Population Situation Analysis: Sri Lanka
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Newsletter Supporting Communities in Need
NEWSLETTER ICRC JULY-SEPTEMBER 2014 SUPPORTING COMMUNITIES IN NEED Economic security and water and sanitation for the vulnerable Dear Reader, they could reduce the immense economic This year, the ICRC started a Community Conflicts destroy livelihoods and hardships and poverty under which they Based Livelihood Support Programme infrastructure which provide water and and their families are living at present” (para (CBLSP) to support vulnerable communities sanitation to communities. Throughout 5.112). in the Mullaitivu and Kilinochchi districts the world, the ICRC strives to enable access to establish or consolidate an income to clean water and sanitation and ensure The ICRC’s response during the recovery generating activity. economic security for people affected by phase to those made vulnerable by the conflict so they can either restore or start a conflict was the piloting of a Micro Economic The ICRC’s economic security programmes livelihood. Initiatives (MEI) programme for women- are closely linked to its water and sanitation headed households, people with disabilities initiatives. In Sri Lanka today, the ICRC supports and extremely vulnerable households in vulnerable households and communities In Sri Lanka, the ICRC restores wells the Vavuniya district in 2011. The MEI is in the former conflict areas to become contaminated as a result of monsoonal a programme in which each beneficiary economically independent through flooding, and renovates and builds pipe identifies and designs the livelihood sustainable income generation activities and networks, overhead water tanks, and for which he or she needs assistance to provides them clean water and sanitation by toilets in rural communities for returnee implement, thereby employing a bottom- cleaning wells and repairing or constructing populations to have access to clean water up needs-based approach. -

Sri Lanka – Tamils – Eastern Province – Batticaloa – Colombo
Refugee Review Tribunal AUSTRALIA RRT RESEARCH RESPONSE Research Response Number: LKA34481 Country: Sri Lanka Date: 11 March 2009 Keywords: Sri Lanka – Tamils – Eastern Province – Batticaloa – Colombo – International Business Systems Institute – Education system – Sri Lankan Army-Liberation Tigers of Tamil Eelam conflict – Risk of arrest This response was prepared by the Research & Information Services Section of the Refugee Review Tribunal (RRT) after researching publicly accessible information currently available to the RRT within time constraints. This response is not, and does not purport to be, conclusive as to the merit of any particular claim to refugee status or asylum. This research response may not, under any circumstance, be cited in a decision or any other document. Anyone wishing to use this information may only cite the primary source material contained herein. Questions 1. Please provide information on the International Business Systems Institute in Kaluvanchikkudy. 2. Is it likely that someone would attain a high school or higher education qualification in Sri Lanka without learning a language other than Tamil? 3. Please provide an overview/timeline of relevant events in the Eastern Province of Sri Lanka from 1986 to 2004, with particular reference to the Sri Lankan Army (SLA)-Liberation Tigers of Tamil Eelam (LTTE) conflict. 4. What is the current situation and risk of arrest for male Tamils in Batticaloa and Colombo? RESPONSE 1. Please provide information on the International Business Systems Institute in Kaluvanchikkudy. Note: Kaluvanchikkudy is also transliterated as Kaluwanchikudy is some sources. No references could be located to the International Business Systems Institute in Kaluvanchikkudy. The Education Guide Sri Lanka website maintains a list of the “Training Institutes Registered under the Ministry of Skills Development, Vocational and Tertiary Education”, and among these is ‘International Business System Overseas (Pvt) Ltd’ (IBS). -

Medicalization of Pregnancy and Childbirth in Sri Lanka Chandani
Medicalization of Pregnancy and Childbirth in Sri Lanka Chandani Liyanage1 Whether the pregnancy and childbirth is a normal event or only a biomedical condition, is yet to be resolved with clear-cut definitions. In the context of Sri Lanka, it had been totally managed by the lay people till the ultra modern science and technology assumed control. Till the gradual shifting of the deal to the hands of experts took place, the event of pregnancy and childbirth was engulfed by a whole network of relations, values, local beliefs and knowledge system. The magnanimity of the expert is such that by now it has become a medicalized issue even in the remote areas. The transfiguration of pregnancy and childbirth is not simply a metaphor for shifting from one institutional site (family and traditional birth attendant) to another (hospital), but also symbolized as a transition of knowledge system regarding the body in general and women’s reproductive body in particular. The objectives of this paper are to explore as to how the event of pregnancy and childbirth has become a medicalized issue even within the village space; how has the transition took place from a totally lay knowledge management to a medicalized issue and what will be the position of already existing and the heretofore knowledge of this subject as against the ensuing medicalize process. Empirical evidence of this study clearly reflects the lack of attention to the social and cultural factors which has not only led to the virtual extinction of the traditional knowledge system, but also to the modern system being deprived of an opportunity for a grand success by incorporating certain constructive traditional aspects. -
Batticaloa District
LAND USE PLAN BATTICALOA DISTRICT 2016 Land Use Policy Planning Department No.31 Pathiba Road, Colombo 05. Tel.0112 500338,Fax: 0112368718 1 E-mail: [email protected] Secretary’s Message Lessons Learnt and Reconciliation Commission (LLRC) made several recommendations for the Northern and Eastern Provinces of Sri Lanka so as to address the issues faced by the people in those areas due to the civil war. The responsibility of implementing some of these recommendations was assigned to the different institutions coming under the purview of the Ministry of Lands i.e. Land Commissioner General Department, Land Settlement Department, Survey General Department and Land Use Policy Planning Department. One of The recommendations made by the LLRC was to prepare Land Use Plans for the Districts in the Northern and Eastern Provinces. This responsibility assigned to the Land Use Policy Planning Department. The task was completed by May 2016. I would like to thank all the National Level Experts, District Secretary and Divisional Secretaries in Batticaloa District and Assistant Director (District Land Use.). Batticaloa and the district staff who assisted in preparing this plan. I also would like to thank Director General of the Land Use Policy Planning Department and the staff at the Head Office their continuous guiding given to complete this important task. I have great pleasure in presenting the Land Use Plan for the Batticaloa district. Dr. I.H.K. Mahanama Secretary, Ministry of Lands 2 Director General’s Message I have great pleasure in presenting the Land Use Plan for the Batticaloa District prepared by the officers of the Land Use Policy Planning Department. -
Preparedness for Implementation of Sustainable Development Goals
Preparedness for Implementation of Sustainable Development Goals Report No.PER/2017/2018/SDG/05 National Audit Office Performance Audit Division 1 | P a g e National preparedness for SDG implementation The summary of main observations on National Preparedness for the Implementation of Sustainable Development Goals (SDGs) is as follows. 1. The Rapid Integrated Assesment (RIA) is a first step in the process of aligning the country,s national development plan or public Investment programme with SDGs and RIA reveals an uneven alignment between the policy initiatives in the 2017 -2020 Public Investment Programme and the SDG target areas for the economy as (84%) people (80%) planet (58%) peace (42%) and partnership (38%). 2. After deducting debt repayments, the Government has allocated Rs. 440,787 million or 18 percent out of the total national budget of Rs. 2,997,845 million on major projects which identified major targets of relevant SDGs in the year 2018. 3. Sri Lanka had not developed a proper communication strategy on monitoring, follow up, review and reporting on progress towards the implementation of the 2030 agenda. 2 | P a g e Audit at a glance The information gathered from the selected participatory Government institutions have been quantified as follows. Accordingly, Sri Lanka has to pay more attention on almost all of the areas mentioned in the graph for successful implementation of Sustainable Development Goals. 40.0% Alignment of budgets, policies 34.5% and programmes 35.0% Policy integration and coordination 30.0% 28.5% 28.3% 27.0% 26.6% Creating ownership and engaging stakeholders 25.0% 24.0% Identification of resources and 20.5% 21.0% capacities 20.0% Mobilizing partnerships 15.0% Managing risks 10.0% Responsibilities, mechanism and process of monitoring, follow-up 5.0% etc (institutional level) Performance indicators and data 0.0% 3 | P a g e Contents Executive Summary ................................................................................................................ -

Rapid Environmental Assessment (REA) Checklist
Environmental Safeguards Due Diligence Report Project Number 42459-014 August 2019 Sri Lanka: Local Government Enhancement Sector Project Additional Financing (LGESP-AF) ̶ Construction of Multipurpose Building at Madurankuliya for Puttalam Pradeshiya Sabha (NWP-AF-PUT-04) Prepared by LGESP (Pura Neguma) Project Management Unit for the Ministry of Internal & Home Affairs and Provincial Councils & Local Government (Formerly named as “Ministry of Provincial Councils, and Local Government and Sports”), Colombo, Sri Lanka and the Asian Development Bank. This environmental safeguards due diligence report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB’s Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgements as to the legal or other status of any territory or area. Ministry of Provincial Councils and Local Government Local Government Enhancement Sector Project (Additional Financing) (ADB assisted – Loan 3431 SRI) DUE DILIGENCE REPORT - ENVIRONMENT PACKAGE NUMBER - NWP AF PUT 04 CONSTRUCTION OF MADURANKULIYA MULTI PURPOSE BUILDING FOR PUTTALAM PRADESHYA SABHA NORTH WESTERN PROVINCE, SRI LANKA March 2019 Prepared for Local Government Enhancement Sector Project (Additional Finance) Subproject Coordination Unit - North Western Province 1. INTRODUCTION A. Background 1. The Local Government Enhancement Sector Project (LGESP) is a key infrastructure initiative of the Government of Sri Lanka which aims to improve local infrastructure, and services delivered effectively by local authorities in less developed areas in Sri Lanka. -
IDP Numbers and Access 30042009 GA Figures
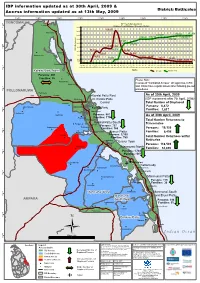
IDP information updated as at 30th April, 2009 & District: Batticaloa Access information updated as at 13th May, 2009 81°15'0"E 81°20'0"E 81°25'0"E 81°30'0"E 81°35'0"E 81°40'0"E 81°45'0"E 81°50'0"E 81°55'0"E TRINCOMALEE (! IDP Trend - Batticaloa District Verugal Returnees Trend - Batticaloa / Trincomalee Districts 8°15'0"N 180,000 159,355 (! 160,000 Kathiravely 136,084 137,659 140,000 127,837 119,527 120,742 136,555 120,000 132,728 97,405 100,000 108,784 72,986 80,000 81,312 8°10'0"N IDPs/Returnees 60,272 68,971 60,000 51,901 (! Vaharai (! 52,685 38,230 Kaddumurivu 40,000 38,121 26,484 24,987 17,600 18,171 12,551 20,000 8,020 1,140 8,543 6,872 (! 0 Panichankerny Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec Jan Feb Mar Apr 2006 2006 2006 2006 2006 2006 2006 2006 2006 2007 2007 2007 2007 2007 2007 2007 2007 2007 2007 2007 2007 2008 2008 2008 2008 2008 2008 2008 2008 2008 2008 2008 2008 2009 2009 2009 2009 8°5'0"N Months IDP Trend Returnees' Trend Koralai Pattu North A 1 Persons: 201 5 Families: 55 (! Please Note: Kirimichchai In areas of "Controlled Access" UN agencies, ICRC Mankerny (! and INGO have regular access after following pre-set procedures. -

Sri Lanka –Eastern Province – Trincomalee – Security Situation – Human Rights – Military and Paramilitary Groups – TMVP – Tamils with LTTE Links – Kiliveddy - Muthur
Refugee Review Tribunal AUSTRALIA RRT RESEARCH RESPONSE Research Response Number: LKA35265 Country: Sri Lanka Date: 5 August 2009 Keywords: – Sri Lanka –Eastern Province – Trincomalee – Security situation – Human Rights – Military and paramilitary groups – TMVP – Tamils with LTTE Links – Kiliveddy - Muthur This response was prepared by the Research & Information Services Section of the Refugee Review Tribunal (RRT) after researching publicly accessible information currently available to the RRT within time constraints. This response is not, and does not purport to be, conclusive as to the merit of any particular claim to refugee status or asylum. This research response may not, under any circumstance, be cited in a decision or any other document. Anyone wishing to use this information may only cite the primary source material contained herein. Questions 1. Please provide an update of the security situation in the East of Sri Lanka, particularly Trincomalee. 2. Is there a large military presence in Trincomalee? Are there reports of human rights abuses by the military in the east? 3. Do paramilitary groups/pro-government militias (such as those previously headed by Karuna and/or Pilliyan) still operate in Trincomalee? Are they still a threat to Tamils who are suspected of having LTTE links? 4. Is there any evidence of a town called Kiliveddy Muthur Trincomalee? Prior to the Sri Lankan government claiming victory over the LTTE, was Kiliveddy controlled by the LTTE or the government? RESPONSE 1. Please provide an update of the security situation in the East of Sri Lanka, particularly Trincomalee. The response to this question has been divided into two sections, the first dealing specifically with security in Trincomalee and the second relating more generally to the security situation in the Eastern Province of Sri Lanka. -

Ministry of Social Empowerment & Welfare
MMiinniissttrryy ooff SSoocciiaall EEmmppoowweerrmmeenntt && WWeellffaarree PPeerrffoorrmmaannccee RReeppoorrtt 22001155 1st Floor Sethsiripaya, Stage ii Battaramulla Telephone : 011-2887349-51 Fax : 011 – 2 187007 E - Mail : [email protected] b Ministry of Social Empowerment & Welfare Contents Page No Introduction i-iii Structure of the Ministry iv 01 Counseling Division 2- 6 01.1 Role of the Counseling Division 3 01.2 Activities in 2015 3-6 01.3 Financial & Phisical Progress 6 02 National Council & Secretariat for Persons with Disabilities 7 - 1 3 02.1 Introduction 8 02.2 Objectives 8 02.3 Financial & Phisical Progress 9-12 02.4 Special Activities 13 03 Single Parent Development Project 14-17 03.1 Introduction 15-16 03.2 Financial & Phisical Progress 17 04 Sisunena Pubuduwa Programme 18-19 04.1 Introduction 19 04.2 Financial & Phisical Progress 19 05 Social Care Centre Project 20 -24 05.1 Introduction 21 05.2 Financial & Phisical Progress 21-24 06 Rural Development Division 25 -35 06.1 Introduction 26 06.2 Financial & Phisical Progress 26-35 07 Department of Social Services 36-44 07.1 Introduction 37-38 07.2 Financial & Phisical Progress 38-42 07.3 Foreign Funded Projects 43-44 07.4 Special Programmes 44 c Ministry of Social Empowerment & Welfare 08 Department of Divineguma Development 45-57 08.1 Introduction 46 08.2 Projects under the 100 Day progamme 46-49 08.3 Financial & Phisical Progress 49-53 08.4 Other Major Programmes 54 08.5 Rural Development, Training & Research Institute 55-57 09 National Council & Secretariat for Elders 58-63 -
42459-014: Local Government Enhancement Sector Project
Environmental Monitoring Report Project Number 42459-014 Loan 3431 Semestral Report July to December 2020 April 2021 Sri Lanka: Local Government Enhancement Sector Project Additional Financing (LGESP-AF) Prepared by LGESP (Pura Neguma) Project Management Unit for the State Ministry of Provincial Councils and Local Government Affairs, Colombo, Sri Lanka and the Asian Development Bank. This environmental monitoring report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB’s Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgements as to the legal or other status of any territory or area. Government of Sri Lanka State Ministry of Provincial Councils & Local Government Affairs Semi Annual Environmental Safeguard Monitoring Report (HY2 - 2020 : 01 July 2020 to 31 December 2020) January 2021 Local Government Enhancement Sector Project - Additional Financing ADB Loan Number 3431 - SRI Project Management Unit Local Government Enhancement Sector Project 191 A, J R Jayewardene Centre, Dharmapala Mawatha, Colombo 07, Sri Lanka 2 ABBREVIATIONS ADB - Asian Development Bank AF - Additional Financing CEA - Central Environmental Authority CKD - Chronic Kidney Disease Management DSC - Design and Supervision Consultants EIA - Environmental Impact Assessment -

(Sri Lanka) - Mid-Term Joint Evaluation
Integrated programme for empowering conflict-affected countries (Sri Lanka) - Mid-Term Joint Evaluation Quick Facts saw the end of armed conflict almost two years before Vavuniya district in the Northern Countries: Sri Lanka Province, and the recovery phase is more Mid-Term Evaluation: August 2012 advanced into the development phase in Mode of Evaluation: Independent Batticaloa, although there are pockets of need ILO Administrative responsibility: CO- in areas where social indicators and civil society Colombo capacities are relatively weak and protection Technical Area: EMP/SKILLS needs high. Evaluation Management: Joint evaluation 2. ECAC which prioritizes a human security Evaluation Team : Dr. Darini Rajaisngham approach to recovery and development had Senanayake generated new networks and synergies among Project End: September 2013 beneficiaries, partners, local government Project Code: SRL/10/03/HSF institutions and service providers, NGOs and Donor: UNDP, UNICEF and ILO CSOs and opened new spaces for information (US$ 967,815) and knowledge sharing on protection and rights Keywords: economic reconstruction, skills based development. This in turn has aided development beneficiary, family and social empowerment and trust building. It has also helped create a sense of security, particularly for women and Executive summary of the joint children, which is visible where inter-agency evaluation report coordination and partnership with GoSL is strong as expressed by state officials and 1. The Integrated Program for empowering partners. Conflict Affected Communities in North East Sri Lanka (ECAC) had a solid reputation and was 3. There is good coverage of vulnerable well regarded among all stakeholders communities from the different ethno-religious interviewed in the course of the Mid Term communities in both districts, which serves to Review that covered the Vavuniya and promote social integration and harmony in a Batticaloa Districts. -

P Art1. Framing Fieldwork in the Batticaloa Region
part 1. framing fieldwork in the batticaloa region Downloaded from http://read.dukeupress.edu/books/book/chapter-pdf/633593/9780822389187-001.pdf by guest on 30 September 2021 introduction ri Lanka has been a remarkably fertile site for Sresearch in social and cultural anthropology, starting with C. G. and Brenda Z. Seligmann’s colo- nial monograph on the Veddas (1911) and continuing to this day with important ethnographic studies by Edmund R. Leach (1961), Nur Yalman (1967), Stanley J. Tambiah (1958), Gananath Obeyesekere (1967, 1981, 1984), James Brow (1978), Michael Roberts (1982), Bruce Kapferer (1983), Jonathan Spencer (1990a), R. L. Stirrat (1992), E. Valentine Daniel (1996), Rohan Bastin (2002), and many others. Despite “postcolo- nial and postempiricist” objections to anthropology in Sri Lanka (Ismail 2005), my intention was always to produce a book in the same scholarly tradition, a study that would extend understanding of the island’s remarkable sociological complexity through long- term, community-based fieldwork, as well as through critical engagement with anthropological writing on South Asia more generally. Now, however, given the brutal ethnic conflict which has consumed Sri Lan- kan society since the 1980s, this study also helps to illuminate what has become the most critical and divided conflict zone of the Eelam War—the island’s Downloaded from http://read.dukeupress.edu/books/book/chapter-pdf/633593/9780822389187-001.pdf by guest on 30 September 2021 Map 1. Sri Lanka and South India eastern coastal region—and the two Tamil-speaking minority communities who have lived there side by side for centuries—the Tamils and the Muslims (or Sri Lankan Moors).