ANNUAL REPORT of the DEPARTMENT of HEALTH 2007 Table of Contents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mural Initiative Brochure Page1
mural initiative 2018 lebanon unrwa UNRWA Ein el Assal school compound, Rashidieh Palestine refugee camp, Tyre Each year since 2013, the UNRWA Operations Support Office Between October 2017 and November 2018, Palestine refugee team (OSO) in Lebanon has taken the lead on initiatives to paint children painted the walls of 14 UNRWA installations including 9 colourful murals on the walls of UNRWA installations in schools, 2 camp services office, 2 health clinic and 1 water tank Palestine refugee camps across Lebanon. Through these and sanitation office across 6 Palestine refugee camps in murals, the initiative aims to promote creativity in portraying Lebanon; Ein el Hilweh camp, Rashidieh camp, Beddawi camp, positive messages, to increase community engagement in Burj el Barajneh camp, Mar Elias camp and Wavel camp. relation to the camp environment, and in addition preserving the neutrality of UNRWA installations in the camps and gatherings. This document enlists the 2018 mural initiatives completed in the four areas of operation in Lebanon (North Lebanon, Central The mural painting included positive messaging related to water, Lebanon, Tyre and Saida) to address neutrality issues in the sanitation and hygiene, sports, inclusion of all communities, following installations: four UNRWA Schools (Sammou, Bissan, friendship and peace. Artists from the community were selected Safad and Naqoura) in Ein el Hilweh Palestine refugee camp, by UNRWA OSO teams to design mural paintings, with the involve- Saida; UNRWA health clinic in Rashidieh Palestine refugee ment of Palestine refugees in Lebanon (PRL) and Palestinian camp, Tyre; UNRWA Ein el Assal school in Rashidieh Palestine refugees from Syria (PRS) children to decide on the themes and refugee camp, Tyre; UNRWA Majeddo and Mazar schools in designs. -

The United Nations and Palestinian Refugees the United Nations and Palestinian Refugees
UNRWA CONTACTS: Public Information Office Gaza HQ P.O. Box 140157 Amman, Jordan 11814 Tel.: +972 8 677 7527 Fax: +972 8 677 7697 E-mail: [email protected] Website: www.unrwa.org UNHCR CONTACTS: United Nations High Commissioner for Refugees 94, Rue de Montbrillant Case Postale 2500 CH-1211 Genève 2 Dépôt Switzerland Tel.: +41 22 739 8111 Fax: +41 22 739 7334 E-mail: [email protected] Website: www.unhcr.org Front cover: Palestinians fleeing to Jordan,June 1967 / UNRWA Back cover: Tents had just been replaced by cement block houses at Khan Younis refugee camp, Gaza Strip, 1955 / UNRWA Inside cover: Baqa’a refugee camp, Jordan, 1969 / UNRWA Opposite: A Palestine refugee with her grandson in Beach refugee camp, Gaza Strip / UNRWA All UNRWA photographs courtesy of UNRWA Photo Archive & Steve Sabella January 2007 2 The United Nations and Palestinian Refugees The United Nations and Palestinian Refugees n December 1949, the United Nations General IAssembly established the United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) to provide humanitarian relief to the more than 700,000 refugees and displaced persons who had been forced to flee their homes in Palestine as a result of the 1948 Arab-Israeli war. Also in December 1949, the United Nations General Assembly decided to set up the Office of the United Nations High Commissioner / 1950s UNRWA for Refugees (UNHCR), as Suffering and fortitude of young and old in of 1 January 1951, with the Jalazone refugee camp, West Bank principal aim of dealing with refugees in Europe of Palestine refugees, that is, refugees left homeless by World War from the territory that had been under II. -

Survey of Palestinian Refugees and Internally Displaced Persons 2010 - 2012 Volume VII
BADIL Resource Center for Palestinian Residency and Refugee Rights is an independent, community-based non- This edition of the Survey of Palestinian Survey of Palestinian Refugees and profit organization mandated to defend Refugees and Internally Displaced Persons BADIL Internally Displaced Persons 2010-2012 and promote the rights of Palestinian (Volume VII) focuses on Palestinian Vol VII 2010-2012 refugees and Internally Displaced Persons Survey of refugees and IDPs. Our vision, mission, 124 Pages, 30 c.m. (IDPs) in the period between 2010 and ISSN: 1728-1679 programs and relationships are defined 2012. Statistical data and estimates of the by our Palestinian identity and the size of this population have been updated Palestinian Refugees principles of international law, in in accordance with figures as of the end Editor: Nidal al-Azza particular international human rights of 2011. This edition includes for the first law. We seek to advance the individual time an opinion poll surveying Palestinian Editorial Team: Amjad Alqasis, Simon and collective rights of the Palestinian refugees regarding specific humanitarian and Randles, Manar Makhoul, Thayer Hastings, services they receive in the refugee Noura Erakat people on this basis. camps. Demographic Statistics: Mustafa Khawaja BADIL Resource Center was established The need to overview and contextualize in January 1998. BADIL is registered Palestinian refugees and (IDPs) - 64 Internally Displaced Persons Layout & Design: Atallah Salem with the Palestinan Authority and years since the Palestinian Nakba Printing: Al-Ayyam Printing, Press, (Catastrophe) and 45 years since Israel’s legally owned by the refugee community Publishing and Distribution Conmpany represented by a General Assembly belligerent occupation of the West Bank, including eastern Jerusalem, and the 2010 - 2012 composed of activists in Palestinian Gaza Strip - is derived from the necessity national institutions and refugee to set the foundations for a human rights- community organizations. -

Israeli Human Rights Violations and Hamas Support Ii Preface
IIssrraaeellii HHuummaann RRiigghhttss VViioollaattiioonnss aanndd HHaammaass SSuuppppoorrtt RReesseeaarrcchhiiinngg PPeerrcceeppttiiioonnss ooff PPaallleessttiiinniiiaann rreeffuuggeeeess iiinn JJoorrddaann Lidwien Wijchers IIssrraaeellii HHuummaann RRiigghhttss VViioollaattiioonnss aanndd HHaammaass SSuuppppoorrtt RReesseeaarrcchhiiinngg PPeerrcceeppttiiioonnss ooff PPaallleessttiiinniiiaann rreeffuuggeeeess iiinn JJoorrddaann Cover photo Lidwien Wijchers Banner in Irbid refugee camp, Jordan: “The Palestinian case and Jerusalem are always in the heart and consciousness of his Majesty the King” Lidwien Wijchers s0801240 Master Thesis Human Geography Center for International Conflict Analysis and Management Radboud University Nijmegen Supervisor: Dr. S. Vukovic Second Reader: Dr. J. Wagemakers July 2013 Israeli Human Rights Violations and Hamas Support ii Preface This thesis is submitted as part of the Human Geography Master specialization Conflicts, Identities, and Territories at the Center of International Conflict Analysis and Management associated with the Radboud University Nijmegen. It is the result of fieldwork conducted in Jordan from August 2012 until March 2013. Throughout the process of writing this thesis, many people have been of help to me. Not in the least the respondents of my questionnaire, and experts with whom I conducted interviews. I hereby express my appreciation to all of them. Furthermore, I would like to extend gratitude to Dr. Siniša Vukovic who supervised me through the writing stages of the thesis, and to my second reader Dr. Joas Wagemakers. Acknowledgment must also be given to Dr. Gearoid Millar, for his guidance in the initial stages of the project. Four other individuals deserve recognition. Lauren Salathiel and Mohamed el Atfy; thank you for your willingness to be sounding boards. Hashim Taani and Rakan Odeh, I am much indebted to you both for the amount of time and help you have selflessly given. -
University of Cincinnati
U UNIVERSITY OF CINCINNATI Date: 05-20-2009 I, Shadi Y. Saleh , hereby submit this original work as part of the requirements for the degree of: Master in Architecture It is entitled: Designing by Community Participation: Meeting the Challenges of the Palestinian Refugee Camps Shadi Saleh Student Signature: This work and its defense approved by: Committee Chair: Elizabeth Riorden Thomas Bible Approval of the electronic document: I have reviewed the Thesis/Dissertation in its final electronic format and certify that it is an accurate copy of the document reviewed and approved by the committee. Committee Chair signature: Elizabeth Riorden Designing by Community Participation: Meeting the Challenges of the Palestinian Refugee Camps A thesis submitted to the Division of Research and Advance Studies of the University of Cincinnati in partial fulfillment of the requirements of the degree of Master of Architecture In the school of Architecture and Interior design Of the College of Design, Architecture, Art and Planning 2009 By Shadi Y. Saleh Committee chair Elizabeth Riorden Thomas Bible ABSTRACT Palestinian refugee camps in the West Bank, Gaza Strip, Jordan, Lebanon and Syria are the result of the sudden population displacements of 1948 and 1967. After 60 years, unorganized urban growth compounds the situation. The absence of state support pushed the refugees to take matters into their own hands. Currently the camps have problems stemming from both the social situation and the degradation of the built environment. Keeping the refugee camps in order to “represent” a nation in exile does not mean to me that there should be no development. The thesis seeks to make a contribution in solving the social and environmental problems in a way that emphasizes the Right of Return. -

Every Child Learns
GOAL AREA 2 Every child learns Global Annual Results Report 2020 Cover image: © UNICEF/UNI366076/Bos Expression of thanks: © UNICEF/UN073783/Al-Issa Children learn on tablets in a new classroom in Tamantay, a village Somar, 8 years old from Syria, living with Down’s syndrome, in Kassala State, Sudan, on their first day of e-learning through the dreams of becoming a violinist and a professional swimmer. Can’t Wait to Learn programme. Expression of thanks The year 2020 was truly unprecedented for children around the world. The commitment of UNICEF’s resource partners allowed millions of children to continue to learn, grow and develop with the support of UNICEF programming. UNICEF funds come entirely from voluntary contributions. We take this opportunity to thank the millions of people, including our government partners, civil society and the private sector, who contributed to UNICEF’s funds this year. Without your support, our work would not have been possible. Your contributions have a wide impact and allow us to deliver on our mandate to advocate for the protection of children’s rights, to help meet their basic needs, and to expand their opportunities to reach their full potential. We also extend special and warm thanks to our partners who contributed to UNICEF’s thematic funding. Thematic funding was critical this year and will continue to be an essential tool that allows UNICEF the flexibility and predictability to deliver technical, operational and programming support to children across the world. By entrusting us with this funding, you have made many of the results in this report possible and have furthered our mandate to reach the most vulnerable children. -

Draft Chapter 1
UvA-DARE (Digital Academic Repository) Palestine online : cyber Intifada and the construction of a virtual community 2001-2005 Aouragh, M. Publication date 2008 Document Version Final published version Link to publication Citation for published version (APA): Aouragh, M. (2008). Palestine online : cyber Intifada and the construction of a virtual community 2001-2005. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) Download date:07 Oct 2021 Palestine Online Dit proefschrift werd mogelijk gemaakt met de financiële steun van: Amsterdam School voor Social Science Research (ASSR) Netherlands Organisation for Scientific Research (NWO) Netherlands Foundation for the Advancement of Tropical Research (WOTRO) Palestine Online Cyber Intifada and the Construction of a Virtual Community 2001-2005 ACADEMISCH PROEFSCHRIFT ter verkrijging van de graad van doctor aan de Universiteit van Amsterdam op gezag van de Rector Magnificus prof. -

Medical Support Manual for United Nations Peacekeeping Operations
UNITED NATIONS NATIONS UNIES MEDICAL SUPPORT MANUAL FOR UNITED NATIONS PEACEKEEPING OPERATIONS UNITED NATIONS DEPARTMENT OF PEACEKEEPING OPERATIONS MEDICAL SUPPORT MANUAL FOR UNITED NATIONS PEACEKEEPING OPERATIONS 2nd Edition Medical Support Manual for United Nations Peacekeeping Operations (2nd Edition) The manual is distributed by the Department of Peace-keeping Operations/ Office of Planning & Support/ Medical Support Unit, New York, 1999. The first edition was issued in 1995 and has since been revised. Copyright © United Nations 1999 This document enjoys copyright under Protocol 2 of the Universal Copyright Convention. Member States’ governmental authorities may, however, photocopy this document for exclusive use within their training institutes. The number of this copy, which is shown at the end of this page, should be noted for future distribution of updates and amendments. No portion of this document may be reproduced for resale or mass publication without the expressed written consent of the Medical Support Unit. No part of the document may be stored in a retrieval system without the prior authorization of the Medical Support Unit. Any communications with regards to the above are to be directed to: DPKO/ OPS/ MSU Secretariat Building, Room 2200-E 1 United Nations Plaza New York, NY 10017, USA Phone: (212) 963-4147 Fax: (212) 963-2614 PREFACE General There has always been a requirement for a standard reference document on the medical support aspects of United Nations peacekeeping operations. To meet this requirement, the Medical Support Manual for United Nations Field Operations was published and distributed in 1995. This aimed to outline operational and procedural guidelines for medical support in the field. -
A Year of Transition
A YEAR OF TRANSITION 2019 ANNUAL REPORT Transitions to Peace 28 PUBLISHING EDITOR: Achieving lasting peace 28 Séverine Ougier Highlights from 2019 30 2020 and beyond 30 AUTHORS & CONTRIBUTORS: Promoting Youth Leadership 32 Sofia Anton A threat to peace 32 Sébastien F. W. Brack Highlights from 2019 33 Alan Doss Contents 2020 and beyond 35 Genna Ingold Michaelene Kinnersley Fabian Lange Combating Hunger 36 Li Ling Low A threat to peace 36 Natalie McDonnell Highlights from 2019 36 Declan O'Brien Foreword by Elhadj As Sy 06 Protecting and enhancing Kofi Annan’s 2020 and beyond 37 Maud Roure legacy: Vision Annan 18 Elhadj As Sy Message from Alan Doss 08 Celebrating Kofi Annan's legacy The Kofi Annan Foundation Board 38 in 2019 18 2020 and beyond 19 AGENCY: About the Kofi Annan Foundation 10 Staff 43 GSDH Kreativagentur Our mission 10 Supporting democracy and elections www.gsdh.org Funding 46 Our values 11 with integrity 20 Funders 46 How the Kofi Annan Foundation works 11 A threat to peace 20 Private Donors 46 IMAGE CREDITS: The three pillars of a fairer, more Highlights from 2019 22 peaceful world 11 Partners 47 Cover and p.42: Eric Roset Protecting Electoral Integrity in the Digital Age 25 All other images used under licence from Our activities in 2019 12 Finances 48 Shutterstock.com or are the property of North and South America 12 Among the key findings 25 2019 Expenses 48 the Kofi Annan Foundation. Europe 14 Download the report 25 2019 Sources of Funds 49 Africa 15 2020 and beyond 26 PRINT DATE: Asia 17 The Kofi Annan Commission on Elections Funding our work with your and Democracy in the Digital Age 27 philanthropic gifts and grants 50 July 2020 06 FOREWORD | ELHADJ AS SY KOFI ANNAN FOUNDATION l 2019 ANNUAL REPORT 07 FOREWORD Elhadj As Sy Foundation after a dynamic and successful career at the Chair of the United Nations. -

Am'ari Refugee Camp
unrwa west bank Photo by Dominiek Benoot profile: am’ari camp ramallah and al-bireh governorate Overview UNRWA in Am’ari camp Am’ari camp, located east of Ramallah city General information UNRWA in Am’ari camp in al-Bireh municipality, is one of the • Established: 1949 Main UNRWA installations: smallest camps in the West Bank. Before the • Size: .096 sq km • Four schools first intifada, many refugees living in Am’ari • Population before 1967 (OCHA): 3,930 • One health centre camp were able to move to surrounding • Estimated population (PCBS): 6,100 villages and cities. However, the • Registered persons (UNRWA): 12,000 UNRWA employees working in Am’ari construction of the West Bank Barrier, • Estimated density: 72,916 per sq km camp: 111 expansion of Ramallah and rising property • Places of origin: Mainly Jaa, Lydd, Remleh, • Education: 71 • Health: 24 prices has meant that this has become and Jerusalem • Relief and Social Services: 3 prohibitively expensive for most residents. * Many refugees left the camp and settled in Ramallah, Bireh, Bitunia, and • Sanitation services: 10 Um al-Sharayet neighbourhoods but maintained their registrered The growing population remains a residence in Am’ari camp. • Administration: 3 challenge for service provision as well as on the existing infrastructure in the camp, while also contributing to overcrowding Relief, Social Services and Emergency Response and poor living conditions. UNRWA social workers conduct regular home visits in the camp to identify families requiring special assistance. Additionally, through the Social Safety Net Programme, Residents in Am’ari report that unemploy- UNRWA provides food parcels to approximately 1,330 impoverished refugees in the camp ment in the camp is rising, especially (approximately 11 per cent of registered persons in the camp). -

Urban Planning Analyses of Refugee Camps, Jabalia As Case Study-Gaza Strip, Palestine
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 Index Copernicus Value (2013): 6.14 | Impact Factor (2015): 6.391 Urban Planning Analyses of Refugee Camps, Jabalia as Case Study-Gaza Strip, Palestine Dr. Usama Ibrahim Badawy1, Dr Ra’ed A. Salha2, Dr. Muain Qasem Jawabrah3, Amjad Jarada4 Mohammed A. EL Hawajri5 1Former Professor of Architecture, Birzeit University Palestine, works currently at UNRWA 2Assistant Professor, Islamic University of Gaza in Geography and GIS Palestine 3Assistance Professor, Architecture Department, Birzeit University Palestine 4Researcher in Infrastructure Planning and Development works currently at UNRWA, G, 5Researcher Geography subjects, works currently as teacher by the Ministry of Education Abstract: The Gaza Strip is a tight area with more than 1.8 million inhabitants. Since the beginning of the last century, and as other Palestinian areas, Gaza Strip was subject to direct occupation. The occupation tightened laws and regulations and increased obstacles, meanwhile it established settlements in a method that besieges existing Palestinian urban areas and leads them to develop in a way that serves the occupation, particularly the security side. This research begins with background information on Palestinian refugees in Gaza, sees that camp Improvement Strategies should called for adoption of the future urban planning, increasing the accommodation capacity of the built-up area, activating the environmental resources protection laws and played down the issue of the land properties when preparing the comprehensive plans. In this study reviews options for addressing the problems faced by Palestinian refugees in Gaza, Recommendations: After discussing the topic through a analyses of the Current Conditions , Land availability, Population distribution, Land requirements, Overcrowding, Public Spaces problems inside the camps , Sustainability in Gaza Strip, socio-economic situation , Unemployment problem and Population density in Jabalia Camp. -
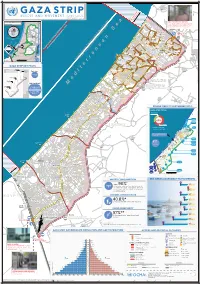
Gaza CRISIS)P H C S Ti P P I U
United Nations Office for the Coordination of Humanitarian Affairs occupied Palestinian territory Zikim e Karmiya s n e o il Z P m A g l in a AGCCESSA ANDZ AMOV EMENTSTRI (GAZA CRISIS)P h c s ti P P i u F a ¥ SEPTEMBER 2014 o nA P N .5 F 1 Yad Mordekhai EREZ CROSSING (BEIT HANOUN) occupied Palestinian territory: ID a As-Siafa OPEN, six days (daytime) a B?week4 for B?3the4 movement d Governorates e e of international workers and limited number of y h s a b R authorized Palestinians including aid workers, medical, P r 2 e A humanitarian cases, businessmen and aid workers. Jenin d 1 e 0 Netiv ha-Asara P c 2 P Tubas r Tulkarm r fo e S P Al Attarta Temporary Wastewater P n b Treatment Lagoons Qalqiliya Nablus Erez Crossing E Ghaboon m Hai Al Amal r Fado's 4 e B? (Beit Hanoun) Salfit t e P P v i Al Qaraya al Badawiya i v P! W e s t R n m (Umm An-Naser) n i o » B a n k a North Gaza º Al Jam'ia ¹¹ M E D I TER RAN EAN Hatabiyya Ramallah da Jericho d L N n r n r KJ S E A ee o Beit Lahia D P o o J g Wastewater Ed t Al Salateen Beit Lahiya h 5 Al Kur'a J a 9 P l D n Treatment Plant D D D D 9 ) D s As Sultan D 1 2 El Khamsa D " Sa D e J D D l i D 0 D s i D D 0 D D d D D m 2 9 Abedl Hamaid D D r D D l D D o s D D a t D D c Jerusalem D D c n P a D D c h D D i t D D s e P! D D A u P 0 D D D e D D D a l m d D D o i t D D l i " D D n .