Current Understanding of Klippel-Trenaunay Syndrome: a Review Article Philip Sheridan Grand Valley State University
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Aggf1 Attenuates Neuroinflammation and BBB Disruption Via PI3K/Akt/NF-Κb Pathway After Subarachnoid Hemorrhage in Rats
Zhu et al. Journal of Neuroinflammation (2018) 15:178 https://doi.org/10.1186/s12974-018-1211-8 RESEARCH Open Access Aggf1 attenuates neuroinflammation and BBB disruption via PI3K/Akt/NF-κB pathway after subarachnoid hemorrhage in rats Qiquan Zhu1,2, Budbazar Enkhjargal2, Lei Huang2,4, Tongyu Zhang2, Chengmei Sun2, Zhiyi Xie2, Pei Wu2, Jun Mo2, Jiping Tang2, Zongyi Xie1* and John H. Zhang2,3,4* Abstract Background: Neuroinflammation and blood-brain barrier (BBB) disruption are two critical mechanisms of subarachnoid hemorrhage (SAH)-induced brain injury, which are closely related to patient prognosis. Recently, angiogenic factor with G-patch and FHA domain 1 (Aggf1) was shown to inhibit inflammatory effect and preserve vascular integrity in non-nervous system diseases. This study aimed to determine whether Aggf1 could attenuate neuroinflammation and preserve BBB integrity after experimental SAH, as well as the underlying mechanisms of its protective roles. Methods: Two hundred forty-nine male Sprague-Dawley rats were subjected to the endovascular perforation model of SAH. Recombinant human Aggf1 (rh-Aggf1) was administered intravenously via tail vein injection at 1 h after SAH induction. To investigate the underlying neuroprotection mechanism, Aggf1 small interfering RNA (Aggf1 siRNA) and PI3K-specific inhibitor LY294002 were administered through intracerebroventricular (i.c.v.) before SAH induction. SAH grade, neurological score, brain water content, BBB permeability, Western blot, and immunohistochemistry were performed. Results: Expression of endogenous Aggf1 was markedly increased after SAH. Aggf1 was primarily expressed in endothelial cells and astrocytes, as well as microglia after SAH. Administration of rh-Aggf1 significantly reduced brain water content and BBB permeability, decreased the numbers of infiltrating neutrophils, and activated microglia in the ipsilateral cerebral cortex following SAH. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -
Pancancer Progression Human Vjune2017
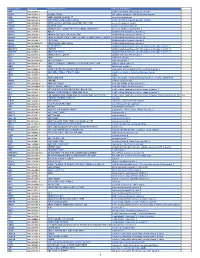
Gene Symbol Accession Alias/Prev Symbol Official Full Name AAMP NM_001087.3 - angio-associated, migratory cell protein ABI3BP NM_015429.3 NESHBP|TARSH ABI family, member 3 (NESH) binding protein ACHE NM_000665.3 ACEE|ARACHE|N-ACHE|YT acetylcholinesterase ACTG2 NM_001615.3 ACT|ACTA3|ACTE|ACTL3|ACTSG actin, gamma 2, smooth muscle, enteric ACVR1 NM_001105.2 ACTRI|ACVR1A|ACVRLK2|ALK2|FOP|SKR1|TSRI activin A receptor, type I ACVR1C NM_145259.2 ACVRLK7|ALK7 activin A receptor, type IC ACVRL1 NM_000020.1 ACVRLK1|ALK-1|ALK1|HHT|HHT2|ORW2|SKR3|TSR-I activin A receptor type II-like 1 ADAM15 NM_207195.1 MDC15 ADAM metallopeptidase domain 15 ADAM17 NM_003183.4 ADAM18|CD156B|CSVP|NISBD|TACE ADAM metallopeptidase domain 17 ADAM28 NM_014265.4 ADAM 28|ADAM23|MDC-L|MDC-Lm|MDC-Ls|MDCL|eMDC II|eMDCII ADAM metallopeptidase domain 28 ADAM8 NM_001109.4 CD156|MS2 ADAM metallopeptidase domain 8 ADAM9 NM_001005845.1 CORD9|MCMP|MDC9|Mltng ADAM metallopeptidase domain 9 ADAMTS1 NM_006988.3 C3-C5|METH1 ADAM metallopeptidase with thrombospondin type 1 motif, 1 ADAMTS12 NM_030955.2 PRO4389 ADAM metallopeptidase with thrombospondin type 1 motif, 12 ADAMTS8 NM_007037.4 ADAM-TS8|METH2 ADAM metallopeptidase with thrombospondin type 1 motif, 8 ADAP1 NM_006869.2 CENTA1|GCS1L|p42IP4 ArfGAP with dual PH domains 1 ADD1 NM_001119.4 ADDA adducin 1 (alpha) ADM2 NM_001253845.1 AM2|dJ579N16.4 adrenomedullin 2 ADRA2B NM_000682.4 ADRA2L1|ADRA2RL1|ADRARL1|ALPHA2BAR|alpha-2BAR adrenoceptor alpha 2B AEBP1 NM_001129.3 ACLP AE binding protein 1 AGGF1 NM_018046.3 GPATC7|GPATCH7|HSU84971|HUS84971|VG5Q -
Protocol Booklet
OmniKine™ Human TWEAK Colorimetric ELISA Kit Catalog #: OK-0169 Detection and Quantification of Human TWEAK Concentrations in Cell Lysates, Sera and Plasma. Please read the provided manual as suggested experimental protocols may have changed. Research Purposes Only. Not Intended for Diagnostic or Clinical Procedures. CONTENTS PAGE Introduction………………………………………………..…………….………..3 Assay Principles……………………………………………………….…………4 Assay Format………………………………………………………………..……5 Assay Restrictions……………………………………………………….……….6 Materials Included……………………………………………….……………….6 Additional Materials Required…………………………………………….…….7 Health and Safety Precautions…………………………………………….…...7 Storage Information………………………………………………………….…..8 Sample Preparation and Storage……………………………………………….9 Sample Experiment Layout…………………………………………………....10 Immunoassay Protocol……………………………………….…………….…..11 Summarized Protocol………………………………………………………......16 Sensitivity………………………………………………………………………..17 Cross Reactivity and Specificity……………………………………….…...…17 Technical Support……………………………………………….……………...18 ELISA Plate Template……………………………………………………..…...19 Notes…………………………………………………………….……………….20 OmniKine™ | Human TWEAK | 2 INTRODUCTION Human TWEAK or TNF-Related Weak Inducer of Apoptosis, also known as the APO3 Ligand, is a 249 amino acid cytokine protein that belongs to the tumor necrosis factor ligand superfamily. Encoded from the TNFSF12 gene located at locus 17p13 on chromosome 17, TWEAK is a ligand for the FN14/TWEAK receptor and has overlapping signaling functions with TNF, but displays a much wider tissue -

Elevated Expression of AGGF1 Predicts Poor Prognosis and Promotes the Metastasis of Colorectal Cancer
Elevated expression of AGGF1 predicts poor prognosis and promotes the metastasis of colorectal cancer Xin Zhang Zhejiang Provincial People's Hospital Huimin Sun Weifang People's Hospital Wanyuan Chen Zhejiang Provincial People's Hospital Xianglei He ( [email protected] ) Zhejiang Provincial People's Hospital https://orcid.org/0000-0002-7685-3451 Research article Keywords: Colorectal cancer; AGGF1; Prognosis; Metastasis Posted Date: October 25th, 2019 DOI: https://doi.org/10.21203/rs.2.14319/v2 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on December 27th, 2019. See the published version at https://doi.org/10.1186/s12885-019-6474-7. Page 1/15 Abstract Abstract Background: Angiogenic factor with G-patch and FHA domains 1 (AGGF1) can promote angiogenesis and increasing evidence has highlighted the important roles of AGGF1 in tumorigenesis. However, the expression patterns as well as the biological functions of AGGF1 in colorectal cancer (CRC) remain to be established. The purpose of the present study is therefore to identify the effect of AGGF1 on prognosis and metastasis in CRC patients. Methods: The expression level of AGGF1 in CRC was examined by qPCR, western blot and immunohistochemistry in a tissue microarray containing 101 CRC specimens. And the effect of AGGF1 on CRC cell malignance was investigated in our established stable AGGF1 upregulated and knockdown CRC cell lines. Results: The expression level of AGGF1 in CRC tissue was not signicantly different to that in adjacent normal mucosa at the mRNA level. -

BMP Signaling in Vascular Biology and Dysfunction
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Lirias Accepted Manuscript Title: BMP signaling in vascular biology and dysfunction Author: Amaya Garc´ıa de Vinuesa Salim Abdelilah-Seyfried Petra Knaus An Zwijsen Sabine Bailly This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. BMP signaling in vascular biology and dysfunction Amaya García de Vinuesa1, Salim Abdelilah-Seyfried2,3, Petra Knaus4, An Zwijsen5,6*, Sabine Bailly7,8,9* 1Department of Molecular Cell Biology, Cancer Genomics Centre Netherlands, Leiden University Medical Center, Leiden, the Netherlands. 2Institute of Biochemistry and Biology, Potsdam University, Karl-Liebknecht-Straße 24- 25, D-14476 Potsdam, Germany. 3Institute of Molecular Biology, Hannover Medical School, Carl-Neuberg Straße 1, D- 30625 Hannover, Germany. 4Institute for Chemistry and Biochemistry, Freie Universitaet Berlin, Berlin, Germany. 5VIB Center for the Biology of Disease, Leuven, Belgium 6KU Leuven, Dept Human Genetics, Leuven, Belgium 7Institut National de la Santé et de la Recherche Médicale (INSERM, U1036), Grenoble, France F-38000 8Commissariat à l’Énergie -

Role of Kcnma1 in the Pathogenesis of Gepd Syndrome
ROLE OF KCNMA1 IN THE PATHOGENESIS OF GEPD SYNDROME WEI DU Bachelor of Science in Biochemistry Beijing Normal University June, 2001 Submitted in partial fulfillment of requirements for the degree DOCTOR OF PHILOSOPHY IN REGULATORY BIOLOGY at the CLEVELAND STATE UNIVERSITY NOVEMBER, 2009 This dissertation has been approved for the Department of Biological, Geological, and Environmental Sciences and the College of Graduate Studies by ___________________________________________ Dissertation Chairperson, Qing Wang __________________________ Department & Date ___________________________________________ Crystal Weyman __________________________ Department & Date ___________________________________________ Sadashiva Karnik __________________________ Department & Date ___________________________________________ Xiaoxia Li __________________________ Department & Date ___________________________________________ Roman Kondratov __________________________ Department & Date ___________________________________________ Qiuyun Chen __________________________ Department & Date ACKNOWLEDGEMENT I would like to thank my advisor, Dr. Qing Wang, for his help and support. I want to thank my committee members, Dr. Crystal Weyman, Dr. Sadashiva Karnik, Dr. Xiaoxia Li, Dr. Roman Kondratov, and Dr. Qiuyun Chen, for their time and effort. I want to thank Dr. Jocelyn Bautista for collecting the blood samples from the patients. I want to thank our collaborators, Dr. Jianmin Cui, Dr. George Richerson, Dr. Huanghe Yang, and Dr. Ana Diez-Sampedro. I want to thank Dr. -

Genetic Syndromes with Vascular Malformations – Update on Molecular Background and Diagnostics
State of the art paper Genetics Genetic syndromes with vascular malformations – update on molecular background and diagnostics Adam Ustaszewski1,2, Joanna Janowska-Głowacka2, Katarzyna Wołyńska2, Anna Pietrzak3, Magdalena Badura-Stronka2 1Institute of Human Genetics, Polish Academy of Sciences, Poznan, Poland Corresponding author: 2Department of Medical Genetics, Poznan University of Medical Sciences, Poznan, Adam Ustaszewski Poland Institute of Human Genetics 3Department of Neurology, Poznan University of Medical Sciences, Poznan, Poland Polish Academy of Sciences 32 Strzeszynska St Submitted: 19 April 2018; Accepted: 9 September 2018 60-479 Poznan, Poland Online publication: 25 February 2020 Phone: +48 61 65 79 223 E-mail: adam.ustaszewski@ Arch Med Sci 2021; 17 (4): 965–991 igcz.poznan.pl DOI: https://doi.org/10.5114/aoms.2020.93260 Copyright © 2020 Termedia & Banach Abstract Vascular malformations are present in a great variety of congenital syn- dromes, either as the predominant or additional feature. They pose a major challenge to the clinician: due to significant phenotype overlap, a precise diagnosis is often difficult to obtain, some of the malformations carry a risk of life threatening complications and, for many entities, treatment is not well established. To facilitate their recognition and aid in differentiation, we present a selection of notable congenital disorders of vascular system development, distinguishing between the heritable germinal and sporadic somatic mutations as their causes. Clinical features, genetic background and comprehensible description of molecular mechanisms is provided for each entity. Key words: arteriovenous malformation, vascular malformation, capillary malformation, venous malformation, arterial malformation, lymphatic malformation. Introduction Congenital vascular malformations (VMs) are disorders of vascular architecture development. -

Molecular Signatures Differentiate Immune States in Type 1 Diabetes Families
Page 1 of 65 Diabetes Molecular signatures differentiate immune states in Type 1 diabetes families Yi-Guang Chen1, Susanne M. Cabrera1, Shuang Jia1, Mary L. Kaldunski1, Joanna Kramer1, Sami Cheong2, Rhonda Geoffrey1, Mark F. Roethle1, Jeffrey E. Woodliff3, Carla J. Greenbaum4, Xujing Wang5, and Martin J. Hessner1 1The Max McGee National Research Center for Juvenile Diabetes, Children's Research Institute of Children's Hospital of Wisconsin, and Department of Pediatrics at the Medical College of Wisconsin Milwaukee, WI 53226, USA. 2The Department of Mathematical Sciences, University of Wisconsin-Milwaukee, Milwaukee, WI 53211, USA. 3Flow Cytometry & Cell Separation Facility, Bindley Bioscience Center, Purdue University, West Lafayette, IN 47907, USA. 4Diabetes Research Program, Benaroya Research Institute, Seattle, WA, 98101, USA. 5Systems Biology Center, the National Heart, Lung, and Blood Institute, the National Institutes of Health, Bethesda, MD 20824, USA. Corresponding author: Martin J. Hessner, Ph.D., The Department of Pediatrics, The Medical College of Wisconsin, Milwaukee, WI 53226, USA Tel: 011-1-414-955-4496; Fax: 011-1-414-955-6663; E-mail: [email protected]. Running title: Innate Inflammation in T1D Families Word count: 3999 Number of Tables: 1 Number of Figures: 7 1 For Peer Review Only Diabetes Publish Ahead of Print, published online April 23, 2014 Diabetes Page 2 of 65 ABSTRACT Mechanisms associated with Type 1 diabetes (T1D) development remain incompletely defined. Employing a sensitive array-based bioassay where patient plasma is used to induce transcriptional responses in healthy leukocytes, we previously reported disease-specific, partially IL-1 dependent, signatures associated with pre and recent onset (RO) T1D relative to unrelated healthy controls (uHC). -

Β-Catenin-Dependent Transcription Is Central to Bmp-Mediated Formation
© 2015. Published by The Company of Biologists Ltd | Development (2015) 142, 497-509 doi:10.1242/dev.115576 RESEARCH ARTICLE β-catenin-dependent transcription is central to Bmp-mediated formation of venous vessels Takeru Kashiwada1,2, Shigetomo Fukuhara1,*, Kenta Terai3, Toru Tanaka1,2, Yuki Wakayama1, Koji Ando1, Hiroyuki Nakajima1, Hajime Fukui1, Shinya Yuge1, Yoshinobu Saito2, Akihiko Gemma2 and Naoki Mochizuki1,4,* ABSTRACT 2009). In the absence of Wnt signaling, cytosolic β-catenin is β-catenin regulates the transcription of genes involved in diverse phosphorylated by a destruction complex composed of axin, β biological processes, including embryogenesis, tissue homeostasis adenomatous polyposis coli and glycogen synthase kinase 3 , β and regeneration. Endothelial cell (EC)-specific gene-targeting which leads to degradation of -catenin via the ubiquitin- analyses in mice have revealed that β-catenin is required for proteasome pathway. Wnt inhibits the activity of this destruction vascular development. However, the precise function of β-catenin- complex, resulting in the stabilization and nuclear translocation of β β mediated gene regulation in vascular development is not well -catenin. In the nucleus, -catenin associates with the T-cell factor understood, since β-catenin regulates not only gene expression but (Tcf)/lymphoid enhancer factor family of transcription factors, also the formation of cell-cell junctions. To address this question, we thereby inducing the transcription of target genes. In addition, β have developed a novel transgenic zebrafish line that allows the -catenin regulates cell-cell adhesions by linking cadherin molecules α visualization of β-catenin transcriptional activity specifically in ECs to the actin cytoskeleton via -catenin (Dejana et al., 2008). -

Angiogenic Factor with G Patch and FHA Domains 1 (AGGF1) Is a Novel Identified Initiator of Angiogenesis Through Promoting the Proliferation of Endothelial Cells
CLINICAL RESEARCH e-ISSN 1643-3750 © Med Sci Monit, 2020; 26: e919896 DOI: 10.12659/MSM.919896 Received: 2019.09.04 Accepted: 2019.12.03 Angiogenic Factor with G Patch and FHA Available online: 2020.01.22 Published: 2020.02.24 Domains 1 (AGGF1) Acts as Diagnostic Biomarker and Adverse Prognostic Factor of Hepatocellular Carcinoma (HCC): Evidence from Bioinformatic Analysis Authors’ Contribution: BCDEF Wensheng Wang* Department of Gastroenterology, Daping Hospital, Army Medical University, Study Design A BCDEF Guangxi Zhu* Chongqing, P.R. China Data Collection B Statistical Analysis C BDEF Shujie Lai Data Interpretation D CDEF Yan Guo Manuscript Preparation E BCEF Xinru Yin Literature Search F Funds Collection G ADFG Dongfeng Chen ABCEF Liangzhi Wen * Wensheng Wang and Guangxi Zhu contributed equally Corresponding Authors: Dongfeng Chen, e-mail: [email protected], Liangzhi Wen, e-mail: [email protected] Source of support: Departmental sources Background: Angiogenic factor with G patch and FHA domains 1 (AGGF1) is a novel identified initiator of angiogenesis through promoting the proliferation of endothelial cells. The continuous angiogenesis plays a key role in the growth, invasion, and metastasis of hepatocellular carcinoma (HCC), while the diagnostic and prognostic roles of AGGF1 for HCC need to be further studied. Material/Methods: The mRNA sequencing datasets and clinical features of HCC patients were extracted from The Cancer Genome Atlas database. The relationship between clinical features and AGGF1 expression was analyzed by Wilcoxon test. Further validation explorations were carried out using online database Oncomine. The diagnostic receiv- er operating characteristic curves of AGGF1 and alpha-fetoprotein were compared to examine the diagnostic efficacy of AGGF1. -

Zimmer Cell Calcium 2013 Mammalian S100 Evolution.Pdf
Cell Calcium 53 (2013) 170–179 Contents lists available at SciVerse ScienceDirect Cell Calcium jo urnal homepage: www.elsevier.com/locate/ceca Evolution of the S100 family of calcium sensor proteins a,∗ b b,1 b Danna B. Zimmer , Jeannine O. Eubanks , Dhivya Ramakrishnan , Michael F. Criscitiello a Center for Biomolecular Therapeutics and Department of Biochemistry & Molecular Biology, University of Maryland School of Medicine, 108 North Greene Street, Baltimore, MD 20102, United States b Comparative Immunogenetics Laboratory, Department of Veterinary Pathobiology, College of Veterinary Medicine & Biomedical Sciences, Texas A&M University, College Station, TX 77843-4467, United States a r t i c l e i n f o a b s t r a c t 2+ Article history: The S100s are a large group of Ca sensors found exclusively in vertebrates. Transcriptomic and genomic Received 4 October 2012 data from the major radiations of mammals were used to derive the evolution of the mammalian Received in revised form 1 November 2012 S100s genes. In human and mouse, S100s and S100 fused-type proteins are in a separate clade from Accepted 3 November 2012 2+ other Ca sensor proteins, indicating that an ancient bifurcation between these two gene lineages Available online 14 December 2012 has occurred. Furthermore, the five genomic loci containing S100 genes have remained largely intact during the past 165 million years since the shared ancestor of egg-laying and placental mammals. Keywords: Nonetheless, interesting births and deaths of S100 genes have occurred during mammalian evolution. Mammals The S100A7 loci exhibited the most plasticity and phylogenetic analyses clarified relationships between Phylogenetic analyses the S100A7 proteins encoded in the various mammalian genomes.