Laminopathy (LMNA)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Emery-Dreifuss Muscular Dystrophy: the Most Recognizable Laminopathy
Review paper Emery-Dreifuss muscular dystrophy: the most recognizable laminopathy Agnieszka Madej-Pilarczyk, Andrzej Kochański Neuromuscular Unit, Mossakowski Medical Research Centre, Polish Academy of Sciences, Warsaw, Poland The authors dedicate this review to Prof. Irena Hausmanowa-Petrusewicz. Folia Neuropathol 2016; 54 (1): 1-8 DOI: 10.5114/fn.2016.58910 Abstract Emery-Dreifuss muscular dystrophy (EDMD), a rare inherited disease, is characterized clinically by humero-peroneal muscle atrophy and weakness, multijoint contractures, spine rigidity and cardiac insufficiency with conduction defects. There are at least six types of EDMD known so far, of which five have been associated with mutations in genes encoding nuclear proteins. The majority of the EDMD cases described so far are of the emerinopathy (EDMD1) kind, with a recessive X-linked mode of inheritance, or else laminopathy (EDMD2), with an autosomal dominant mode of inheritance. In the work described here, the authors have sought to describe the history by which EDMD came to be distinguished as a separate entity, as well as the clinical and genetic characteristics of the disease, the pathophysiolo- gy of lamin-related muscular diseases and, finally, therapeutic issues, prevention and ethical aspects. Key words: Emery-Dreifuss muscular dystrophy, emerin, lamin A/C, laminopathy, LMNA gene. embryo nic development [14,35]. Lamin A/C plays the Introduction role of a structural integrator in a cell nucleus, ensur- Laminopathies fall within a group of rare diseas- ing the maintenance of the latter’s shape, as well as es connected with structural/functional defects of its mechanical endurance (mechanotransduction). the proteins making up the nuclear envelope (which It takes part in regulation of the cell-division cycle, is composed of inner and outer nuclear membranes). -

Three New Cases of Dilated Cardiomyopathy Caused by Mutations in LMNA Gene
Acta Myologica • 2017; XXXVI: p. 207-212 Three new cases of dilated cardiomyopathy caused by mutations in LMNA gene Larysa N. Sivitskaya1, Nina G. Danilenko1, Tatiyana G. Vaikhanskaya2, Tatsiyana V. Kurushka2 and Oleg G. Davydenko1 1 Institute of Genetics and Cytology, National Academy of Sciences of Belarus, Minsk, Belarus; 2 Republican Scientific and Practical Center of Cardiology, Minsk, Belarus Three cases of delated cardiomyopathy (DCM) with conduc- Mutations in LMNA affect lamins’ dimerization and as- tion defects (OMIM 115200), limb girdle muscular dystrophy sembly (1, 2). It apparently leads to nuclear stability loss 1B (OMIM 159001) and autosomal dominant Emery-Dreifuss and inability to perform functions in its entirety. The muscular dystrophy 2 (OMIM 181350), all associated with dif- ferent LMNA mutations are presented. Three heterozygous mutations in LMNA lead to at least 10 clinically distinct missense mutations were identified in unrelated patients – p. phenotypes, termed laminopathies, affecting different W520R (c.1558T > C), p.T528R (с.1583С > G) and p.R190P tissues including cardiac and skeletal muscle, cutane- (c.569G > C). We consider these variants as pathogenic, lead- ous, nervous and adipose tissue. There is no explicit ing to isolated DCM with conduction defects or syndromic relation between syndrome development and mutation DCM forms with limb-girdle muscular dystrophy and Emery- domain localization. A number of hot spots were de- Dreifuss muscular dystrophy. The mutations were not detected in the ethnically matched control group and publicly available scribed in LMNA, but the mutations common for lami- population databases. Their de novo occurrence led to the de- nopathies were not found. -

De Barsy Syndrome: Orthopedic Case Report and Literature Review
MOJ Orthopedics & Rheumatology De Barsy Syndrome: Orthopedic Case report and Literature Review Introduction Case Report Volume 7 Issue 5 - 2017 This condition was first described in 1968 by De Barsy who and degeneration of the elastic tissue of the cornea and skin, Jose de Jesus Guerra Jasso1*, Douglas reported a case of a patient with progeria, dwarfism, oligofrenia and since then, it is known as Barsy Syndrome or Barsy- Colmenares Bonilla2 and Loreett Ocampo Perez3 of progeroid aspect, cutis laxa, corneal opacity, intrauterine 1Pediatric Orthopedics, Hospital Regional de Alta Especialidad growthMoens-Dierckx retardation Syndrome. and severe This ismental defined retardation as the combination (although del Bajio, Mexico some will learn to speak, intelligence is less than normal) [1]. 2Pediatric Orthopedic Service, Hospital regional de alta especialidad del bajio The orthopedic manifestations are dysplasia of hip development, 3Fellow of Pediatric Orthopedics, Hospital Regional de Alta hyper laxity of severe joints, athetoid movements, scoliosis and Especialidad del Bajio, Mexico severe deformities of the foot. Epidemiology in Latin America is unknown because of its underdiagnosis and when confused *Corresponding author: Jesus Guerra Jasso, Hospital with other connective tissue pathologies (Hutchinson-Gilford Regional de Alta Especialidad del Bajio, Boulevard Milenio No. 130. Col, San Carlos la Roncha, C.P. 37660, Guanajuato, syndrome, gerodermic osteodiplasia, even Ehlers-Danlos), the Mexico, Tel: 477-267 2000; Ext-1403; life expectancy of these patients varies according to the degree of Email: penetrance and in the world literature, there are very few reports (about 50), so the diagnosis requires a challenge [2]. Received: January 13, 2017 | Published: March 21, 2017 Clinical Case and thick clamp. -

Genetic Mutations and Mechanisms in Dilated Cardiomyopathy
Genetic mutations and mechanisms in dilated cardiomyopathy Elizabeth M. McNally, … , Jessica R. Golbus, Megan J. Puckelwartz J Clin Invest. 2013;123(1):19-26. https://doi.org/10.1172/JCI62862. Review Series Genetic mutations account for a significant percentage of cardiomyopathies, which are a leading cause of congestive heart failure. In hypertrophic cardiomyopathy (HCM), cardiac output is limited by the thickened myocardium through impaired filling and outflow. Mutations in the genes encoding the thick filament components myosin heavy chain and myosin binding protein C (MYH7 and MYBPC3) together explain 75% of inherited HCMs, leading to the observation that HCM is a disease of the sarcomere. Many mutations are “private” or rare variants, often unique to families. In contrast, dilated cardiomyopathy (DCM) is far more genetically heterogeneous, with mutations in genes encoding cytoskeletal, nucleoskeletal, mitochondrial, and calcium-handling proteins. DCM is characterized by enlarged ventricular dimensions and impaired systolic and diastolic function. Private mutations account for most DCMs, with few hotspots or recurring mutations. More than 50 single genes are linked to inherited DCM, including many genes that also link to HCM. Relatively few clinical clues guide the diagnosis of inherited DCM, but emerging evidence supports the use of genetic testing to identify those patients at risk for faster disease progression, congestive heart failure, and arrhythmia. Find the latest version: https://jci.me/62862/pdf Review series Genetic mutations and mechanisms in dilated cardiomyopathy Elizabeth M. McNally, Jessica R. Golbus, and Megan J. Puckelwartz Department of Human Genetics, University of Chicago, Chicago, Illinois, USA. Genetic mutations account for a significant percentage of cardiomyopathies, which are a leading cause of conges- tive heart failure. -

Deciphering Nuclear Mechanobiology in Laminopathy
cells Review Deciphering Nuclear Mechanobiology in Laminopathy Jungwon Hah and Dong-Hwee Kim * KU-KIST Graduate School of Converging Science and Technology, Korea University, Seoul 02841, Korea; [email protected] * Correspondence: [email protected]; Tel.: +82-2-3290-4615 Received: 29 January 2019; Accepted: 5 March 2019; Published: 11 March 2019 Abstract: Extracellular mechanical stimuli are translated into biochemical signals inside the cell via mechanotransduction. The nucleus plays a critical role in mechanoregulation, which encompasses mechanosensing and mechanotransduction. The nuclear lamina underlying the inner nuclear membrane not only maintains the structural integrity, but also connects the cytoskeleton to the nuclear envelope. Lamin mutations, therefore, dysregulate the nuclear response, resulting in abnormal mechanoregulations, and ultimately, disease progression. Impaired mechanoregulations even induce malfunction in nuclear positioning, cell migration, mechanosensation, as well as differentiation. To know how to overcome laminopathies, we need to understand the mechanisms of laminopathies in a mechanobiological way. Recently, emerging studies have demonstrated the varying defects from lamin mutation in cellular homeostasis within mechanical surroundings. Therefore, this review summarizes recent findings highlighting the role of lamins, the architecture of nuclear lamina, and their disease relevance in the context of nuclear mechanobiology. We will also provide an overview of the differentiation of cellular mechanics in laminopathy. Keywords: lamin; laminopathy; cytoskeleton; nucleus 1. Introduction Mechanical stimuli are the key to controlling numerous biological processes, including proliferation, differentiation, and migration [1–3]. Integrin mediates the transduction of forces from the external microenvironment to the intracellular cytoskeleton, and the nucleo-cytoskeletal molecular connections transmit the forces to the intranuclear chromosomal organizations [4,5]. -

The Progeria Syndrome Fact Sheet
HUTCHINSON-GILFORD PROGERIA SYNDROME FREQUENTLY ASKED QUESTIONS WHAT IS PROGERIA? Hutchinson-Gilford Progeria Syndrome “Progeria” or “HGPS” is a rare, fatal genetic condition characterized by an appearance of accelerated aging in children. Its name is derived from the Greek and means "prematurely old." While there are different forms of Progeria*, the classic type is Hutchinson- Gilford Progeria Syndrome, which was named after the doctors who first described it in England: in 1886 by Dr. Jonathan Hutchinson, and in 1897 by Dr. Hastings Gilford. HOW COMMON IS PROGERIA? Progeria affects approximately 1 in 4 - 8 million newborns. It affects both sexes equally and all races. In the past 15 years, children with Progeria have been reported all over the world , including in: Algeria Cuba Ireland Peru Sweden Argentina Denmark Israel Philippines Switzerland Australia Dominican Italy Poland Turkey Austria Republic Japan Portugal United States Belgium Egypt Libya Puerto Rico Venezuela Brazil England Mexico Romania Vietnam Canada France Morocco South Africa Yugoslavia China Germany Netherlands South Korea Columbia India Pakistan Spain WHAT ARE THE FEATURES OF PROGERIA? Although they are born looking healthy, most children with Progeria begin to display many characteristics of Progeria within the first year of life. Progeria signs include growth failure, loss of body fat and hair, aged-looking skin, stiffness of joints, hip dislocation, generalized atherosclerosis, cardiovascular (heart) disease and stroke. The children have a remarkably similar appearance, despite differing ethnic backgrounds. Children with Progeria die of atherosclerosis (heart disease) at an average age of thirteen years (with a range of about 8 – 21 years). WHAT DOES PROGERIA HAVE TO DO WITH AGING? Children with Progeria are genetically predisposed to premature, progressive heart disease. -

Genetic Determinants Underlying Rare Diseases Identified Using Next-Generation Sequencing Technologies
Western University Scholarship@Western Electronic Thesis and Dissertation Repository 8-2-2018 1:30 PM Genetic determinants underlying rare diseases identified using next-generation sequencing technologies Rosettia Ho The University of Western Ontario Supervisor Hegele, Robert A. The University of Western Ontario Graduate Program in Biochemistry A thesis submitted in partial fulfillment of the equirr ements for the degree in Master of Science © Rosettia Ho 2018 Follow this and additional works at: https://ir.lib.uwo.ca/etd Part of the Medical Genetics Commons Recommended Citation Ho, Rosettia, "Genetic determinants underlying rare diseases identified using next-generation sequencing technologies" (2018). Electronic Thesis and Dissertation Repository. 5497. https://ir.lib.uwo.ca/etd/5497 This Dissertation/Thesis is brought to you for free and open access by Scholarship@Western. It has been accepted for inclusion in Electronic Thesis and Dissertation Repository by an authorized administrator of Scholarship@Western. For more information, please contact [email protected]. Abstract Rare disorders affect less than one in 2000 individuals, placing a huge burden on individuals, families and the health care system. Gene discovery is the starting point in understanding the molecular mechanisms underlying these diseases. The advent of next- generation sequencing has accelerated discovery of disease-causing genetic variants and is showing numerous benefits for research and medicine. I describe the application of next-generation sequencing, namely LipidSeq™ ‒ a targeted resequencing panel for the identification of dyslipidemia-associated variants ‒ and whole-exome sequencing, to identify genetic determinants of several rare diseases. Utilization of next-generation sequencing plus associated bioinformatics led to the discovery of disease-associated variants for 71 patients with lipodystrophy, two with early-onset obesity, and families with brachydactyly, cerebral atrophy, microcephaly-ichthyosis, and widow’s peak syndrome. -

Lamin A/C Cardiomyopathy: Implications for Treatment
Current Cardiology Reports (2019) 21:160 https://doi.org/10.1007/s11886-019-1224-7 MYOCARDIAL DISEASE (A ABBATE AND G SINAGRA, SECTION EDITORS) Lamin A/C Cardiomyopathy: Implications for Treatment Suet Nee Chen1 & Orfeo Sbaizero1,2 & Matthew R. G. Taylor1 & Luisa Mestroni1 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Purpose of Review The purpose of this review is to provide an update on lamin A/C (LMNA)-related cardiomyopathy and discuss the current recommendations and progress in the management of this disease. LMNA-related cardiomyopathy, an inherited autosomal dominant disease, is one of the most common causes of dilated cardiomyopathy and is characterized by steady progression toward heart failure and high risks of arrhythmias and sudden cardiac death. Recent Findings We discuss recent advances in the understanding of the molecular mechanisms of the disease including altered cell biomechanics, which may represent novel therapeutic targets to advance the current management approach, which relies on standard heart failure recommendations. Future therapeutic approaches include repurposed molecularly directed drugs, siRNA- based gene silencing, and genome editing. Summary LMNA-related cardiomyopathy is the focus of active in vitro and in vivo research, which is expected to generate novel biomarkers and identify new therapeutic targets. LMNA-related cardiomyopathy trials are currently underway. Keywords Lamin A/C gene . Laminopathy . Heart failure . Arrhythmias . Mechanotransduction . P53 . CRISPR–Cas9 therapy Introduction functions, including maintaining nuclear structural integrity, regulating gene expression, mechanosensing, and Mutations in the lamin A/C gene (LMNA)causelaminopathies, mechanotransduction through the lamina-associated proteins a heterogeneous group of inherited disorders including muscu- [6–11]. -

Hippocampal LMNA Gene Expression Is Increased in Late-Stage Alzheimer’S Disease
International Journal of Molecular Sciences Article Hippocampal LMNA Gene Expression is Increased in Late-Stage Alzheimer’s Disease Iván Méndez-López 1,2,*,†, Idoia Blanco-Luquin 1,†, Javier Sánchez-Ruiz de Gordoa 1,3, Amaya Urdánoz-Casado 1, Miren Roldán 1, Blanca Acha 1, Carmen Echavarri 1,4, Victoria Zelaya 5, Ivonne Jericó 3 and Maite Mendioroz 1,3,* 1 Neuroepigenetics Laboratory-Navarrabiomed, Complejo Hospitalario de Navarra, Universidad Pública de Navarra (UPNA), IdiSNA (Navarra Institute for Health Research), Pamplona, Navarra 31008, Spain; [email protected] (I.B.-L.); [email protected] (J.S.-R.d.G.); [email protected] (A.U.-C.); [email protected] (M.R.); [email protected] (B.A.); [email protected] (C.E.) 2 Department of Internal Medicine, Hospital García Orcoyen, Estella 31200, Spain 3 Department of Neurology, Complejo Hospitalario de Navarra- IdiSNA (Navarra Institute for Health Research), Pamplona, Navarra 31008, Spain; [email protected] 4 Hospital Psicogeriátrico Josefina Arregui, Alsasua, Navarra 31800, Spain 5 Department of Pathology, Complejo Hospitalario de Navarra- IdiSNA (Navarra Institute for Health Research), Pamplona, Navarra 31008, Spain; [email protected] * Correspondence: [email protected] (I.M.-L.); [email protected] (M.M.); Tel.: +34-848-422677 (I.M.-L.) † These authors contributed equally to this work. Received: 30 November 2018; Accepted: 14 February 2019; Published: 18 February 2019 Abstract: Lamins are fibrillary proteins that are crucial in maintaining nuclear shape and function. Recently, B-type lamin dysfunction has been linked to tauopathies. However, the role of A-type lamin in neurodegeneration is still obscure. -

Atrial Fibrillation (ATRIA) Study
European Journal of Human Genetics (2014) 22, 297–306 & 2014 Macmillan Publishers Limited All rights reserved 1018-4813/14 www.nature.com/ejhg REVIEW Atrial fibrillation: the role of common and rare genetic variants Morten S Olesen*,1,2,4, Morten W Nielsen1,2,4, Stig Haunsø1,2,3 and Jesper H Svendsen1,2,3 Atrial fibrillation (AF) is the most common cardiac arrhythmia affecting 1–2% of the general population. A number of studies have demonstrated that AF, and in particular lone AF, has a substantial genetic component. Monogenic mutations in lone and familial AF, although rare, have been recognized for many years. Presently, mutations in 25 genes have been associated with AF. However, the complexity of monogenic AF is illustrated by the recent finding that both gain- and loss-of-function mutations in the same gene can cause AF. Genome-wide association studies (GWAS) have indicated that common single-nucleotide polymorphisms (SNPs) have a role in the development of AF. Following the first GWAS discovering the association between PITX2 and AF, several new GWAS reports have identified SNPs associated with susceptibility of AF. To date, nine SNPs have been associated with AF. The exact biological pathways involving these SNPs and the development of AF are now starting to be elucidated. Since the first GWAS, the number of papers concerning the genetic basis of AF has increased drastically and the majority of these papers are for the first time included in a review. In this review, we discuss the genetic basis of AF and the role of both common and rare genetic variants in the susceptibility of developing AF. -
Neurodegeneration in Accelerated Aging
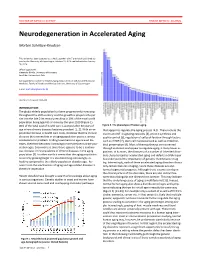
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -

Trichothiodystrophy
Trichothiodystrophy Author: Doctor Alfredo Rossi1 and Doctor C. Cantisani. Creation date: June 2004 Scientific Editor: Prof Antonella Tosti 1Dipartimento di Malattie Cutanee-Veneree Chirurgia Plastica-Ricostruttiva, Università degli studi di Roma “La Sapienza” Abstract Keywords Definition Epidemiology Etiology Clinical description Diagnostic methods Prenatal diagnosis Management References Abstract Trichothiodystrophy (TTD) is a rare autosomal recessive genetic disorder characterized by abnormal synthesis of the sulphur containing keratins and consequently hair dysplasia, associated with numerous symptoms affecting mainly organs derived from the neuroectoderm. This phenotypic aspect is due to mutations in the DNA-dependent ATPase/helicase subunit of TFIIH, XPB and XPD. Abnormalities in excision repair of ultraviolet (UV)-damaged DNA are recognized in about half of the patients. The clinical appearance is characterized by brittle and fragile hair, congenital ichthyosis, nail and dental dysplasias, cataract, progeria-like face, growth and mental retardation. The abnormalities are usually obvious at birth, with variable clinical expression. The variants of TTD, depending on their different associations, are known by the initials BIDS, IBIDS, PIBIDS, SIBIDS, ONMRS, as well as the eponyms of the Pollit, Tay, Sabinas syndromes or Amish brittle hair. The exact prevalence of TTD is unknown, but appears to be rather uncommon. About 20 cases of PIBI(D)S have been reported in the literature. Up to 1991, clinical data of 15 cases with IBIDS were published. Prenatal diagnostic of TTD is available. There is no specific treatment. Keywords Brittle hair, photosensitivity, ichthyosis, BIDS, IBIDS, PIBIDS, SIBIDS, ONMRS, Tay-syndrome Definition tail pattern). They named it Trichothiodystrophy, Trichothiodystrophy (TTD) is a group of rare noticing also an increased Photosensitivity and autosomal recessive disorders with heterogenic Ichthyosis in these patients (PIBIDS).