Gene Expression Signature Discriminates Sporadic from Post-Radiotherapy-Induced Thyroid Tumors
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Aggf1 Attenuates Neuroinflammation and BBB Disruption Via PI3K/Akt/NF-Κb Pathway After Subarachnoid Hemorrhage in Rats
Zhu et al. Journal of Neuroinflammation (2018) 15:178 https://doi.org/10.1186/s12974-018-1211-8 RESEARCH Open Access Aggf1 attenuates neuroinflammation and BBB disruption via PI3K/Akt/NF-κB pathway after subarachnoid hemorrhage in rats Qiquan Zhu1,2, Budbazar Enkhjargal2, Lei Huang2,4, Tongyu Zhang2, Chengmei Sun2, Zhiyi Xie2, Pei Wu2, Jun Mo2, Jiping Tang2, Zongyi Xie1* and John H. Zhang2,3,4* Abstract Background: Neuroinflammation and blood-brain barrier (BBB) disruption are two critical mechanisms of subarachnoid hemorrhage (SAH)-induced brain injury, which are closely related to patient prognosis. Recently, angiogenic factor with G-patch and FHA domain 1 (Aggf1) was shown to inhibit inflammatory effect and preserve vascular integrity in non-nervous system diseases. This study aimed to determine whether Aggf1 could attenuate neuroinflammation and preserve BBB integrity after experimental SAH, as well as the underlying mechanisms of its protective roles. Methods: Two hundred forty-nine male Sprague-Dawley rats were subjected to the endovascular perforation model of SAH. Recombinant human Aggf1 (rh-Aggf1) was administered intravenously via tail vein injection at 1 h after SAH induction. To investigate the underlying neuroprotection mechanism, Aggf1 small interfering RNA (Aggf1 siRNA) and PI3K-specific inhibitor LY294002 were administered through intracerebroventricular (i.c.v.) before SAH induction. SAH grade, neurological score, brain water content, BBB permeability, Western blot, and immunohistochemistry were performed. Results: Expression of endogenous Aggf1 was markedly increased after SAH. Aggf1 was primarily expressed in endothelial cells and astrocytes, as well as microglia after SAH. Administration of rh-Aggf1 significantly reduced brain water content and BBB permeability, decreased the numbers of infiltrating neutrophils, and activated microglia in the ipsilateral cerebral cortex following SAH. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

Supplementary Information Material and Methods
MCT-11-0474 BKM120: a potent and specific pan-PI3K inhibitor Supplementary Information Material and methods Chemicals The EGFR inhibitor NVP-AEE788 (Novartis), the Jak inhibitor I (Merck Calbiochem, #420099) and anisomycin (Alomone labs, # A-520) were prepared as 50 mM stock solutions in 100% DMSO. Doxorubicin (Adriablastin, Pfizer), EGF (Sigma Ref: E9644), PDGF (Sigma, Ref: P4306) and IL-4 (Sigma, Ref: I-4269) stock solutions were prepared as recommended by the manufacturer. For in vivo administration: Temodal (20 mg Temozolomide capsules, Essex Chemie AG, Luzern) was dissolved in 4 mL KZI/glucose (20/80, vol/vol); Taxotere was bought as 40 mg/mL solution (Sanofi Aventis, France), and prepared in KZI/glucose. Antibodies The primary antibodies used were as follows: anti-S473P-Akt (#9271), anti-T308P-Akt (#9276,), anti-S9P-GSK3β (#9336), anti-T389P-p70S6K (#9205), anti-YP/TP-Erk1/2 (#9101), anti-YP/TP-p38 (#9215), anti-YP/TP-JNK1/2 (#9101), anti-Y751P-PDGFR (#3161), anti- p21Cip1/Waf1 (#2946), anti-p27Kip1 (#2552) and anti-Ser15-p53 (#9284) antibodies were from Cell Signaling Technologies; anti-Akt (#05-591), anti-T32P-FKHRL1 (#06-952) and anti- PDGFR (#06-495) antibodies were from Upstate; anti-IGF-1R (#SC-713) and anti-EGFR (#SC-03) antibodies were from Santa Cruz; anti-GSK3α/β (#44610), anti-Y641P-Stat6 (#611566), anti-S1981P-ATM (#200-301), anti-T2609 DNA-PKcs (#GTX24194) and anti- 1 MCT-11-0474 BKM120: a potent and specific pan-PI3K inhibitor Y1316P-IGF-1R were from Bio-Source International, Becton-Dickinson, Rockland, GenTex and internal production, respectively. The 4G10 antibody was from Millipore (#05-321MG). -

Poster Authors: Martin Lee Miller, Søren Brunak, Lars Juhl Jensen, Michael B
A Sequence-Specificity Atlas of the Kinase World CK1 family NEK2 Negative Atypical S TGFbR2 S D F T EIF2AK2 YS SY A EE S F EDDETDG S DTTYGA 0 1 2 3 4 5 6 7 -7 -6 -5 -4 -3 -2 -1 L I M S TR FWMW VS W G LT Y H T 0 1 2 3 4 5 6 7 -7 -6 -5 -4 -3 -2 -1 E S R CK1gamma3 CK1gamma1 CK1gamma2 R K T TS DE CK1epsilon S CK1alpha2 NND QRN S KKS M CQ CK1alpha 0 1 2 3 4 5 6 7 O -6 -5 -4 -3 -2 -1 T CK1delta -7 V D KRT R D E RL D R SEL T PTTS LD T S S L S SK LM PLP LS E E P A E K RG LDLF Y G V N G GR L I A T LV VAY TT TTBK2 KR I T RVFS I RE KA TDD RS KQ KM D EE G G BUBR1 TTBK1 VRK2 VRK1 N RE P D SgK396 VRK3 MPKRT F NFNMGPM SgK196 P I GMVHG KYL I MEL SgK493 Positive 0 SgK110 Haspin S BUB1 -7 -6 -5 -4 -3 -2 -1 SgK069 +3 +4 +5 +6 +7 +1 +2 SgK223 SgK269 Wnk2 Wnk4 Wnk3 NRBP1 ATM/ATR NRBP2 Wnk1 SCYL2 SCYL1 SCYL3 PIK3R4 Slob SgK424 SgK307 PINK1 SBK SgK496 MOS TBCK PBK CYGF CDC7 CYGD HSER NEK1 ANPb Proline NEK5 ANPa ILK NEK3 BMPR2 NEK11NEK4 MISR2 TGFbR2 ACTR2 NEK2 ACTR2B ALK2 NEK9 ALK1 NEK8 BMPR1B NEK6 BMPR1A NEK10NEK7 ALK7 TGFbR1 ALK4 AAK1 MLKL IRAK4 S S MPSK1 BIKE IRAK2 E Q EIF2AK2 S D G S E IRAK1 ES A S PS I SS GAK TQL PL SQ DL Syk family S VP Tec family P D E IRAK3 EphB3 L T GCN2 1 TESK2 0 PEK TESK1 -7 -6 -5 -4 -3 -2 -1 S +1 +2 +3 +4 +5 +6 +7 Q LIMK1 Wee1B LIMK2 mTOR LRRK2 HRI LRRK1 Wee1 RIPK1 MYT1 RIPK3 RNAseL RIPK2 IRE1 ANKRD3 IRE2 SgK288 KSR2 SgK071 KSR1 D E V L P KIS ARAF EV P S D R TTK E D D R VE AD VS A EE D DG V SSDDE EY NP R BRAF D V L E M ATPVD CLIK1LCLIK1 S EES E YE L LEE QLT EN PD E A L D T I SP NQ DG ANSS D DEE S DLL MS G PS P K A SD TEN T NGLKND -
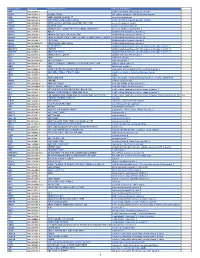
Pancancer Progression Human Vjune2017
Gene Symbol Accession Alias/Prev Symbol Official Full Name AAMP NM_001087.3 - angio-associated, migratory cell protein ABI3BP NM_015429.3 NESHBP|TARSH ABI family, member 3 (NESH) binding protein ACHE NM_000665.3 ACEE|ARACHE|N-ACHE|YT acetylcholinesterase ACTG2 NM_001615.3 ACT|ACTA3|ACTE|ACTL3|ACTSG actin, gamma 2, smooth muscle, enteric ACVR1 NM_001105.2 ACTRI|ACVR1A|ACVRLK2|ALK2|FOP|SKR1|TSRI activin A receptor, type I ACVR1C NM_145259.2 ACVRLK7|ALK7 activin A receptor, type IC ACVRL1 NM_000020.1 ACVRLK1|ALK-1|ALK1|HHT|HHT2|ORW2|SKR3|TSR-I activin A receptor type II-like 1 ADAM15 NM_207195.1 MDC15 ADAM metallopeptidase domain 15 ADAM17 NM_003183.4 ADAM18|CD156B|CSVP|NISBD|TACE ADAM metallopeptidase domain 17 ADAM28 NM_014265.4 ADAM 28|ADAM23|MDC-L|MDC-Lm|MDC-Ls|MDCL|eMDC II|eMDCII ADAM metallopeptidase domain 28 ADAM8 NM_001109.4 CD156|MS2 ADAM metallopeptidase domain 8 ADAM9 NM_001005845.1 CORD9|MCMP|MDC9|Mltng ADAM metallopeptidase domain 9 ADAMTS1 NM_006988.3 C3-C5|METH1 ADAM metallopeptidase with thrombospondin type 1 motif, 1 ADAMTS12 NM_030955.2 PRO4389 ADAM metallopeptidase with thrombospondin type 1 motif, 12 ADAMTS8 NM_007037.4 ADAM-TS8|METH2 ADAM metallopeptidase with thrombospondin type 1 motif, 8 ADAP1 NM_006869.2 CENTA1|GCS1L|p42IP4 ArfGAP with dual PH domains 1 ADD1 NM_001119.4 ADDA adducin 1 (alpha) ADM2 NM_001253845.1 AM2|dJ579N16.4 adrenomedullin 2 ADRA2B NM_000682.4 ADRA2L1|ADRA2RL1|ADRARL1|ALPHA2BAR|alpha-2BAR adrenoceptor alpha 2B AEBP1 NM_001129.3 ACLP AE binding protein 1 AGGF1 NM_018046.3 GPATC7|GPATCH7|HSU84971|HUS84971|VG5Q -

Article Reference
Article Phosphorylation by NLK inhibits YAP‐14‐3‐3‐interactions and induces its nuclear localization MOON, Sungho, et al. Reference MOON, Sungho, et al. Phosphorylation by NLK inhibits YAP‐14‐3‐3‐interactions and induces its nuclear localization. EMBO Reports, 2017, vol. 18, no. 1, p. 61-71 PMID : 27979972 DOI : 10.15252/embr.201642683 Available at: http://archive-ouverte.unige.ch/unige:112477 Disclaimer: layout of this document may differ from the published version. 1 / 1 Published online: December 15, 2016 Scientific Report Phosphorylation by NLK inhibits YAP-14-3-3- interactions and induces its nuclear localization Sungho Moon1,† , Wantae Kim1,†, Soyoung Kim1, Youngeun Kim1, Yonghee Song1, Oleksii Bilousov2, Jiyoung Kim1, Taebok Lee1, Boksik Cha1, Minseong Kim1, Hanjun Kim1, Vladimir L Katanaev2,3,* & Eek-hoon Jho1,** Abstract tissue homeostasis have become a long-standing topic of interest. As loss of the organ size control is linked to many human diseases, includ- Hippo signaling controls organ size by regulating cell proliferation ing cancer and degenerative diseases, regulation of the organ size and apoptosis. Yes-associated protein (YAP) is a key downstream could be an attractive therapeutic strategy. Recently, Hippo signaling effector of Hippo signaling, and LATS-mediated phosphorylation of has been identified as a major signaling pathway to control the organ YAP at Ser127 inhibits its nuclear localization and transcriptional size; dysregulation of this pathway results in aberrant growth [1]. activity. Here, we report that Nemo-like kinase (NLK) phosphory- The Hippo pathway is evolutionarily conserved from nematodes lates YAP at Ser128 both in vitro and in vivo, which blocks interac- to humans and controls a variety of cellular processes, such as cell tion with 14-3-3 and enhances its nuclear localization. -

Table S1. Identified Proteins with Exclusive Expression in Cerebellum of Rats of Control, 10Mg F/L and 50Mg F/L Groups
Table S1. Identified proteins with exclusive expression in cerebellum of rats of control, 10mg F/L and 50mg F/L groups. Accession PLGS Protein Name Group IDa Score Q3TXS7 26S proteasome non-ATPase regulatory subunit 1 435 Control Q9CQX8 28S ribosomal protein S36_ mitochondrial 197 Control P52760 2-iminobutanoate/2-iminopropanoate deaminase 315 Control Q60597 2-oxoglutarate dehydrogenase_ mitochondrial 67 Control P24815 3 beta-hydroxysteroid dehydrogenase/Delta 5-->4-isomerase type 1 84 Control Q99L13 3-hydroxyisobutyrate dehydrogenase_ mitochondrial 114 Control P61922 4-aminobutyrate aminotransferase_ mitochondrial 470 Control P10852 4F2 cell-surface antigen heavy chain 220 Control Q8K010 5-oxoprolinase 197 Control P47955 60S acidic ribosomal protein P1 190 Control P70266 6-phosphofructo-2-kinase/fructose-2_6-bisphosphatase 1 113 Control Q8QZT1 Acetyl-CoA acetyltransferase_ mitochondrial 402 Control Q9R0Y5 Adenylate kinase isoenzyme 1 623 Control Q80TS3 Adhesion G protein-coupled receptor L3 59 Control B7ZCC9 Adhesion G-protein coupled receptor G4 139 Control Q6P5E6 ADP-ribosylation factor-binding protein GGA2 45 Control E9Q394 A-kinase anchor protein 13 60 Control Q80Y20 Alkylated DNA repair protein alkB homolog 8 111 Control P07758 Alpha-1-antitrypsin 1-1 78 Control P22599 Alpha-1-antitrypsin 1-2 78 Control Q00896 Alpha-1-antitrypsin 1-3 78 Control Q00897 Alpha-1-antitrypsin 1-4 78 Control P57780 Alpha-actinin-4 58 Control Q9QYC0 Alpha-adducin 270 Control Q9DB05 Alpha-soluble NSF attachment protein 156 Control Q6PAM1 Alpha-taxilin 161 -
Protocol Booklet
OmniKine™ Human TWEAK Colorimetric ELISA Kit Catalog #: OK-0169 Detection and Quantification of Human TWEAK Concentrations in Cell Lysates, Sera and Plasma. Please read the provided manual as suggested experimental protocols may have changed. Research Purposes Only. Not Intended for Diagnostic or Clinical Procedures. CONTENTS PAGE Introduction………………………………………………..…………….………..3 Assay Principles……………………………………………………….…………4 Assay Format………………………………………………………………..……5 Assay Restrictions……………………………………………………….……….6 Materials Included……………………………………………….……………….6 Additional Materials Required…………………………………………….…….7 Health and Safety Precautions…………………………………………….…...7 Storage Information………………………………………………………….…..8 Sample Preparation and Storage……………………………………………….9 Sample Experiment Layout…………………………………………………....10 Immunoassay Protocol……………………………………….…………….…..11 Summarized Protocol………………………………………………………......16 Sensitivity………………………………………………………………………..17 Cross Reactivity and Specificity……………………………………….…...…17 Technical Support……………………………………………….……………...18 ELISA Plate Template……………………………………………………..…...19 Notes…………………………………………………………….……………….20 OmniKine™ | Human TWEAK | 2 INTRODUCTION Human TWEAK or TNF-Related Weak Inducer of Apoptosis, also known as the APO3 Ligand, is a 249 amino acid cytokine protein that belongs to the tumor necrosis factor ligand superfamily. Encoded from the TNFSF12 gene located at locus 17p13 on chromosome 17, TWEAK is a ligand for the FN14/TWEAK receptor and has overlapping signaling functions with TNF, but displays a much wider tissue -

Androgen Receptor Modifications
Kennedy’s Disease Research at the Lim Lab - Signaling pathway modulating Androgen Receptor post-translational modifications and its clearance as well as their contribution to KD Janghoo Lim, Ph.D. Department of Genetics Department of Neuroscience Program in Cellular Neuroscience, Neurodegeneration and Repair Yale University School of Medicine Translational Neuroscience Neurodegenerative Diseases successful therapies? gene identification SBMA pre-clinical trials disease models drug discovery pathogenesis studies candidate targets for therapeutic intervention Basic Neuroscience Translational Neuroscience Neurodegenerative Diseases successful therapies? gene identification SBMA pre-clinical trials disease models drug discovery pathogenesis studies candidate targets for therapeutic intervention Basic Neuroscience Translational Neuroscience Neurodegenerative Diseases successful therapies? gene identification SBMA pre-clinical trials disease models drug discovery pathogenesis studies candidate targets for therapeutic intervention Basic Neuroscience Translational Neuroscience Neurodegenerative Diseases successful therapies? gene identification SBMA pre-clinical trials disease models drug discovery pathogenesis studies candidate targets for therapeutic intervention Basic Neuroscience Are there any good candidate targets for therapeutic intervention for SBMA? Are there any good candidate targets for therapeutic intervention for SBMA? Nemo-Like Kinase (NLK) Nemo-Like Kinase (NLK) . Conserved MAPK-like serine/threonine protein kinase Cargnello et -

Elevated Expression of AGGF1 Predicts Poor Prognosis and Promotes the Metastasis of Colorectal Cancer
Elevated expression of AGGF1 predicts poor prognosis and promotes the metastasis of colorectal cancer Xin Zhang Zhejiang Provincial People's Hospital Huimin Sun Weifang People's Hospital Wanyuan Chen Zhejiang Provincial People's Hospital Xianglei He ( [email protected] ) Zhejiang Provincial People's Hospital https://orcid.org/0000-0002-7685-3451 Research article Keywords: Colorectal cancer; AGGF1; Prognosis; Metastasis Posted Date: October 25th, 2019 DOI: https://doi.org/10.21203/rs.2.14319/v2 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on December 27th, 2019. See the published version at https://doi.org/10.1186/s12885-019-6474-7. Page 1/15 Abstract Abstract Background: Angiogenic factor with G-patch and FHA domains 1 (AGGF1) can promote angiogenesis and increasing evidence has highlighted the important roles of AGGF1 in tumorigenesis. However, the expression patterns as well as the biological functions of AGGF1 in colorectal cancer (CRC) remain to be established. The purpose of the present study is therefore to identify the effect of AGGF1 on prognosis and metastasis in CRC patients. Methods: The expression level of AGGF1 in CRC was examined by qPCR, western blot and immunohistochemistry in a tissue microarray containing 101 CRC specimens. And the effect of AGGF1 on CRC cell malignance was investigated in our established stable AGGF1 upregulated and knockdown CRC cell lines. Results: The expression level of AGGF1 in CRC tissue was not signicantly different to that in adjacent normal mucosa at the mRNA level. -

Nemo-Like Kinase in Development and Diseases: Insights from Mouse Studies
International Journal of Molecular Sciences Review Nemo-Like Kinase in Development and Diseases: Insights from Mouse Studies Renée Daams and Ramin Massoumi * Department of Laboratory Medicine, Translational Cancer Research, Faculty of Medicine, Lund University, 22381 Lund, Sweden; [email protected] * Correspondence: [email protected]; Tel.: +46-46-2226430 Received: 16 November 2020; Accepted: 1 December 2020; Published: 2 December 2020 Abstract: The Wnt signalling pathway is a central communication cascade between cells to orchestrate polarity and fate during development and adult tissue homeostasis in various organisms. This pathway can be regulated by different signalling molecules in several steps. One of the coordinators in this pathway is Nemo-like kinase (NLK), which is an atypical proline-directed serine/threonine mitogen-activated protein (MAP) kinase. Very recently, NLK was established as an essential regulator in different cellular processes and abnormal NLK expression was highlighted to affect the development and progression of various diseases. In this review, we focused on the recent discoveries by using NLK-deficient mice, which show a phenotype in the development and function of organs such as the lung, heart and skeleton. Furthermore, NLK could conduct the function and differentiation of cells from the immune system, in addition to regulating neurodegenerative diseases, such as Huntington’s disease and spinocerebellar ataxias. Overall, generations of NLK-deficient mice have taught us valuable lessons about the role of this kinase in certain diseases and development. Keywords: Nemo-like kinase (NLK); animal models; mice; development; immune system neuronal disorders 1. Introduction 1.1. Wnt Signalling Pathway The Wnt proteins consist of conserved, secreted glycoproteins harbouring essential roles in the mechanisms directing cell proliferation, cell polarity and cell fate determination during embryonic development, as well as adult tissue homeostasis in various organisms [1]. -

BMP Signaling in Vascular Biology and Dysfunction
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Lirias Accepted Manuscript Title: BMP signaling in vascular biology and dysfunction Author: Amaya Garc´ıa de Vinuesa Salim Abdelilah-Seyfried Petra Knaus An Zwijsen Sabine Bailly This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. BMP signaling in vascular biology and dysfunction Amaya García de Vinuesa1, Salim Abdelilah-Seyfried2,3, Petra Knaus4, An Zwijsen5,6*, Sabine Bailly7,8,9* 1Department of Molecular Cell Biology, Cancer Genomics Centre Netherlands, Leiden University Medical Center, Leiden, the Netherlands. 2Institute of Biochemistry and Biology, Potsdam University, Karl-Liebknecht-Straße 24- 25, D-14476 Potsdam, Germany. 3Institute of Molecular Biology, Hannover Medical School, Carl-Neuberg Straße 1, D- 30625 Hannover, Germany. 4Institute for Chemistry and Biochemistry, Freie Universitaet Berlin, Berlin, Germany. 5VIB Center for the Biology of Disease, Leuven, Belgium 6KU Leuven, Dept Human Genetics, Leuven, Belgium 7Institut National de la Santé et de la Recherche Médicale (INSERM, U1036), Grenoble, France F-38000 8Commissariat à l’Énergie