Medical Policy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Water Stream in Bidet Toilet Commode As A
Ann Colorectal Res. 2017 March; 5(1):e46479. doi: 10.5812/acr.46479. Published online 2017 March 25. Research Article Water Stream in Bidet Toilet Commode as a Cause of Anterior Anal Fissure: A Case-Control Study Pankaj Garg,1,2,* and Pratiksha Singh2 1Colorectal Surgery Division, Indus Super Specialty Hospital, Mohali, Punjab, India 2Garg Fistula Research Institute, Panchkula, Haryana, India *Corresponding author: Pankaj Garg, Garg Fistula Research Institute, 1042, Sector-15, Panchkula, Haryana, India. Tel: +91-9501011000, Fax: +91-1722594556, E-mail: [email protected] Received 2017 January 09; Revised 2017 February 06; Accepted 2017 March 08. Abstract Background: Water used as a single sharp stream in toilet commode for post defecation cleansing is a common practice in sev- eral countries across the globe including India. Repeated hitting of the anus by water stream could potentially cause injury to the anal canal epithelium and lead to development of fissure-in-ano. As the water stream is emanating from the backside of the toilet commode, the possible injury, if any, would be on the anterior anal canal. Objectives: The present study aimed at determining whether water stream usage in toilet commodes increased the incidence of anterior fissure-in-ano; this was determined by the incidence of anterior fissure-in-ano the study and control groups. Methods: All consecutive fissure-in-ano patients referring to a colorectal clinic from February 2012 to 2015 were included in the study. The patients were classified as a study group (who were using water stream for cleansing purposes in toilet commodes) and a control group (patients who were not using water stream). -

X-EFFECT® BOWL CLEANER Disinfects, Cleans, and Deodorizes with a Fresh Lavender Scent
X-EFFECT® BOWL CLEANER Disinfects, cleans, and deodorizes with a fresh lavender scent X-EFFECT Bowl Cleaner cleans and disinfects toilets, com- modes, and urinals. Bacteria and viruses found in public restrooms can cause odors and create an unsafe environment for building occupants. X-EFFECT Bowl Cleaner offers a con- venient and effective solution for removing bacteria and viruses while leaving a fresh lavender fragrance. For best results, use with common scent products like Airlift® Ultra-Fragrant Urinal Screens, Commode Clips, and Odor Eliminators. EPA Registration Number: 5741-18 Providing quality maintenance and chemical specialty solutions with unparalleled customer service since 1956 X-EFFECT® BOWL CLEANER FEATURES DIRECTIONS FOR USE • Ready-to-use disinfectant cleaner ONE-STEP DISINFECTING AND CLEANING TOILET • Kills the virus that causes COVID-191,2 BOWLS AND URINALS Remove visible soil before disinfection. Empty toilet bowl or urinal and ap- • Broad-spectrum, hospital-grade disinfectant ply product to exposed surfaces with a brush or swab mop. Brush or swab • Formulated for use in daily maintenance programs thoroughly, especially under the rim. Let stand for 10 minutes, then flush. ONE-STEP DISINFECTING CERAMIC TILE, PORCE- BENEFITS LAIN, SHOWER WALLS, FLOORS, AND OTHER HARD, • Cleans as it disinfects NON-POROUS SURFACES • Features a fresh lavender fragrance Remove visible soil before disinfection. Apply X-EFFECT Bowl Cleaner with a cloth, mop, sponge, or coarse sprayer. Treated surfaces must • Ready-to-use formula ensures proper ppm required for disinfection remain wet for 10 minutes. Rinse thoroughly with water. • Pre-labeled, pre-filled quarts offer the ultimate safety and convenience GENERAL DEODORIZING AND CLEANING 1 SARS-Related Coronavirus 2 Dilute X-EFFECT Bowl Cleaner 1:10 (12 oz/gal of water) for general 2 On hard, non-porous surfaces deodorizing and cleaning of hard, nonporous bathroom surfaces. -
Bedside Commode Chair
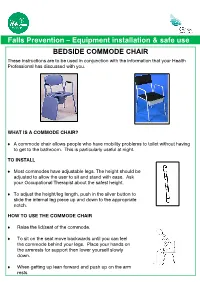
Falls Prevention – Equipment installation & safe use BEDSIDE COMMODE CHAIR These instructions are to be used in conjunction with the information that your Health Professional has discussed with you. WHAT IS A COMMODE CHAIR? A commode chair allows people who have mobility problems to toilet without having to get to the bathroom. This is particularly useful at night. TO INSTALL Most commodes have adjustable legs. The height should be adjusted to allow the user to sit and stand with ease. Ask your Occupational Therapist about the safest height. To adjust the height/leg length, push in the silver button to slide the internal leg piece up and down to the appropriate notch. HOW TO USE THE COMMODE CHAIR Raise the lid/seat of the commode. To sit on the seat move backwards until you can feel the commode behind your legs. Place your hands on the armrests for support then lower yourself slowly down. When getting up lean forward and push up on the arm rests PRECAUTIONS & SAFETY Ensure that the commode chair is stable on the floor and cannot slide or tip over Ensure legs of the commode chair are adjusted to the correct height Ensure the toilet paper is situated within easy reach Ensure the pan is emptied regularly Ensure there is adequate space around the commode chair to enable safe movement on, off & around the commode MAINTENANCE & CLEANING Ensure that you regularly clean the commode chair and bucket with a mild disinfectant. For a standard commode, lift the toilet seat and pick up the bucket using the handle. -

The LS600 Bariatric Toilet Lift
The LS600 Bariatric Toilet Lift The LS600 combines our breakthrough LiftTekTM Core Assistive Technology with bedside to bathroom flexibility to deliver the most advanced bariatric toilet transfer solution available for your safe patient handling and fall prevention programs. Product Highlights 650 lb. weight capacity Reduces the risk of staff and patient injury by delivering the hip, knee, and ankle joint “LiftSeat has significant support required during the sit-to-stand motion path implications for protecting healthcare Moves easily and locks in place to provide bedside and over-the-toilet assistance anywhere in your facility workers from musculoskeletal disorders Converts facility toilets to taller ADA height and increased weight rating without costly and preventing injury to patients.” construction and plumbing modifications Pete Wirtz, MD Large flat transfer seat with removable grab bars ensures safe, comfortable toileting transfers Board Certified Orthopaedic Surgeon Pod design encloses mechanics for easy unit cleaning; open front enables easy cleaning of toilet and surrounding area Schedule a product in-service and evaluation for your facility today. Innovative drop-in commode bucket hygienically accommodates bedside toileting needs Call LiftSeat at (877) 665-4381 or Handheld control pendant gives caregivers the ability to operate the lifting process visit us online at www.liftseat.com MADE IN USA The Bedside to Bathroom Toileting Solution Whether used as a bedside commode or over-the-toilet, the LS600 Bariatric Toilet Lift’s versatile design delivers a safe, stable, easy-to-use toileting solution that greatly reduces the physical force required by caregivers to help patients on and off the toilet. The LS600 also moves easily from room to room to support a facility’s toileting needs. -

Museum & Gardens
Museum & Gardens Program A: Waste & Water at Point Ellice House Updated January 2021 Note: There is a powerpoint slideshow file that accompanies this package which you can use in conjunction with or instead of the provided worksheets. Program Outline General Description Program Title: Waste & Water at Point Ellice House Target Grades: 1 through 5 Location Addressed: Point Ellice House, Victoria, British Columbia Time Period Addressed: 1870s–1920s Links to Curriculum Content: ● Relationships between a community and its environment ● How people’s needs and wants are met in communities ● Local (Victoria) and colonial settler history Recommended Program Time: 50–80 minutes. For the youngest grades, we strongly recommend working on a single activity in a session, rather than completing all three at once. Historical Context Point Ellice House was built in 1862, and no flush toilet existed on the property until at least the 1880s. Residents would use commodes, privies (outhouses), or chamber pots to go to the bathroom. The first flush toilets came to North America only in the late 1800s. A municipal water supply did not come to Victoria until the 1870s. Commodes and chamber pots were used primarily at night and emptied into the pits of the privies in the morning. The O’Reillys were a wealthy family and employed servants, so this would have been the work of the chambermaid. The privy pits would eventually fill up. It was the job of private businessmen called scavengers to empty them. This job was done at night because of the foul smell. There was a well on the property that was used to get water until city water pipes were extended to the house in 1876. -
How to Clean and Sanitize a Bedside Commode
How to Clean and Sanitize a Bedside Commode Cleaning Keeping a bedside commode clean and odor free doesn't have to be a chore. Much like your toddler's old potty chair, bedside commodes are relatively easy to clean. All it takes is a pair of disposable gloves, Clorox wipes, and a can of Lysol aerosol spray. Step 1: Put on a pair of disposable gloves. Step 2: Place the lid on the waste container and carry with both hands to the bathroom. (For models with a carrying handle, it's a wise practice to support the bucket with one hand in case the handle detaches). Lift up the toilet seat and pour the contents into the toilet. Step 3: Rinse the bucket with some warm water and pour into the toilet. This will help to remove residual amount of waste. Step 4: Wipe down the inside of the bucket with Clorox wipes, disposing of the wipes in a separate container. For the frugally minded, a less expensive solution is to make your own cleaning agent by mixing up a pint of warm water with a tablespoons of bleach, which can then be decanted in a spray bottle. Spray the solution directly onto a paper towel which can then be used to wipe down the inside of the waste bucket and the underside of the lid. Take care not to spill any of the solution on your clothes or the bathroom rug! Step 5: Rinse the waste pail thoroughly with warm water and dry with a clean rag. Step 6: Spray the inside of the container with Lysol spray, and then place the bucket back under the commode. -

Performing Toilets: Putting Matter Into Place Danielle Dick Mcgeough Louisiana State University and Agricultural and Mechanical College
Louisiana State University LSU Digital Commons LSU Doctoral Dissertations Graduate School 2011 Performing toilets: putting matter into place Danielle Dick McGeough Louisiana State University and Agricultural and Mechanical College Follow this and additional works at: https://digitalcommons.lsu.edu/gradschool_dissertations Part of the Communication Commons Recommended Citation Dick McGeough, Danielle, "Performing toilets: putting matter into place" (2011). LSU Doctoral Dissertations. 157. https://digitalcommons.lsu.edu/gradschool_dissertations/157 This Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion in LSU Doctoral Dissertations by an authorized graduate school editor of LSU Digital Commons. For more information, please [email protected]. PERFORMING TOILETS: PUTTING MATTER INTO PLACE A Dissertation Submitted to the Graduate Faculty of the Louisiana State University and Agricultural and Mechanical College In partial fulfillment of the Requirements for the degree of Doctor of Philosophy in The Department of Communication Studies By Danielle Dick McGeough B.A., University of Northern Iowa, 2004 M.A., University of Northern Iowa, 2007 December 2011 Acknowledgements The process of writing is full of moments of self-doubt and possibility, isolation and connection, pleasure and frustration. Persevering through the process of writing is dependent on the bonds of real friendships and collaboration. There are many people whose unconditional love continues to nurture me in ways far beyond my expectations. I am forever grateful to those of you who have made this project possible. Thank you. Dr. Ruth Laurion Bowman, thank you for selflessly offering your time and energy to comment on these words and ideas, and critically engaging with me in generous and generative ways. -
Assistive Product Specification for Procurement
ASSISTIVE PRODUCT SPECIFICATION FOR PROCUREMENT Toilet and Shower Chairs Objective: The objective of this specification is to help organizations in procuring good quality toilet/shower chairs that are durable and which help individuals with self-care. World Health Organization DRAFT – DO NOT CIRCULATE FOR USE 1. Product description The purpose of this section is to provide specific key details relevant to the assistive product so that it is easily identifiable. Purpose of 1.1 Name of product as per WHO priority APL and/or commonly used names. 1.1 Name of product Toilet/shower chairs Purpose of 1.2 As per ISO 9999 classification and terminology document (refer https://www.iso.org/standard/60547.html). 1.2 ISO 9999 code 09 12 03 Commode chairs Chairs, with or without castors, with a collection receptacle used for toileting away from the bathroom Included are, e.g. sanichairs, toilet wheelchairs, commode chairs also used for showering. 09 12 12 Raised toilet seats mounted on frame Raised toilet seats (separate) standing on floor, where the seat can easily be removed from the toilet bowl Included are, e.g. over toilet frames. 09 33 07 Shower chairs with and without wheels Devices for supporting sitting during showering Included are, e.g. shower stools. Purpose of 1.3 Describes the product type in clear, simple, easily understood language and the intended use in addressing functional needs. 1.3 Description and Toilet/ Shower Chairs are designed to enable hygiene maintenance for those who find it intended use difficult or impossible to use a standard toilet or shower. -

Cleaning Your Apartment
Cleaning Your Apartment *Special Note: Safety First! 1. Always read cleaning chemical directions and warnings 2. Never mix chemicals, especially bleach and ammonia BATHROOM TUB & TILE fill your tub with hot water. Dump a significant amount of scouring powder into the water and use a scratch pad or brush to scrub the tub and walls. Follow these directions for the sink. Use glass cleaner to shine spigots BATHROOM COMMODE/TOILET use a toilet cleaning solution or scouring powder and a toilet brush to scrub inside and out, include toilet seat. Typically missed areas are by the bolts on the seat and the bolts that hold your toilet to the floor. If it’s not white, it’s not clean. BATHROOM MEDICINE CABINET top, shelves, & mirror should be wiped with glass cleaner. BATHROOM SINK Use a bathroom cleaning solution, scouring powder, or Soft Scrub to clean the sink area. BLINDS should feel smooth and be dust and residue free. Dusting will usually do the job except around the kitchen areas where blinds may have grease build up. Pull blinds down and turn the handle until the blinds are closed. Use a soft cloth to gently dust. Also, avoid using a strong cleaner like Formula 409. It may also cause paint to peel. Be careful not to bend the slats. CARPET usually is fine after vacuuming, but if it is discolored or darkened in heavy traffic areas or if you have major stains, you can try using Woolite or Resolve to clean stained areas. DISHWASHER wipe down inside and outside with soapy water. -
Unit 5: Safe Handling and Disposal of Faeces 27
Unit 5: Safe Handling and Disposal of Faeces 27. Do all faeces contaminate and spread illnesses? Yes, ALL faeces contaminate and spread illnesses, whether they are from adults, children, babies, or animals. 28.Where to Dispose of Faeces Safely disposing of faeces is a critical step to reducing the chance of spreading germs and greatly reducing the spread of diseases. It is important to put ALL faeces in a latrine. ALL faeces from people (babies, young children, the frail/elderly, the ill, the healthy) should be put in a latrine. If it is impossible to put the faeces in a latrine, then you should bury the faeces (like cats bury their faeces). Animal and people faeces that are in and around the house and near your source of water should be picked up with a shovel/hoe/broom (not by hand!) and put in the latrine or buried (the way cats bury their faeces). 72 FAECES DISPOSAL Counselling Card Put faeces of sick people, adults, children, babies, and animals (including birds) in a latrine. HYGIENE IMPROVEMENT PROJECT THE REPUBLIC OF UGANDA HIP Ministry of Health 29. Faeces and Urine Disposal Care for a BEDBOUND client The body must get rid of faeces and urine to remain healthy. The amount of help that a client needs to get rid of his/her faeces depends on how your client feels, how well they are able to move/walk, and whether the client can still control when he/she urinates or defecates. This section provides information for how to provide urine and faeces disposal help for clients who CANNOT GET OUT OF BED. -

Toilets of the World Free
FREE TOILETS OF THE WORLD PDF Morna E. Gregory,Sian James | 256 pages | 01 Sep 2009 | Merrell Publishers Ltd | 9781858944999 | English | London, United Kingdom Toilets From Around the World | One Point Partitions It's the one spot in every home that all members of the family use on a regular basis, from California to Dubai. Culture, custom, habit and convenience all dictate a society's notion of what defines a Toilets of the World toilet ," even though this humble household item is often taken for granted. Toilets of the World do what we do where we Toilets of the World it, with little ado, due to the toilet's unassuming quality in our lives. It's hardly any wonder, then, that so many folks are startled when encountering their first foreign toilet. Chances are, you might be surprised at Toilets of the World of the international Toilets of the World, both public and privately maintained, that the world has Toilets of the World offer a weary traveler. Across the globe, the toilet has evolved within sets of specific cultural traditions. Since each Toilets of the World has a different concept of hygiene, access to disposable paper and water availability, our body's most natural functions have been dealt with in a variety of ways. Despite complaints about airline bathrooms, plan an international excursion and you may find that the airplane toilet was the last vestige of Toilets of the World hometown bathroom expectations. But you'll also find that the world offers a myriad of ways for one to "get down to business. -

Water Stream in Bidet Toilet Commode As a Cause of Anterior Anal Fissure: a Case-Control Study Pankaj Garg,1,2,* and Pratiksha Singh2
Ann Colorectal Res. 2017 March; 5(1-2):e46479. doi: 10.5812/acr.46479. Published online 2017 March 25. Research Article Water Stream in Bidet Toilet Commode as a Cause of Anterior Anal Fissure: A Case-Control Study Pankaj Garg,1,2,* and Pratiksha Singh2 1Colorectal Surgery Division, Indus Super Specialty Hospital, Mohali, Punjab, India 2Garg Fistula Research Institute, Panchkula, Haryana, India *Corresponding author: Pankaj Garg, Garg Fistula Research Institute, 1042, Sector-15, Panchkula, Haryana, India. Tel: +91-9501011000, Fax: +91-1722594556, E-mail: [email protected] Received 2017 January 09; Revised 2017 February 06; Accepted 2017 March 08. Abstract Background: Water used as a single sharp stream in toilet commode for post defecation cleansing is a common practice in sev- eral countries across the globe including India. Repeated hitting of the anus by water stream could potentially cause injury to the anal canal epithelium and lead to development of fissure-in-ano. As the water stream is emanating from the backside of the toilet commode, the possible injury, if any, would be on the anterior anal canal. Objectives: The present study aimed at determining whether water stream usage in toilet commodes increased the incidence of anterior fissure-in-ano; this was determined by the incidence of anterior fissure-in-ano the study and control groups. Methods: All consecutive fissure-in-ano patients referring to a colorectal clinic from February 2012 to 2015 were included in the study. The patients were classified as a study group (who were using water stream for cleansing purposes in toilet commodes) and a control group (patients who were not using water stream).