is ankylosing spondylitis? Spondylitis means inflammation of the spine. Ankylosing is a word that describes bones that tend to join together (fuse) across a joint. In ankylosing spondylitis (AS), the discs and ligaments of the lower spine become inflamed. The discs and ligaments are the strong tissues that connect the spinal bones (vertebrae) together. The joints between the lower spine and the pelvis (the sacro-iliac joints), and the small facet joints between the vertebrae are also commonly affected. Inflammation around the lower spine that persists long-term can cause scarring. This may, over time, cause some of the vertebrae in the spine to fuse together. In some cases, inflammation occurs in other joints and in other parts of the body outside of the spine (detailed below). Who gets ankylosing spondylitis? AS usually develops in teenagers or young adults. It rarely first develops after the age of 40. It is three times more common in men than women. There may be a family history with two or more members of a family being affected. About 1 in 1000 people in the UK have AS. What causes ankylosing spondylitis? The cause of AS is not known. There is a strong genetic (hereditary) part. Something may 'trigger' AS to develop in people who have an inherited tendency to have it. -
Bunion Basics
WHAT IS A BUNION? A bunion is a “bump” on the outer edge of your big toe and forms when the bone or tissue at the big toe joint moves out of place. You may have a bunion if this area of your foot is red, swollen, or painful. BUNION BASICS WHY DO I HAVE A BUNION? Blame your genetics first, but your footwear next! Bunions tend to run in families, specifically among those who have the foot type prone to developing a bunion. If you have flat feet, low arches, arthritis, or inflammatory joint disease, you can develop a bunion. Footwear choices play a role too! Wearing shoes that are too tight or cause the toes to be squeezed together, like many stylish peep-or pointed-toe shoes, aggravates a bunion-prone foot. WHAT CAN I DO ABOUT MY BUNION? If you’ve noticed the beginnings of a bunion, avoid high heels over two inches with tight toe-boxes. You can also use a bunion pad inside of your shoes to provide some protection. WHO CAN HELP WITH MY BUNION? Today’s podiatrist is the bunion expert and can help you Beat Bunion Blues! There are several treatment options available, including the following: – Padding and taping to minimize pain and keep the foot in a normal position, reducing stress and pain. – Anti-inflammatory medications and cortisone injections can be prescribed to ease acute pain and inflammation. – Physical therapy can relieve bunion pain, and ultrasound therapy is a technique for treating bunions and their associated soft tissue involvement. – Orthotics or shoe inserts may be useful in controlling foot function to prevent worsening of a bunion. -

ICD-10 Diagnoses on Router
L ARTHRITIS R L HAND R L ANKLE R L FRACTURES R OSTEOARTHRITIS: PRIMARY, 2°, POST TRAUMA, POST _____ CONTUSION ACHILLES TEN DYSFUNCTION/TENDINITIS/RUPTURE FLXR TEN CLAVICLE: STERNAL END, SHAFT, ACROMIAL END CRYSTALLINE ARTHRITIS: GOUT: IDIOPATHIC, LEAD, CRUSH INJURY AMPUTATION TRAUMATIC LEVEL SCAPULA: ACROMION, BODY, CORACOID, GLENOID DRUG, RENAL, OTHER DUPUYTREN’S CONTUSION PROXIMAL HUMERUS: SURGICAL NECK 2 PART 3 PART 4 PART CRYSTALLINE ARTHRITIS: PSEUDOGOUT: HYDROXY LACERATION: DESCRIBE STRUCTURE CRUSH INJURY PROXIMAL HUMERUS: GREATER TUBEROSITY, LESSER TUBEROSITY DEP DIS, CHONDROCALCINOSIS LIGAMENT DISORDERS EFFUSION HUMERAL SHAFT INFLAMMATORY: RA: SEROPOSITIVE, SERONEGATIVE, JUVENILE OSTEOARTHRITIS PRIMARY/SECONDARY TYPE _____ LOOSE BODY HUMERUS DISTAL: SUPRACONDYLAR INTERCONDYLAR REACTIVE: SECONDARY TO: INFECTION ELSEWHERE, EXTENSION OR NONE INTESTINAL BYPASS, POST DYSENTERIC, POST IMMUNIZATION PAIN OCD TALUS HUMERUS DISTAL: TRANSCONDYLAR NEUROPATHIC CHARCOT SPRAIN HAND: JOINT? OSTEOARTHRITIS PRIMARY/SECONDARY TYPE _____ HUMERUS DISTAL: EPICONDYLE LATERAL OR MEDIAL AVULSION INFECT: PYOGENIC: STAPH, STREP, PNEUMO, OTHER BACT TENDON RUPTURES: EXTENSOR OR FLEXOR PAIN HUMERUS DISTAL: CONDYLE MEDIAL OR LATERAL INFECTIOUS: NONPYOGENIC: LYME, GONOCOCCAL, TB TENOSYNOVITIS SPRAIN, ANKLE, CALCANEOFIBULAR ELBOW: RADIUS: HEAD NECK OSTEONECROSIS: IDIOPATHIC, DRUG INDUCED, SPRAIN, ANKLE, DELTOID POST TRAUMATIC, OTHER CAUSE SPRAIN, ANKLE, TIB-FIB LIGAMENT (HIGH ANKLE) ELBOW: OLECRANON WITH OR WITHOUT INTRA ARTICULAR EXTENSION SUBLUXATION OF ANKLE, -

Clinical and Radiographic Features of Spondylitic Hip Disease J
Ann Rheum Dis: first published as 10.1136/ard.38.4.332 on 1 August 1979. Downloaded from Annals of the Rheumatic Diseases, 1979, 38, 332-336 Clinical and radiographic features of spondylitic hip disease J. S. MARKS AND K. HARDINGE From the Rheumatology Unit and the Centre for Hip Surgery, Wrightington Hospital, Wigan, Lancs SUMMARY The clinical and radiographic features of hip disease in 76 patients with definite anky- losing spondylitis have been studied. Symptomatic hip involvement occurred late in the course of the disease, with a mean delay after the onset of 12 years in males and 7 years in females. Patients with disease onset before the age of 20 developed hip symptoms at an earlier stage. Associated diseases included uveitis (13 %), colitis (4 %), and psoriasis (4 %). Bilateral concentric loss of hip joint space with a relatively undeformed femoral head was the commonest radiological change (61 %). Localised loss ofjoint space at the upper pole (16 %) was associated with femoral head destruction and a greater degree of osteophytosis, suggesting coincidental or secondary osteoarthrosis. Bony ankylosis of the hips (10%) was present only in women, and the absence of osteophytes, cysts, and bone lesions of the iliac crests and ischial rami suggests that it is a distinct radiographic manifestation of female ankylosing spondylitis. copyright. Ankylosing spondylitis characteristically affects Clinical details obtained from the medical records the sacroiliac joints and the spine, but peripheral included age at onset of disease, site(s) of initial joint involvement occurs in at least 50% of patients symptoms, age at initial hip symptoms, associated during the course of their disease (Polley and diseases, previous medical and surgical treatment, Slocumb, 1947; Wilkinson and Bywaters, 1958; and details of hip surgery during admission. -

Hallux Valgus
MedicalContinuing Education Building Your FOOTWEAR PRACTICE Objectives 1) To be able to identify and evaluate the hallux abductovalgus deformity and associated pedal conditions 2) To know the current theory of etiology and pathomechanics of hallux valgus. 3) To know the results of recent Hallux Valgus empirical studies of the manage- ment of hallux valgus. Assessment and 4) To be aware of the role of conservative management, faulty footwear in the develop- ment of hallux valgus deformity. and the role of faulty footwear. 5) To know the pedorthic man- agement of hallux valgus and to be cognizant of the 10 rules for proper shoe fit. 6) To be familiar with all aspects of non-surgical management of hallux valgus and associated de- formities. Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Continu- ing Medical Education by the Council on Podiatric Medical Education. You may enroll: 1) on a per issue basis (at $15 per topic) or 2) per year, for the special introductory rate of $99 (you save $51). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the near future, you may be able to submit via the Internet. If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned credits. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. -

Adult Still's Disease
44 y/o male who reports severe knee pain with daily fevers and rash. High ESR, CRP add negative RF and ANA on labs. Edward Gillis, DO ? Adult Still’s Disease Frontal view of the hands shows severe radiocarpal and intercarpal joint space narrowing without significant bony productive changes. Joint space narrowing also present at the CMC, MCP and PIP joint spaces. Diffuse osteopenia is also evident. Spot views of the hands after Tc99m-MDP injection correlate with radiographs, showing significantly increased radiotracer uptake in the wrists, CMC, PIP, and to a lesser extent, the DIP joints bilaterally. Tc99m-MDP bone scan shows increased uptake in the right greater than left shoulders, as well as bilaterally symmetric increased radiotracer uptake in the elbows, hands, knees, ankles, and first MTP joints. Note the absence of radiotracer uptake in the hips. Patient had bilateral total hip arthroplasties. Not clearly evident are bilateral shoulder hemiarthroplasties. The increased periprosthetic uptake could signify prosthesis loosening. Adult Stills Disease Imaging Features • Radiographs – Distinctive pattern of diffuse radiocarpal, intercarpal, and carpometacarpal joint space narrowing without productive bony changes. Osseous ankylosis in the wrists common late in the disease. – Joint space narrowing is uniform – May see bony erosions. • Tc99m-MDP Bone Scan – Bilaterally symmetric increased uptake in the small and large joints of the axial and appendicular skeleton. Adult Still’s Disease General Features • Rare systemic inflammatory disease of unknown etiology • 75% have onset between 16 and 35 years • No gender, race, or ethnic predominance • Considered adult continuum of JIA • Triad of high spiking daily fevers with a skin rash and polyarthralgia • Prodromal sore throat is common • Negative RF and ANA Adult Still’s Disease General Features • Most commonly involved joint is the knee • Wrist involved in 74% of cases • In the hands, interphalangeal joints are more commonly affected than the MCP joints. -

Arthritis in Myasthenia Gravis
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.38.11.1048 on 1 November 1975. Downloaded from Journal ofNeurology, Neurosurgery, and Psychiatry, 1975, 38, 1048-1055 Arthritis in myasthenia gravis J. A. AARLI1, E.-J. MILDE, AND S. THUNOLD From the Departments of Neurology and Pathology, School of Medicine, University of Bergen, and the Rheumatic Disease Unit, The Deaconesses' Hospital, Bergen, Norway SYNOPSIS Seven patients with myasthenia gravis developed clinical signs of arthropathy. In two patients, the symptoms were due to a deforming rheumatoid arthritis and the myasthenic symptoms appeared as a transitory phase during the course of the disease. Muscle antibodies of IgG class were demonstrated with sera from both patients. Autoreactivity between muscle antibodies and rheuma- toid factor was detected in one patient. Both patients died from sudden cardiac failure. Necropsy was performed in one and revealed a spotty myocardial necrosis. One patient had juvenile rheumatoid arthritis. Two patients had mild articular symptoms with indices of multivisceral disease and sero- logical findings indicating a systemic lupus erythematosus. One patient had classical ankylosing spondylitis, and one, unspecified arthropathy. guest. Protected by copyright. The concept of myasthenia gravis as a pure cate a clinical overlap (Oosterhuis and de Haas, disorder of the neuromuscular transmission has 1968). The aim of the present paper is a re- probably been an obstacle to the full delineation appraisal ofthe relationship between myasthenia of the clinical picture of this disease. Thus, care- gravis and arthritis. Seven patients are described ful clinical examination has revealed a series of and the data compared with relevant literature. -

Bunion Surgery - Orthoinfo - AAOS 6/10/12 3:20 PM
Bunion Surgery - OrthoInfo - AAOS 6/10/12 3:20 PM Copyright 2001 American Academy of Orthopaedic Surgeons Bunion Surgery Most bunions can be treated without surgery. But when nonsurgical treatments are not enough, surgery can relieve your pain, correct any related foot deformity, and help you resume your normal activities. An orthopaedic surgeon can help you decide if surgery is the best option for you. Whether you've just begun exploring treatment for bunions or have already decided with your orthopaedic surgeon to have surgery, this booklet will help you understand more about this valuable procedure. What Is A Bunion? A bunion is one problem that can develop due to hallux valgus, a foot deformity. The term "hallux valgus" is Latin and means a turning outward (valgus) of the big toe (hallux). The bone which joins the big toe, the first metatarsal, becomes prominent on the inner border of the foot. This bump is the bunion and is made up of bone and soft tissue. What Causes Bunions? By far the most common cause of bunions is the prolonged wearing of poorly fitting shoes, usually shoes with a narrow, pointed toe box that squeezes the toes into an unnatural position. Bunions also may be caused by arthritis or polio. Heredity often plays a role in bunion formation. But these causes account for only a small percentage of bunions. A study by the American Orthopaedic Foot and Ankle Society found that 88 percent of women in the U.S. wear shoes that are too small and 55 percent have bunions. Not surprisingly, bunions are nine times more common in women than men. -
Surgical Challenges in Complex Primary Total Hip Arthroplasty
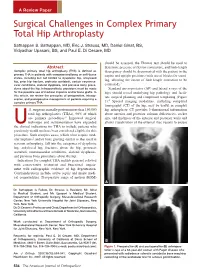
A Review Paper Surgical Challenges in Complex Primary Total Hip Arthroplasty Sathappan S. Sathappan, MD, Eric J. Strauss, MD, Daniel Ginat, BS, Vidyadhar Upasani, BS, and Paul E. Di Cesare, MD should be assessed, the Thomas test should be used to Abstract determine presence of flexion contracture, and limb-length Complex primary total hip arthroplasty (THA) is defined as discrepancy should be documented with the patient in the primary THA in patients with compromised bony or soft-tissue supine and upright positions (with use of blocks for stand- states, including but not limited to dysplastic hip, ankylosed hip, prior hip fracture, protrusio acetabuli, certain neuromus- ing, allowing the extent of limb-length correction to be 3 cular conditions, skeletal dysplasia, and previous bony proce- estimated). dures about the hip. Intraoperatively, provisions must be made Standard anteroposterior (AP) and lateral x-rays of the for the possible use of modular implants and/or bone grafts. In hips should reveal underlying hip pathology and facili- this article, we review the principles of preoperative, intraop- tate surgical planning and component templating (Figure erative, and postoperative management of patients requiring a 4 complex primary THA. 1). Special imaging modalities, including computed tomography (CT) of the hip, may be useful in complex .S. surgeons annually perform more than 150,000 hip arthroplasty. CT provides 3-dimensional information total hip arthroplasties (THAs), 90% of which about anterior and posterior column deficiencies, socket are primary procedures.1 Improved surgical size, and thickness of the anterior and posterior walls and technique and instrumentation have expanded allows visualization of the external iliac vessels to ensure Uthe clinical indications for THA to include patients who previously would not have been considered eligible for this procedure. -

Observed Changes in Radiographic Measurements of The
The Journal of Foot & Ankle Surgery xxx (2014) 1–4 Contents lists available at ScienceDirect The Journal of Foot & Ankle Surgery journal homepage: www.jfas.org Original Research Observed Changes in Radiographic Measurements of the First Ray after Frontal and Transverse Plane Rotation of the Hallux: Does the Hallux Drive the Metatarsal in a Bunion Deformity? Paul Dayton, DPM, MS, FACFAS 1, Mindi Feilmeier, DPM, FACFAS 2, Merrell Kauwe, BS 3, Colby Holmes, BS 3, Austin McArdle, BS 3, Nathan Coleman, DPM 4 1 Foot and Ankle Division, UnityPoint Clinic, and Adjunct Professor, Des Moines University College of Podiatric Medicine and Surgery, Fort Dodge, IA 2 Assistant Professor, Des Moines University College of Podiatric Medicine and Surgery, Fort Dodge, IA 3 Podiatric Medical Student, Des Moines University College of Podiatric Medicine and Surgery, Des Moines, IA 4 Second Year Resident, Podiatric Medicine and Surgery Residency, Foot and Ankle Division, UnityPoint Health, Fort Dodge, IA article info abstract Level of Clinical Evidence: 5 It is well known that the pathologic positions of the hallux and the first metatarsal in a bunion deformity are multiplanar. It is not universally understood whether the pathologic changes in the hallux or first metatarsal Keywords: etiology drive the deformity. We have observed that frontal plane rotation of the hallux can result in concurrent po- fi fresh frozen cadaver sitional changes proximally in the rst metatarsal in hallux abducto valgus. In the present study, we observed hallux abducto valgus the changes in common radiographic measurements used to evaluate a bunion deformity in 5 fresh frozen metatarsus primus adducto valgus cadaveric limbs. -

The Role of Arthroscopic Adhesiolysis in the Treatment of the Arthrofibrosis and the Partial Ankylosis of the Knee
Acta Orthop Traumatol Turc 28, 379-383 , 1994 The role of arthroscopic adhesiolysis in the treatment of the arthrofibrosis and the partial ankylosis of the knee Metin Lütfü Saydartl), Ethem Gür1l ), Vecihi Kırdemir1 l ), Ali Saib Engin(1) Dizin parsiyel ankilozu ve artrofibrozisinin tedavisinde artroskopik adezyolizisin rolü Travma, klf/k yada distal femur cerrahi girişim ardından gelişen diz hareketi kısıtlanan 23 hastanın 27 dizi, artroskopik kontrol altında , perkutan adezyon releasei ile tedavi edildi. Diz hareketlerini kısıtlayan neden ile artroskopik adezyolizis arasındaki dönem 4 ile 24 ay (ortalama 7 ay) arasında değişiyordu. Ortalama preope ratif diz hareketi 43°, ortalama postop diz hareketi IIS°'ydi. Ortalama postoperatif hareket kaybı 17"'ydi. Takip sonunda ortalama hareket kazancı SS°'ydi. Anahtar kelimeler: Artroskopi, artrofibrozis, adezyolizis, diz, ankiloz The role of arthroscopic adhesiolysis in the treatment of the arthrofibrosis and the partial ankylosis of theknee The 27 knees of 23 patients with limited range of motion that developed after trauma, fractures or open surgical procedures of the distal femur were treated by the percutaneous release of the adhesions under art hroscopic control. The inteNal between the cause of the limited ROM and the arthroscopic adhesiolysis ran ged from 4 months to 24 months (mean: 7 months). The average preoperative ROM was 43° and the average postoperative ROM was 115°. The average loss from the postoperative ROM was 1r. At the fol/ow-up, the average final gain of ROM was 55°. Keywords: Arthroscopy, arthrofibrosis, adhesiolysis, knee, ankylosis. The pathogenesis of arthrofibrosis is not a single Another subgroup of the post-traumatic arthrofib process but there are multiple factors that play roles rosis is the Infrapatellar Contracture Syndrome in this procedure. -

First Metatarsophalangeal Joint Replacement with Total Arthroplasty in the Surgical Treatment of the Hallux Rigidus R
Acta Biomed 2014; Vol. 85, Supplement 2: 113-117 © Mattioli 1885 Original article First metatarsophalangeal joint replacement with total arthroplasty in the surgical treatment of the hallux rigidus R. Valentini, G. De Fabrizio, G. Piovan Clinica Ortopedica e Traumatologica, Università degli Studi di Trieste, Azienda Ospedaliero-Universitaria “Ospedali Riuniti” di Trieste Abstract. The hallux rigidus, especially in advanced stage, has always been a challenge as regards the surgical treatment. Over the years there have been various surgical techniques proposed with the aim of relieving pain, correcting deformity and maintain a certain degree of movement. For some years we have addressed the prob- lem with the replacement metatarsophalangeal joint arthroplasty with Reflexion system. As far as our experi- ence we have operated and monitored 25 patients (18 females and 7 males) of mean age 58.1 years, operated with this technique from June 2008 to June 2011. It reached an average ROM of 72° (extension and flexion 45° and 27°) with a good functional recovery in 8 patients, and this articulation was good (50° - 40°) in 12 patients and moderate in 5 with a articular range from 40°- 30°. The clinical results, according to our experience, appear to be favorable, as even patient satisfaction is complete. (www.actabiomedica.it) Key words: hallux rigidus, metatarsophalangeal, arthroprosthesis Introduction The pathology of stiff big toe has ranked about Regnauld classification (5) in three stages, so that the Degenerative disease of the first metatarsal- I stage is characterized by wear of the joint with mini- phalangeal articulation, the so-called “Hallux rigi- mal osteophytes reaction, the II stage is reached when dus”, especially in advanced phase, has always been the joint line is further reduced, the articular surfaces a sort of challenge as a surgical treatment.