OA Guide to High Altitude Acclimatization & Illnesses
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Fog and Low Clouds As Troublemakers During Wildfi Res
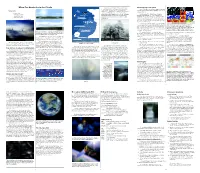
When Our Heads Are in the Clouds Sometimes water droplets do not freeze in below- Detecting fog from space Up to 60,000 ft (18,000m) freezing temperatures. This happens if they do not have Weather satellites operated by the National Oceanic The fog comes a surface (like a dust particle or an ice crystal) upon and Atmospheric Administration (NOAA) collect data on on little cat feet. which to freeze. This below-freezing liquid water becomes clouds and storms. Cirrus Commercial Jetliner “supercooled.” Then when it touches a surface whose It sits looking (36,000 ft / 11,000m) temperature is below freezing, such as a road or sidewalk, NOAA operates two different types of satellites. over harbor and city Geostationary satellites orbit at about 22,236 miles Breitling Orbiter 3 the water will freeze instantly, making a super-slick icy on silent haunches (34,000 ft / 10,400m) Cirrocumulus coating on whatever it touches. This condition is called (35,786 kilometers) above sea level at the equator. At this and then moves on. Mount Everest (29,035 ft / 8,850m) freezing fog. altitude, the satellite makes one Earth orbit per day, just Carl Sandburg Cirrostratus as Earth rotates once per day. Thus, the satellite seems to 20,000 feet (6,000 m) Cumulonimbus hover over one spot below and keeps its “birds’-eye view” of nearly half the Earth at once. Altocumulus The other type of NOAA satellites are polar satellites. Their orbits pass over, or nearly over, the North and South Clear and cloudy regions over the U.S. -

Altitude Sickness in Nepal Is About 1 in 30,000 Trekkers, Or 2-3 Deaths Per Year
Shoreland Travax Medical Summary ALTITUDE ILLNESS INTRODUCTION Altitude illness occurs when one ascends more rapidly than the body can adjust ("acclimatize") to the reduced atmospheric pressure and decreased oxygen delivery to the body's cells at the higher altitude. Factors affecting acclimatization include the altitude attained, the rate of ascent, the duration of exposure, genetic predisposition, and certain preexisting conditions. (See "Acclimatization," "Risk," and "Effect of High Altitude on Preexisting Medical Conditions.") Altitude illness is generally divided into 3 syndromes: acute mountain sickness (AMS), high altitude pulmonary edema (HAPE), and high altitude cerebral edema (HACE). See "Syndromes and Symptoms." Symptoms can range from mild to life-threatening. Although mild symptoms have been documented at relatively low altitudes of 1,200- 1,800 m (3,900-5,900 ft), serious syndromes are rarely seen below 2,500-3,000 m (8,200-9,800 ft). While death can occur from the more severe forms of altitude illness, most symptoms can be prevented or minimized by proper acclimatization and/or preventive medications. Risk and prevention strategies vary depending on the type of travel planned: travel to typical tourist destinations at relatively moderate heights or trekking in extreme high altitude situations. See "Risk of Altitude Illness" and "Prevention." ACCLIMATIZATION Acclimatization is a built-in adjustment mechanism that can optimize performance at higher altitudes. If a person ascends more rapidly than the body can adjust, symptoms occur that are referred to as altitude illness. Acclimatization seems to be determined by factors that are not known but may possibly be genetic. Some people adjust very easily to high altitude, while others cannot go above relatively moderate heights of 3,000 m (9,800 ft) without experiencing symptoms. -

Aviation Glossary
AVIATION GLOSSARY 100-hour inspection – A complete inspection of an aircraft operated for hire required after every 100 hours of operation. It is identical to an annual inspection but may be performed by any certified Airframe and Powerplant mechanic. Absolute altitude – The vertical distance of an aircraft above the terrain. AD - See Airworthiness Directive. ADC – See Air Data Computer. ADF - See Automatic Direction Finder. Adverse yaw - A flight condition in which the nose of an aircraft tends to turn away from the intended direction of turn. Aeronautical Information Manual (AIM) – A primary FAA publication whose purpose is to instruct airmen about operating in the National Airspace System of the U.S. A/FD – See Airport/Facility Directory. AHRS – See Attitude Heading Reference System. Ailerons – A primary flight control surface mounted on the trailing edge of an airplane wing, near the tip. AIM – See Aeronautical Information Manual. Air data computer (ADC) – The system that receives and processes pitot pressure, static pressure, and temperature to present precise information in the cockpit such as altitude, indicated airspeed, true airspeed, vertical speed, wind direction and velocity, and air temperature. Airfoil – Any surface designed to obtain a useful reaction, or lift, from air passing over it. Airmen’s Meteorological Information (AIRMET) - Issued to advise pilots of significant weather, but describes conditions with lower intensities than SIGMETs. AIRMET – See Airmen’s Meteorological Information. Airport/Facility Directory (A/FD) – An FAA publication containing information on all airports, seaplane bases and heliports open to the public as well as communications data, navigational facilities and some procedures and special notices. -

Solar Energy Generation Model for High Altitude Long Endurance Platforms
Solar Energy Generation Model for High Altitude Long Endurance Platforms Mathilde Brizon∗ KTH - Royal Institute of Technology, Stockholm, Sweden For designing and evaluating new concepts for HALE platforms, the energy provided by solar cells is a key factor. The purpose of this thesis is to model the electrical power which can be harnessed by such a platform along any flight trajectory for different aircraft designs. At first, a model of the solar irradiance received at high altitude will be performed using the solar irradiance models already existing for ground level applications as a basis. A calculation of the efficiency of the energy generation will be performed taking into account each solar panel's position as well as shadows casted by the aircraft's structure. The evaluated set of trajectories allows a stationary positioning of a hale platform with varying wind conditions, time of day and latitude for an exemplary aircraft configuration. The qualitative effects of specific parameter changes on the harnessed solar energy is discussed as well as the fidelity of the energy generation model results. Nomenclature δ Solar declination ({) EQE Quantum efficiency (%) η Efficiency (%) hg Altitude of the aircraft (m) ◦ Γ Day angle ( ) hO3 Height of max ozone concentration(m) ◦ −2 −1 λg Longitude aircraft ( ) Id Direct irradiance (W:m .µm ) ◦ −2 −1 ! Hour angle ( ) Is Diffuse irradiance (W:m .µm ) ◦ −2 −1 φg Latitude of the aircraft ( ) Itot Total irradiance (W:m .µm ) ◦ −1 ◦ τ Rayleigh optical depth ({) kPmax;T Temperature Coefficient (%: C ) 2 A Solar cell -

1 the Atmosphere of Pluto As Observed by New Horizons G
The Atmosphere of Pluto as Observed by New Horizons G. Randall Gladstone,1,2* S. Alan Stern,3 Kimberly Ennico,4 Catherine B. Olkin,3 Harold A. Weaver,5 Leslie A. Young,3 Michael E. Summers,6 Darrell F. Strobel,7 David P. Hinson,8 Joshua A. Kammer,3 Alex H. Parker,3 Andrew J. Steffl,3 Ivan R. Linscott,9 Joel Wm. Parker,3 Andrew F. Cheng,5 David C. Slater,1† Maarten H. Versteeg,1 Thomas K. Greathouse,1 Kurt D. Retherford,1,2 Henry Throop,7 Nathaniel J. Cunningham,10 William W. Woods,9 Kelsi N. Singer,3 Constantine C. C. Tsang,3 Rebecca Schindhelm,3 Carey M. Lisse,5 Michael L. Wong,11 Yuk L. Yung,11 Xun Zhu,5 Werner Curdt,12 Panayotis Lavvas,13 Eliot F. Young,3 G. Leonard Tyler,9 and the New Horizons Science Team 1Southwest Research Institute, San Antonio, TX 78238, USA 2University of Texas at San Antonio, San Antonio, TX 78249, USA 3Southwest Research Institute, Boulder, CO 80302, USA 4National Aeronautics and Space Administration, Ames Research Center, Space Science Division, Moffett Field, CA 94035, USA 5The Johns Hopkins University Applied Physics Laboratory, Laurel, MD 20723, USA 6George Mason University, Fairfax, VA 22030, USA 7The Johns Hopkins University, Baltimore, MD 21218, USA 8Search for Extraterrestrial Intelligence Institute, Mountain View, CA 94043, USA 9Stanford University, Stanford, CA 94305, USA 10Nebraska Wesleyan University, Lincoln, NE 68504 11California Institute of Technology, Pasadena, CA 91125, USA 12Max-Planck-Institut für Sonnensystemforschung, 37191 Katlenburg-Lindau, Germany 13Groupe de Spectroscopie Moléculaire et Atmosphérique, Université Reims Champagne-Ardenne, 51687 Reims, France *To whom correspondence should be addressed. -

Deadly High Altitude Pulmonary Disorders: Acute Mountain Sickness
Research Article Int J Pul & Res Sci Volume 1 Issue 1 - April 2016 Copyright © All rights are reserved by Michael Obrowski DOI : 10.19080/IJOPRS.2016.01.555553 Deadly High Altitude Pulmonary Disorders: Acute Mountain Sickness (AMS); High Altitude Pulmonary Edema (HAPE) and High Altitude Cerebral Edema (HACE): A Clinical Review Michael Obrowski1* and Stephanie Obrowski2 1Doctor of Medicine (M.D. – 2000); Assistant Professor of Anatomy; CEO, Chief Physician and Surgeon of Wilderness Physicians, European Union 2Doctor of Medicine (M.D. – 2019); Medical University of Łódź; President of Wilderness Physicians, European Union Submission: January 26, 2016; Published: April 15, 2016 *Corresponding author: Michael Obrowski, M.D., Doctor of Medicine (M.D. – 2000); Assistant Professor of Anatomy; CEO, Chief Physician and Surgeon of Wilderness Physicians, European Union, 43C Żeligowskiego Street, #45, Łódź, Poland 90-644, Email: Abstract Acute Mountain Sickness (AMS); High Altitude Pulmonary Edema (HAPE) and High Altitude Cerebral Edema (HACE). These three disorders, withMountain relatively Sickness, unimportant also smallcalled variationsHigh Altitude seen Sickness, in some isPulmonology specifically aTextbooks, triad of different because disorders, these are inso orderserious, of increasingthey are all seriousness: potentially deadly pulmonary disorders and we will discuss these three major, deadly disorders. Each one, starting with AMS, can progress rapidly to HAPE and then HACE. The two authors of this article have over half a century of high altitude mountaineering experience. They have also alsohad anddisaster still domedicine. have, for Since the lastspring twenty is rapidly years, approaching an NGO, Non-Profit and many Medical “weekend Organization backpackers” (Wilderness will start Physicians going into www.wildernessphysicians. -

Comparison of Health and Performance Risk for Accelerated Mars Mission Scenarios
NASA/TM-20210009779 Comparison of Health and Performance Risk for Accelerated Mars Mission Scenarios Erik Antonsen MD, PhD Baylor College of Medicine NASA Johnson Space Center, Houston, TX Mary Van Baalen, PhD; NASA Johnson Space Center, Houston, TX Integrated Medical Model Team Space Radiation Analysis Group Binaifer Kadwa, MS Lori Chappell, MS NASA Johnson Space Center, Houston, TX KBR NASA Johnson Space Center, Houston, TX Lynn Boley, RN, MS KBR Edward Semones, MS NASA Johnson Space Center, Houston, TX NASA Johnson Space Center, Houston, TX John Arellano, PhD Space Radiation Element MEI Technologies NASA Johnson Space Center, Houston, TX S. Robin Elgart, PhD University of Houston Eric Kerstman, MD NASA Johnson Space Center, Houston, TX University of Texas Medical Branch NASA Johnson Space Center, Houston, TX National Aeronautics and Space Administration Lyndon B. Johnson Space Center Houston, Texas 77058 February 2021 NASA STI Program…in Profile Since its founding, NASA has been dedicated to the CONFERENCE PUBLICATION. advancement of aeronautics and space science. The Collected papers from scientific and NASA scientific and technical information (STI) technical conferences, symposia, seminars program plays a key part in helping NASA or other meetings sponsored or co- maintain this important role. sponsored by NASA. The NASA STI program operates under the auspices of the Agency Chief Information Officer. SPECIAL PUBLICATION. Scientific, It collects, organizes, provides for archiving, and technical, or historical information from disseminates NASA’s STI. The NASA STI NASA programs, projects, and missions, program provides access to the NTRS Registered often concerned with subjects having and its public interface, the NASA Technical substantial public interest. -

Altitude Sickness
Altitude Sickness Team River Runner hosted their National Conference and Swiftwater Rescue Training out West this year. It was a great place to visit and our hosts: TRR Boise and Pilgrim’s Cove couldn’t have been more accommodating. Several participants came from low lying areas – near sea level including myself. Some attendees and myself as well experienced: • Headache • Loss of normal appetite • Nausea • Insomnia • General Fatigue We each came up with different conclusions on why we were experiencing these symptoms, in my case possible motion sickness, dehydration, etc. None of us thought Altitude Sickness may be contributing to our malaise. It wasn’t till after the conference when several of us that live near sea level and were experiencing the above symptoms figured out that a mild form of Altitude Sickness was a highly probably diagnosis. Part of my job is Risk Management so it’s well worth considering this possibility and precautions we should consider whenever traveling to locales that can trigger these issues. Most whom take Wilderness First Aid courses are taught the magic cutoff: 2400m or roughly 8,000’ (Red Cross says 7,000’). McCall Idaho is roughly 5,000’, roughly a mile high. It turns out that the 8,000’ cutoff is actually for: • HACE – High Altitude Cerebral Edema • HAPE – High Altitude Pulmonary Edema High Altitude per Wilderness EMS is actually from 1,500m to 3,500m, or starting at 4,921’ (roughly the altitude where we were staying at). A good guide is the Lake Louise Acute Mountain Sickness (AMS) Scoring System (LLS). -

Altitude Sickness Fact Sheet
Altitude Sickness Fact Sheet At high elevation, you may experience a potentially life threatening condition called altitude sickness. This is exacerbated if you ascend in elevation quickly. At 8,000 feet, there is only ~75% of the available oxygen at sea level. Oxygen decreases ~3% with each 1000 feet in elevation. Altitude sickness is caused by the body not being able to get enough oxygen. There are three types of altitude sickness: Acute Mountain Sickness, High Altitude Pulmonary Edema, and High Altitude Cerebral Edema. SYMPTOMS Acute Mountain Sickness • Lack of appetite, nausea, or vomiting • Fatigue • Dizziness • Insomnia • Shortness of breath upon exertion • Nosebleed • Persistent rapid pulse • Swelling of hands, feet, and/or face High Altitude Pulmonary Edema (HAPE) • Symptoms similar to bronchitis • Persistent dry cough • Fever • Shortness of breath even at rest High Altitude Cerebral Edema (HACE) • Headache that does not respond to medication • Difficulty walking • Altered mental state (confusion, changes in alertness, disorientation, irrational behavior) • Loss of consciousness • Increased nausea • Blurred vision or retinal hemorrhage PREVENTION If your hike starts at high elevation, spend a few days adjusting to the altitude prior to any major physical exertion. It is best to sleep no more than 1,500 feet (457.2 m) higher than you did the night before. This helps the body adjust gradually to the decreased amount of oxygen. Contact your primary care physician for an evaluation prior to travelling to areas with high elevation. FIRST AID TREATMENT If you have any of these symptoms at altitude, assume that it is altitude sickness until proven otherwise. Do not ascend any further with symptoms. -

Altitude Profiles of CCN Characteristics Across the Indo-Gangetic Plain Prior to the Onset of the Indian Summer Monsoon
5 Altitude profiles of CCN characteristics across the Indo-Gangetic Plain prior to the onset of the Indian summer monsoon Venugopalan Nair Jayachandran1, Surendran Nair Suresh Babu1*, Aditya Vaishya2, Mukunda M. Gogoi1, Vijayakumar S Nair1, Sreedharan Krishnakumari Satheesh3,4, Krishnaswamy Krishna Moorthy3 10 1 Space Physics Laboratory, Vikram Sarabhai Space Centre, ISRO PO, Thiruvananthapuram, India. 2 School of Arts and Sciences, Ahmedabad University, Ahmedabad, India. 3 Centre for Atmospheric and Oceanic Sciences, Indian Institute of Science, Bangalore, India. 4 Divecha Centre for Climate Change, Indian Institute of Science, Bangalore, India. 15 *Correspondence to: Surendran Nair Suresh Babu ([email protected] / [email protected]) 1 5 Abstract Concurrent measurements of the altitude profiles of cloud condensation nuclei (CCN) concentration, as a function of supersaturation (ranging from 0.2% to 1.0%), and aerosol optical properties (scattering and absorption coefficients) were carried out aboard an instrumented aircraft across the Indo-Gangetic Plain (IGP) just prior to the onset of the Indian summer monsoon (ISM) 10 of 2016. The experiment was conducted under the aegis of the SWAAMI - RAWEX campaign. The measurements covered coastal, urban and arid environments. In general, the CCN concentration has been highest in the Central IGP, decreasing spatially from east to west above the planetary boundary layer (PBL), which is ~1.5 km for the IGP during pre-monsoon. Despite this, the CCN activation efficiency at 0.4% supersaturation has been, interestingly, the highest over the 15 eastern IGP (~72%), followed by that in the west (~61%), and has been the least over the central IGP (~24%) within the PBL. -

Backcountry Safety: Illnesses and Weather Hazards Sequoia National Forest
USDA ~ United States Department of Agriculture Backcountry Safety: Illnesses and Weather Hazards Sequoia National Forest The backcountry is beautiful place to visit, but also primitive and you will be on your own! We want you to enjoy your backcountry visit, and we want you to venture as safe as possible. These are some tips to remember. First and foremost, tell someone of your planned route and time of return before you travel into the backcountry! What to Pack Hyperthermia Sudden shifts in weather are one of the backcountry’s Caused by the body’s inability to cool in high heat greatest dangers. We recommend that you bring at the conditions. The body regulates the temperature by least a warm fleece or wool pullover, a waterproof jacket, sweating and releasing excess heat, but sometimes this an emergency blanket, a hat, sunglasses, sunscreen, lip is not enough especially when ambient air temperature balm, insect repellant, first-aid kit, pocket knife, flashlight is high and humid. The best way to cool the body is to or headlamp, waterproof matches, map, compass, a mirror stay hydrated and drink plenty of water in high and whistle for signaling if you are lost, plenty of water, temperatures conditions. If this is not enough, take a and extra food with you. break in a shaded area and remove some clothing to allow for more body cooling. There are three forms of Hiking in Variable Terrain heat-related illness that can lead to hyperthermia. Identify safe routes and local conditions. Test and use 1. Heat cramps is the mildest sign of heat-illness secure footing and never run down slopes. -

Respiratory Diseases in Relation to Changes in Atmospheric Pressure
A n n a l s o f C linical Laboratory Science, Vol. 3 , No. 2 Copyright © 1 9 7 3 , Institute for Clinical Science Respiratory Diseases in Relation to Changes in Atmospheric Pressure BROOKS H. HURD, M.D. Director of Laboratories, Grant Hospital and Clinical Associate Professor of Pathology, ■ Ohio State University, Columbus, OH 43215 ABSTRACT In this paper are reviewed the present status of respiratory diseases in relation to high and low altitude environments. High Altitude Sickness in mountaineers occurred on their initial Intkoduction exposure to high altitude without proper acclimatization time. Men living at high Mountain sickness occurs in both an altitudes have a higher total blood volume acute form and a chronic form. Only re and a greater proportion of pulmonary cently has this been studied to any degree; blood volume than that present in sea level however, the first description was by a inhabitants. Persons going to high altitudes Peruvian in 1897.8 In 1937, Hurtado de tend to develop greater blood volume in scribed a case of pulmonary edema in an the pulmonary bed. Houston had reported Indian who became acutely ill after return mountaineers who have described cases of ing home from sea level to the high alti rapid death attributed to pneumonia. This tude.7 In 1945, a 39 year old man was occurred in healthy persons who were en examined who had developed pulmonary gaged in strenuous exercise over 14,000 edema after going to a height of 11,550 feet. feet. Death in 12 to 24 hours resulted if In 1949, a 29 year old man was described the symptoms were severe and remained who died from an acute pulmonary illness untreated.