A Novel AGGF1-Pdgfrb Fusion in Pediatric T-Cell Acute Lymphoblastic Leukemia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Aggf1 Attenuates Neuroinflammation and BBB Disruption Via PI3K/Akt/NF-Κb Pathway After Subarachnoid Hemorrhage in Rats
Zhu et al. Journal of Neuroinflammation (2018) 15:178 https://doi.org/10.1186/s12974-018-1211-8 RESEARCH Open Access Aggf1 attenuates neuroinflammation and BBB disruption via PI3K/Akt/NF-κB pathway after subarachnoid hemorrhage in rats Qiquan Zhu1,2, Budbazar Enkhjargal2, Lei Huang2,4, Tongyu Zhang2, Chengmei Sun2, Zhiyi Xie2, Pei Wu2, Jun Mo2, Jiping Tang2, Zongyi Xie1* and John H. Zhang2,3,4* Abstract Background: Neuroinflammation and blood-brain barrier (BBB) disruption are two critical mechanisms of subarachnoid hemorrhage (SAH)-induced brain injury, which are closely related to patient prognosis. Recently, angiogenic factor with G-patch and FHA domain 1 (Aggf1) was shown to inhibit inflammatory effect and preserve vascular integrity in non-nervous system diseases. This study aimed to determine whether Aggf1 could attenuate neuroinflammation and preserve BBB integrity after experimental SAH, as well as the underlying mechanisms of its protective roles. Methods: Two hundred forty-nine male Sprague-Dawley rats were subjected to the endovascular perforation model of SAH. Recombinant human Aggf1 (rh-Aggf1) was administered intravenously via tail vein injection at 1 h after SAH induction. To investigate the underlying neuroprotection mechanism, Aggf1 small interfering RNA (Aggf1 siRNA) and PI3K-specific inhibitor LY294002 were administered through intracerebroventricular (i.c.v.) before SAH induction. SAH grade, neurological score, brain water content, BBB permeability, Western blot, and immunohistochemistry were performed. Results: Expression of endogenous Aggf1 was markedly increased after SAH. Aggf1 was primarily expressed in endothelial cells and astrocytes, as well as microglia after SAH. Administration of rh-Aggf1 significantly reduced brain water content and BBB permeability, decreased the numbers of infiltrating neutrophils, and activated microglia in the ipsilateral cerebral cortex following SAH. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -
Pancancer Progression Human Vjune2017
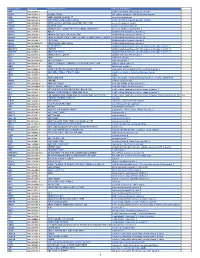
Gene Symbol Accession Alias/Prev Symbol Official Full Name AAMP NM_001087.3 - angio-associated, migratory cell protein ABI3BP NM_015429.3 NESHBP|TARSH ABI family, member 3 (NESH) binding protein ACHE NM_000665.3 ACEE|ARACHE|N-ACHE|YT acetylcholinesterase ACTG2 NM_001615.3 ACT|ACTA3|ACTE|ACTL3|ACTSG actin, gamma 2, smooth muscle, enteric ACVR1 NM_001105.2 ACTRI|ACVR1A|ACVRLK2|ALK2|FOP|SKR1|TSRI activin A receptor, type I ACVR1C NM_145259.2 ACVRLK7|ALK7 activin A receptor, type IC ACVRL1 NM_000020.1 ACVRLK1|ALK-1|ALK1|HHT|HHT2|ORW2|SKR3|TSR-I activin A receptor type II-like 1 ADAM15 NM_207195.1 MDC15 ADAM metallopeptidase domain 15 ADAM17 NM_003183.4 ADAM18|CD156B|CSVP|NISBD|TACE ADAM metallopeptidase domain 17 ADAM28 NM_014265.4 ADAM 28|ADAM23|MDC-L|MDC-Lm|MDC-Ls|MDCL|eMDC II|eMDCII ADAM metallopeptidase domain 28 ADAM8 NM_001109.4 CD156|MS2 ADAM metallopeptidase domain 8 ADAM9 NM_001005845.1 CORD9|MCMP|MDC9|Mltng ADAM metallopeptidase domain 9 ADAMTS1 NM_006988.3 C3-C5|METH1 ADAM metallopeptidase with thrombospondin type 1 motif, 1 ADAMTS12 NM_030955.2 PRO4389 ADAM metallopeptidase with thrombospondin type 1 motif, 12 ADAMTS8 NM_007037.4 ADAM-TS8|METH2 ADAM metallopeptidase with thrombospondin type 1 motif, 8 ADAP1 NM_006869.2 CENTA1|GCS1L|p42IP4 ArfGAP with dual PH domains 1 ADD1 NM_001119.4 ADDA adducin 1 (alpha) ADM2 NM_001253845.1 AM2|dJ579N16.4 adrenomedullin 2 ADRA2B NM_000682.4 ADRA2L1|ADRA2RL1|ADRARL1|ALPHA2BAR|alpha-2BAR adrenoceptor alpha 2B AEBP1 NM_001129.3 ACLP AE binding protein 1 AGGF1 NM_018046.3 GPATC7|GPATCH7|HSU84971|HUS84971|VG5Q -

A Genome-Wide Library of MADM Mice for Single-Cell Genetic Mosaic Analysis
bioRxiv preprint doi: https://doi.org/10.1101/2020.06.05.136192; this version posted June 6, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Contreras et al., A Genome-wide Library of MADM Mice for Single-Cell Genetic Mosaic Analysis Ximena Contreras1, Amarbayasgalan Davaatseren1, Nicole Amberg1, Andi H. Hansen1, Johanna Sonntag1, Lill Andersen2, Tina Bernthaler2, Anna Heger1, Randy Johnson3, Lindsay A. Schwarz4,5, Liqun Luo4, Thomas Rülicke2 & Simon Hippenmeyer1,6,# 1 Institute of Science and Technology Austria, Am Campus 1, 3400 Klosterneuburg, Austria 2 Institute of Laboratory Animal Science, University of Veterinary Medicine Vienna, Vienna, Austria 3 Department of Biochemistry and Molecular Biology, University of Texas, Houston, TX 77030, USA 4 HHMI and Department of Biology, Stanford University, Stanford, CA 94305, USA 5 Present address: St. Jude Children’s Research Hospital, Memphis, TN 38105, USA 6 Lead contact #Correspondence and requests for materials should be addressed to S.H. ([email protected]) 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.06.05.136192; this version posted June 6, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Contreras et al., SUMMARY Mosaic Analysis with Double Markers (MADM) offers a unique approach to visualize and concomitantly manipulate genetically-defined cells in mice with single-cell resolution. -

Genetic Mosaic Dissection of Lis1 and Ndel1 in Neuronal Migration
Neuron Article Genetic Mosaic Dissection of Lis1 and Ndel1 in Neuronal Migration Simon Hippenmeyer,1,* Yong Ha Youn,2 Hyang Mi Moon,2,3 Kazunari Miyamichi,1 Hui Zong,1,5 Anthony Wynshaw-Boris,2,4 and Liqun Luo1,* 1Howard Hughes Medical Institute and Department of Biology, Stanford University, Stanford, CA 94305, USA 2Department of Pediatrics and Institute for Human Genetics 3Biomedical Sciences Graduate Program 4Eli and Edythe Broad Center of Regeneration Medicine and Stem Cell Research University of California, San Francisco School of Medicine, San Francisco, CA 94143, USA 5Institute of Molecular Biology, University of Oregon, Eugene, OR 97403, USA *Correspondence: [email protected] (S.H.), [email protected] (L.L.) DOI 10.1016/j.neuron.2010.09.027 SUMMARY studied. Cortical layering occurs in an ‘‘inside-out’’ fashion whereby earlier born neurons occupy deep layers and succes- Coordinated migration of newly born neurons to their sively later born neurons settle in progressively upper layers (An- prospective target laminae is a prerequisite for neural gevine and Sidman, 1961; Rakic, 1974). Upon radial glia progen- circuit assembly in the developing brain. The evolu- itor cell (RGPC)-mediated neurogenesis, newborn migrating tionarily conserved LIS1/NDEL1 complex is essential cortical projection neurons are bipolar-shaped in the ventricular for neuronal migration in the mammalian cerebral zone (VZ) but then convert to a multipolar morphology within the cortex. The cytoplasmic nature of LIS1 and NDEL1 subventricular zone (SVZ) and migrate into the intermediate zone (IZ). A switch from the multipolar state back to a bipolar proteins suggest that they regulate neuronal migra- morphology precedes radial glia-guided locomotion of projec- tion cell autonomously. -

Activation of Aurora-A Is Essential for Neuronal Migration Via Modulation of Microtubule Organization
11050 • The Journal of Neuroscience, August 8, 2012 • 32(32):11050–11066 Cellular/Molecular Activation of Aurora-A Is Essential for Neuronal Migration via Modulation of Microtubule Organization Takako Takitoh,1 Kanako Kumamoto,1 Chen-Chi Wang,2,4 Makoto Sato,2,3,4 Shiori Toba,1 Anthony Wynshaw-Boris,5 and Shinji Hirotsune1 1Department of Genetic Disease Research, Osaka City University Graduate School of Medicine, Osaka 545-8585, Japan, 2Division of Cell Biology and Neuroscience, Department of Morphological and Physiological Sciences, Faculty of Medical Sciences, University of Fukui, 3Child Development Research Center, Graduate School of Medical Sciences, University of Fukui, 4Research and Education Program for Life Science, University of Fukui, Fukui 910-1193, Japan, and 5Department of Pediatrics and Institute for Human Genetics, University of California, San Francisco, School of Medicine, San Francisco, California 94143 Neuronal migration is a critical feature to ensure proper location and wiring of neurons during cortical development. Postmitotic neurons migrate from the ventricular zone into the cortical plate to establish neuronal lamina in an “inside-out” gradient of maturation. Here, we report that the mitotic kinase Aurora-A is critical for the regulation of microtubule organization during neuronal migration via an Aurora-A–NDEL1 pathway in the mouse. Suppression of Aurora-A activity by inhibitors or siRNA resulted in severe impairment of neuronal migration of granular neurons. In addition, in utero injection of the Aurora-A kinase-dead mutant provoked defective migra- tion of cortical neurons. Furthermore, we demonstrated that suppression of Aurora-A impaired microtubule modulation in migrating neurons. Interestingly, suppression of CDK5 by an inhibitor or siRNA reduced Aurora-A activity and NDEL1 phosphorylation by Aurora-A, which led to defective neuronal migration. -
Protocol Booklet
OmniKine™ Human TWEAK Colorimetric ELISA Kit Catalog #: OK-0169 Detection and Quantification of Human TWEAK Concentrations in Cell Lysates, Sera and Plasma. Please read the provided manual as suggested experimental protocols may have changed. Research Purposes Only. Not Intended for Diagnostic or Clinical Procedures. CONTENTS PAGE Introduction………………………………………………..…………….………..3 Assay Principles……………………………………………………….…………4 Assay Format………………………………………………………………..……5 Assay Restrictions……………………………………………………….……….6 Materials Included……………………………………………….……………….6 Additional Materials Required…………………………………………….…….7 Health and Safety Precautions…………………………………………….…...7 Storage Information………………………………………………………….…..8 Sample Preparation and Storage……………………………………………….9 Sample Experiment Layout…………………………………………………....10 Immunoassay Protocol……………………………………….…………….…..11 Summarized Protocol………………………………………………………......16 Sensitivity………………………………………………………………………..17 Cross Reactivity and Specificity……………………………………….…...…17 Technical Support……………………………………………….……………...18 ELISA Plate Template……………………………………………………..…...19 Notes…………………………………………………………….……………….20 OmniKine™ | Human TWEAK | 2 INTRODUCTION Human TWEAK or TNF-Related Weak Inducer of Apoptosis, also known as the APO3 Ligand, is a 249 amino acid cytokine protein that belongs to the tumor necrosis factor ligand superfamily. Encoded from the TNFSF12 gene located at locus 17p13 on chromosome 17, TWEAK is a ligand for the FN14/TWEAK receptor and has overlapping signaling functions with TNF, but displays a much wider tissue -

Forschungsbericht Science Report
FORSCHUNGSBERICHT SCIENCE REPORT2017/2018 ST. ANNA KINDERKREBSFORSCHUNG ST. ANNA CHILDREN’S CANCER RESEARCH INSTITUTE TUMOR BIOLOGY Understanding tumor heterogeneity and relapse in neuroblastoma patients to allow adequate treatment options. MOLECULAR MICROBIOLOGY LCH BIOLOGY Clinically important Targeted resistant mutations in Philadelphia inhibition chromosome-positive leukemias. of the MAPK pathway leads to a STUDIES & STATISTICS rapid and sustained clinical response in severe multisystem LCH. Busulfan and melphalan is considered standard high-dose chemotherapy for high-risk neuroblastoma. GENETICS OF LEUKEMIAS A novel genetic MOLECULAR BIOLOGY OF SOLID TUMORS subtype of leukemia. Understanding mechanisms EPIGENOME-BASED PRECISION MEDICINE of tumor cell plasticity EPIGENETIC and its role in diversity in Ewing sarcoma metastasis. Ewing sarcoma. MORE SCIENCE REPORTS INSIDE >>> [ 06 ] Forschungsbericht St. Anna Kinderkrebsforschung | Science Report St. Anna Children’s Cancer Research Institute Inhalt Einleitung Vorwort des Institutsleiters 10 Vorwort des wissenschaftlichen Direktors 12 30 Jahre – unseren Spendern sei Dank! 14 Daten & Fakten Kompetitive Drittmittel 2018 20 Zuweisung der Geldmittel 2018 20 Finanzierung 2018 20 Nationen 21 Personelle Zusammensetzung 21 PatientInnenaufkommen im S2IRP 22 2-Jahres-Überlebensrate krebskranker Kinder 23 5-Jahres-Überlebensrate krebskranker Kinder 24 Forschungsnetzwerke 26 Inhalt Forschungsbericht I St. Anna Kinderkrebsforschung | Science Report St. Anna Cancer Research Institute [ 07 ] Science -

Lis1 and Ndel1 Influence the Timing of Nuclear Envelope Breakdown in Neural Stem Cells
University of South Carolina Scholar Commons Faculty Publications Biological Sciences, Department of 9-22-2008 Lis1 and Ndel1 Influence the Timing of Nuclear Envelope Breakdown in Neural Stem Cells Sachin Hebbar University of South Carolina - Columbia Mariano T. Mesngon University of South Carolina - Columbia Aimee M. Guillotte University of South Carolina - Columbia Bhavim Desai University of South Carolina - Columbia, [email protected] Ramses Ayala Mass General Institute for Neurodegenerative Disease See next page for additional authors Follow this and additional works at: https://scholarcommons.sc.edu/biol_facpub Part of the Biology Commons Publication Info The Journal of Cell Biology, Volume 182, Issue 6, 2008, pages 1063-1071. © 2008, the authors. Originally published in the Journal of Cell Biology by the Rockefeller University Press. This Article is brought to you by the Biological Sciences, Department of at Scholar Commons. It has been accepted for inclusion in Faculty Publications by an authorized administrator of Scholar Commons. For more information, please contact [email protected]. Author(s) Sachin Hebbar, Mariano T. Mesngon, Aimee M. Guillotte, Bhavim Desai, Ramses Ayala, and Deanna S. Smith This article is available at Scholar Commons: https://scholarcommons.sc.edu/biol_facpub/58 Published September 22, 2008 JCB: REPORT Lis1 and Ndel1 infl uence the timing of nuclear envelope breakdown in neural stem cells Sachin Hebbar , 1 Mariano T. Mesngon , 1 Aimee M. Guillotte , 1 Bhavim Desai , 1 Ramses Ayala , 2 and Deanna S. Smith 1 1 Department of Biological Sciences, University of South Carolina, Columbia, SC 29208 2 Neurology Department, Mass General Institute for Neurodegenerative Disease, Charlestown, MA 02120 is1 and Ndel1 are essential for animal development. -

Current Treatment of Juvenile Myelomonocytic Leukemia
Journal of Clinical Medicine Review Current Treatment of Juvenile Myelomonocytic Leukemia Christina Mayerhofer 1 , Charlotte M. Niemeyer 1,2 and Christian Flotho 1,2,* 1 Division of Pediatric Hematology and Oncology, Department of Pediatrics and Adolescent Medicine, Medical Center, Faculty of Medicine, University of Freiburg, 79106 Freiburg, Germany; [email protected] (C.M.); [email protected] (C.M.N.) 2 German Cancer Consortium (DKTK), 79106 Freiburg, Germany * Correspondence: christian.fl[email protected] Abstract: Juvenile myelomonocytic leukemia (JMML) is a rare pediatric leukemia characterized by mutations in five canonical RAS pathway genes. The diagnosis is made by typical clinical and hematological findings associated with a compatible mutation. Although this is sufficient for clinical decision-making in most JMML cases, more in-depth analysis can include DNA methylation class and panel sequencing analysis for secondary mutations. NRAS-initiated JMML is heterogeneous and adequate management ranges from watchful waiting to allogeneic hematopoietic stem cell transplan- tation (HSCT). Upfront azacitidine in KRAS patients can achieve long-term remissions without HSCT; if HSCT is required, a less toxic preparative regimen is recommended. Germline CBL patients often experience spontaneous resolution of the leukemia or exhibit stable mixed chimerism after HSCT. JMML driven by PTPN11 or NF1 is often rapidly progressive, requires swift HSCT and may benefit from pretransplant therapy with azacitidine. Because graft-versus-leukemia alloimmunity is central to cure high risk patients, the immunosuppressive regimen should be discontinued early after HSCT. Keywords: juvenile myelomonocytic leukemia; RAS signaling; hematopoietic stem cell transplantation; 5-azacitidine; myelodysplastic/myeloproliferative disorders; targeted therapy Citation: Mayerhofer, C.; Niemeyer, C.M.; Flotho, C. -

CRL5-Dependent Regulation of the Small Gtpases ARL4C and ARF6 Controls Hippocampal Morphogenesis
CRL5-dependent regulation of the small GTPases ARL4C and ARF6 controls hippocampal morphogenesis Jisoo S. Hana,1, Keiko Hinoa,1, Wenzhe Lia, Raenier V. Reyesa, Cesar P. Canalesa,2, Adam M. Miltnera, Yasmin Haddadia, Junqing Sunb, Chao-Yin Chenb, Anna La Torrea, and Sergi Simóa,3 aDepartment of Cell Biology and Human Anatomy, University of California, Davis, CA 95616; and bDepartment of Pharmacology, University of California, Davis, CA 95616 Edited by Mary E. Hatten, Rockefeller University, New York, NY, and approved August 3, 2020 (received for review February 14, 2020) The small GTPase ARL4C participates in the regulation of cell migra- Importantly, CRL5 substrate adaptors are dynamically regulated tion, cytoskeletal rearrangements, and vesicular trafficking in epithe- during development, directing CRL5 activity to specific substrates lial cells. The ARL4C signaling cascade starts by the recruitment of the at different times and areas in the CNS (19). In the neocortex, ARF–GEF cytohesins to the plasma membrane, which, in turn, bind CRL5 opposes projection neuron migration by down-regulating and activate the small GTPase ARF6. However, the role of ARL4C– the Reelin/DAB1 signaling pathway as migrating projection neu- cytohesin–ARF6 signaling during hippocampal development remains rons reach the top of the cortical plate (18, 20, 21). In the CNS, elusive. Here, we report that the E3 ubiquitin ligase Cullin 5/RBX2 Reelin/DAB1 signaling participates in several developmental (CRL5) controls the stability of ARL4C and its signaling effectors to processes, including neuron migration, dendritogenesis, axo- regulate hippocampal morphogenesis. Both RBX2 knockout and genesis, and synaptogenesis (22–24). Moreover, CRL5 also con- Cullin 5 knockdown cause hippocampal pyramidal neuron mislocali- trols levels of the tyrosine kinase FYN, which exerts important zation and development of multiple apical dendrites. -

Elevated Expression of AGGF1 Predicts Poor Prognosis and Promotes the Metastasis of Colorectal Cancer
Elevated expression of AGGF1 predicts poor prognosis and promotes the metastasis of colorectal cancer Xin Zhang Zhejiang Provincial People's Hospital Huimin Sun Weifang People's Hospital Wanyuan Chen Zhejiang Provincial People's Hospital Xianglei He ( [email protected] ) Zhejiang Provincial People's Hospital https://orcid.org/0000-0002-7685-3451 Research article Keywords: Colorectal cancer; AGGF1; Prognosis; Metastasis Posted Date: October 25th, 2019 DOI: https://doi.org/10.21203/rs.2.14319/v2 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on December 27th, 2019. See the published version at https://doi.org/10.1186/s12885-019-6474-7. Page 1/15 Abstract Abstract Background: Angiogenic factor with G-patch and FHA domains 1 (AGGF1) can promote angiogenesis and increasing evidence has highlighted the important roles of AGGF1 in tumorigenesis. However, the expression patterns as well as the biological functions of AGGF1 in colorectal cancer (CRC) remain to be established. The purpose of the present study is therefore to identify the effect of AGGF1 on prognosis and metastasis in CRC patients. Methods: The expression level of AGGF1 in CRC was examined by qPCR, western blot and immunohistochemistry in a tissue microarray containing 101 CRC specimens. And the effect of AGGF1 on CRC cell malignance was investigated in our established stable AGGF1 upregulated and knockdown CRC cell lines. Results: The expression level of AGGF1 in CRC tissue was not signicantly different to that in adjacent normal mucosa at the mRNA level.