Eorgian Edical Ews
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

I.S. Beritashvili and Psychoneural Integration of Behavior (PDF)
I.S. Beritashvili and Psychoneural Integration of Behavior Merab G. Tsagareli1,* 1 Ivane Beritashvili Center for Experimental Biomedicine, Tbilisi, Georgia [email protected] Abstract. Ivane S. Beritashvili’s doctrine of psychoneural or goal-directed behavior was established in the late 1920s. It bears a strong resemblance to the concepts of purposive behavior and “cognitive maps” developed in parallel by Edward C. Tolman (1932), and significantly anticipated respective modern concepts. Beritashvili’s research was motivated by a disagreement with Ivan P. Pavlov concerning the physiological bases of conditioned reflex formation. In the late 1920s, Beritashvili came to the conclusion that due to the great restrictions it placed on animals’ behavioral repertoire, the Pavlov-Bechterev type of conditioning was not a proper model for the study of behavior. Instead, Beritashvili came to prefer the method of “free movement” of the experimental animal. He then pursued an ingenious and extensive investigation of comparative memory in vertebrates. This revealed the unique nature of mammalian memory processes, which he forthrightly called “image-driven” and unequivocally distinguished from memory processes underlying conditional reflexes. These extraordinary works led to the discovery of the mediation of animal goal-directed behavior by image-driven memory. Keywords: animal behavioral science, conditioned reflexes, goal-directed behavior, image-driven memory, learning, spatial orientation 1 Introduction The phrase “psychoneural integration of behavior” was used by Ivane S. Beritashvili† in the title of his article in the Annual Review of Physiology in 1966 [1], which formed the prefatory chapter to a thick volume covering numerous areas of physiology. To some degree following Ivan M. -

Specific Support to Georgia: Horizon 2020 Policy Support Facility Mission (1) Mission Dates: December 4-7, 2017 Agenda Monday, December 4, 2017
Specific Support to Georgia: Horizon 2020 Policy Support Facility mission (1) Mission dates: December 4-7, 2017 Agenda Monday, December 4, 2017 Time Meeting Venue 13:00 – 14:00 Dr. Mikheil Chkhenkeli, Minister of Education and Ministry of Education and Science of Science of Georgia Georgia Address: #52 Dimitri Uznadze Str., Dr. Alexander Tevzadze, Deputy Minister of Tbilisi, Georgia Education and Science of Georgia 15:00 – 17:00 Meeting with Rectors of Major State Research Ivane Javakhishvili Tbilisi State University Universities of Georgia: Address: #1 Chavchavadze ave. Room - Ivane Javakhishvili Tbilisi State University #107 Dr. George Sharvashidze, Rector, - Ilia State University Dr. Giga Zedania, Rector, - Georgian Technical University Dr. Archil Prangishvili - Tbilisi State Medical University Dr. Zurab Vadachkoria, Rector, - Sokhumi State University Dr. Zurab Khonelidze, Rector - Akaki Tsereteli State University Dr. George Ghavtadze - Shota Meskhia State Teaching University of Zugdidi Dr. Tea Khupenia - Batumi Shota Rustaveli State University Dr. Natia Tsiklashvili - Samtskhe-Javakheti State University Merab Beridze/Maka Kachkachishvili-Beridze 17:30 – 18:30 Meeting with representatives of MoES, SRNSFG Shota Rustaveli National Science and the delegationn of the European Union to Foundation of Georgia, Georgia: Address: # 1 Aleksidze Street, III floor, Conference Hall Mr. Kakha Khandolishvili, Ms.Natia Gabitashvili, Ms. Manana Mikaberidze, Dr. Nino Gachechiladze, Dr. Ekaterine Kldiashvili, Ms. Mariam Keburia Ms. Nika Kochishvili Wrap-up -

Implementing Agency: Social Service Agency, LEPL
Chapter V Affordable, Quality Healthcare and Social Security 1.1. Social Security of Population (Program Code: 35 02) Implementing Agency: Social Service Agency, LEPL 1.1.1. Pension Payments to Population (Program Code: 35 02 01) • Beneficiaries of state pensions and state compensations envisaged in Laws of Georgia on State pension, State Commensations and State Academic Bursaries have been paid pensions through financing the commitments made by the State on pension payments; • State pensions have been paid in January to over 708.1 thousand individuals, in February – to over 708.6 thousand individuals, in March – to over 709.4 thousand individuals, in April – to over 710.6 thousand individuals, in May – to over 711.5 thousand individuals, in June – to over 713.0 thousand individuals, in July – to over 714,2 thousand individuals, in August – to over 716.3 thousand individuals, in September – to over 717.8 thousand individuals, while state compensations have been paid in January-February to over 20.7-20.7 thousand beneficiaries, in March – to over 20.8 thousand beneficiaries, in April-May – to over 20.9-20.9 thousand beneficiaries, in June – to over 20.8 thousand beneficiaries and July-September - to over 20.9-20.9 thousand beneficiaries. Total expenditure towards this end in the reporting period has been 1 153.1 MLN GEL. 1.1.2. Social Security of Targeted Groups of Population (Program Code: 35 02 02) • Number of beneficiaries getting subsistance minimum in January has amounted over 407.3 thousand individuals, February – over 422.0 thousand -

Tsu Mecniereba TSU Science
Tsu mecniereba N4 TSUivlisi.2013.July Science stresis zegavlena ujredul metabolizmze Tavis tvinSi xelovnuri saperfuzio sistemebi - Tsu mecnierebisgan muslimi mesxebi - integracia Tu separacia? Sah-names versiebi saqarTvelodan Canasaxis sicocxlis ufleba The Effects of Stress on the Cellular Metabolism of the Brain The Embryo’s Right to Life in Georgia and the World TSU Scientists Work on Artificial Perfusion Systems Muslim Meskhetians – Integration or Separation? Georgia Presents Versions of Shahnameh Tsu I korpusi. gamocdis molodinSi TSU Building I. Students awaiting exams sarCevi - Contents Tsu stabilurad inarCunebs lideri 3 TSU firmly maintains its status as a leading samecniero-kvleviTi dawesebulebis research institution statuss Sah-names versiebi saqarTvelodan 8 Georgia Presents Versions of Shahnameh qarTuli palimfsesturi xelnawerebi 13 Georgian Palimpsest Manuscripts bilingvuri ganaTlebis xelSemSleli da 16 Factors Inhibiting or Promoting Bilingual xelSemwyobi faqtorebi saqarTveloSi Education in Georgia "rac ufro metia kvleva religiis da 20 “The more research is carried out in the sekularizmis sakiTxze, miT ufro field of religion and secularism, the more meti kiTxva Cndeba" questions are raised’’ saqarTvelos saxelmwifo sazRvris 25 A Scientific Basis for Georgian State delimitacia-demarkaciisaTvis Border Demarcation mecnieruli bazis Sesaqmnelad biosamedicino daniSnulebis 29 Magnetic Nanoparticles for Biomedical magnituri nanonawilakebi Applications protonis gadatanis reaqciebis 34 Non-Traditional Proton Transfer Reaction aratradiciuli -
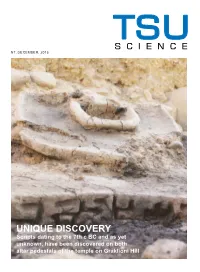
UNIQUE DISCOVERY Scripts Dating to the 7Th C BC and As Yet Unknown, Have Been Discovered on Both Altar Pedestals of the Temple on Graklioni Hill TSU SCIENCE CONTENTS
TSU SCIENCE N7, DECEMBER, 2015 UNIQUE DISCOVERY Scripts dating to the 7th c BC and as yet unknown, have been discovered on both altar pedestals of the temple on Graklioni Hill TSU SCIENCE CONTENTS TSU SCIENCE • 2015 14 THE GELATI BIBLE WITH CATENAS 3 TSU – LEADING IN THE CAUCASUS REGION ACCORDING TO UNIVERSITY 29 THE EUROPEANIZATION RANKINGS 16 INDICATORS OF OF GEORGIA’S POST-TRAUMATIC NATIONAL SECURITY GROWTH (PTG) AND PSYCHOLOGICAL 32 TEXTBOOK ON WELL-BEING IN LIFE PROBATION LAW STORIES 34 LIBERALIZING TRENDS 20 CITIZENSHIP STYLES IN GEORGIAN CRIMINAL IN GEORGIA LAW 5 TSU SCIENTISTS MAKE A UNIQUE DISCOVERY 23 MATERIALS FROM ILIA CHAVCHAVADZE’S PERSONAL ENCYCLOPAEDIA 37 GEOLOGY AND 10 ANTHIM IVERIANUL – PROBLEMS OF THE GEORGIAN-EUROPEAN 26 SECURITY STUDIES AT VARDZIA CAVE DIALOGUE TSU MONASTERY COMPLEX TSU CONTENTS SCIENCE №7, 2015 Editorial Board: Vladimer Papava – Rector, Academician of the Georgian Na- tional Academy of Sciences, Chairman of the Editorial Board Merab Eliashvili – Deputy Rector, Professor, Deputy Chairman of the Editorial Board 50 MAJOR DENTAL Levan Aleksidze – Director of TSU Institute of International DISEASES Law, Academician of the Georgian National Academy of Sci- IN GEORGIA ences, Professor, Deputy Chairman of the Editorial Board AND MODERN Giorgi Gvedashvili – Professor, Head of the Department of Sci- entific Research and Development APPROACHES TO TBILISI STATE Revaz Gachechiladze – TSU Professor, corresponding member 39 PREVENTION of the Georgian National Academy of Sciences UNIVERSITY AND Iago Kachkachishvili -

Ivane Beritashvili: Founder of Physiology and Neuroscience in Georgia Merab G
This article was downloaded by: [University Library Utrecht] On: 17 August 2013, At: 12:48 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of the History of the Neurosciences: Basic and Clinical Perspectives Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/njhn20 Ivane Beritashvili: Founder of Physiology and Neuroscience in Georgia Merab G. Tsagareli a a Beritashvili Institute of Physiology, Tbilisi, Georgia Published online: 11 Jul 2007. To cite this article: Merab G. Tsagareli (2007) Ivane Beritashvili: Founder of Physiology and Neuroscience in Georgia, Journal of the History of the Neurosciences: Basic and Clinical Perspectives, 16:3, 288-306, DOI: 10.1080/09647040600600148 To link to this article: http://dx.doi.org/10.1080/09647040600600148 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. -

Beritashvili, Ivane
12/15/12 Ev ernote Web Beritashvili, Ivane Saturday, December 15 2012, 10:42 AM Ivane Beritashvili (1884-1974) Citation: Tsagareli, Merab G. (2006), IBRO History of Neuroscience, Ivane Beritashvili (1884-1974), IBRO History of Neuroscience [http://www.ibro.info/Pub/Pub_Main_Display.asp?LC_Docs_ID=3443] Accessed: date Ivane Beritashvili (1884-1974) Merab G. Tsagareli This article is dedicated to one of the outstanding neuroscientists of the 20th century - Ivane Beritashvili, the founder of the national school of physiology and neuroscience in Georgia. His most significant contribution was the discovery of the mediation of animal psychoneural behavior by image-driven memory. In 1958-60, together with Herbert Jasper, Henri Gastaut, Alfred Fessard and Vladimir Rusinov, he was one of the founders of the IBRO. Ivane S. Beritashvili, the son of a priest, was born on 31 December 1884 in the small village of Vegini in Kakheti, in the Eastern region of Georgia (at that time part of the Russian Empire). He first studied for the priesthood at the ecclesiastic school in Telavi, the main city of Kakheti, and then at the theological seminary in Tiflis (Tbilisi), capital of Georgia. Because he came to dislike the prospect of becoming a priest, the young Ivane took examinations for the school-leaving certificate at the 2nd Tiflis gymnasium in 1906. In the same year he matriculated into the Natural Division of the Department of Physical and Mathematical Sciences of St. Petersburg University. Beritashvili began his experimental research early, as a third year student under the supervision of the eminent Russian physiologist Prof. N.E. -

Caucasus Journal of Social Sciences
aucasus Journal C of social sciences Volume 11 2018 Politics and International Relations Education History and Anthropology Humanities Law and Art Public Health and Psychology Business and Economics ISSN 1512-3677 www.ug.edu.ge Caucasus Journal of Social Sciences Volume 11 Issue 1 The University of Georgia Publishing House Tbilisi 2018 UDC(uak) 908 (479) (06) k144 Printed at The University of Georgia. Tbilisi, Georgia. Copyright © 2018. All rights reserved by the University of Georgia. Permission to make digital or hard copies of part or all of this work for personal or classroom use is granted without fee provided that copies are not made or distributed for profit or commercial advantage. No responsibility for the views expressed by authors in the Caucasus Journal of Social Sciences is assumed by the editors or the publisher. Caucasus Journal of Social Sciences The University of Georgia. Georgia, Tbilisi, 0175. M. Kostava Street 77, Building IV. Tel: (+995 32) 255 22 22 Email: [email protected] Copyright © 2018 Caucasus Journal of Social Sciences ISSN 1512-3677 Caucasus Journal of Social Sciences Editor-in-Chief Jeremiah Paul Johnson Managing Editor Julieta Andguladze Board of Editors Abuladze Konstantine Tbilisi Teaching University “Gorgasali” Alasania Giuli The University of Georgia Blauvelt Timothy American Councils Carper Mark The University of Alaska Anchorage Davies Janette Oxford University Dzebisashvili Lasha The University of Georgia Ghudushauri Tinatin The University of Georgia Gvelesiani Mariam The University of Georgia -
Creation of Core-Course in Georgian Language from National Specificity
8th EUTERP WORKSHOP Optimization of training in radiation protection Dolmen Hotel, Qawra, St Paul’s Bay, Malta April 10-12, 2019 Creation of core-course in Georgian language from national specificity and needs of Georgia in radiation safety, with structure of additional modules and creation and publishing the handbook D.Nadareishvili Z.Sichinava K. Jariashvili I.Beritashvili Center of Experimental Biomedicine Agency of Nuclear and Radiation Safety ANRS Tbilisi, Georgia Pharnavaz I ; 3rd century BC: 302–237 BC The Old Georgian tradition (in particular, Leonti Mroveli, the eleventh-century historian) ascribes the creation of the Georgian alphabet to Parnavaz I, the king of Georgia in the third century B.C. Writing systems in Europe . The Georgian scripts are the Modern Georgian alphabet three writing systems used to Mkhedruli(modern) and “qwerty” write the Georgian language: Asomtavruli, Nuskhuri and Mkhedruli. Although the systems differ in appearance, all three are unicase, their letters share the same names and alphabetical order, and are written horizontally from left to right. Of the three scripts, Mkhedruli, once the civilian royal script of the Kingdom of Georgia and mostly used for the royal charters, is now the standard script for modern Georgian and its related Kartvelian languages, Nuskhuri Asomtavruli whereas Asomtavruli and Nuskhuri are used only by the Georgian Orthodox Church, in Georgian Alphabet in UNESCO ceremonial religious texts and iconography. Intangible Cultural Heritage List In 2010 the I.Beritashvili Experimental Biomedicine Center (www.biomedicine.org.ge) was founded on the bases of I.Beritashvili Institute of Physiology, Centre of Radiobiology and Radiation Ecology (Founded in 1991), Institute of Molecular Biology and Biological Physics and the Center of Experimental Neurology Research.