MASTER CLINICIAN R.G. “Wick” Alexander, DDS, MSD
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Stability of Anterior Open Bite Treatment with Molar Intrusion Using Skeletal
González Espinosa et al. Progress in Orthodontics (2020) 21:35 https://doi.org/10.1186/s40510-020-00328-2 REVIEW Open Access Stability of anterior open bite treatment with molar intrusion using skeletal anchorage: a systematic review and meta- analysis Daybelis González Espinosa1,2, Paulo Eliezer de Oliveira Moreira1, Amanda Silva da Sousa1, Carlos Flores-Mir3 and David Normando1* Abstract Objectives: The aim of this systematic review and meta-analysis is to assess the degree of stability of anterior open bite (AOB) treatment performed through the molar intrusion supported with skeletal anchorage at least 1 year posttreatment. Methods: This study was registered in PROSPERO (CRD42016037513). A literature search was conducted to identify randomized (RCT) or non-randomized clinical trials based including those considering before and after design. Data sources were electronic databases including PubMed, Cochrane Library, Science Direct, Google Scholar, Scopus, Lilacs, OpenGrey, Web of Science, and ClinicalTrials.gov. The quality of evidence was assessed through the JBI tool and certainty of evidence was evaluated through the GRADE tool. Random effects meta-analysis was conducted when appropriate. Results: Six hundred twenty-four articles met the initial inclusion criteria. From these, only 6 remained. The mean posttreatment follow-up time was 2.5 years (SD = 1.04). The overbite showed a standardized mean relapse of − 1.23 mm (95% CI − 1.64, − 0.81, p < 0.0001). Maxillary and mandibular incisors presented a non-significant mean relapse, U1-PP − 0.04 mm (95% CI − 0.55, 0.48) and L1-MP − 0.10 mm (95% CI − 0.57, 0.37). Molar intrusion showed a relapse rate around 12% for the maxillary molars and a 27.2% for mandibular molars. -
Important Message
WE INTERRUPT YOUR REGULARLY SCHEDULED PROGRAM FOR AN IMPORTANT MESSAGE Q1 2018 inside this Disrupted: edition... New Rules for a New Type of Customer By Angela Weber, CMO OrthoSynetics Page 34 BUSINESS PRACTICE & DEVELOPMENT TRAVEL & LEISURE CLINICAL CORNER 18 15 37 From the Rear View Mirror Pro Travel Tips High Frequency Vibration Can BY DR. COURTNEY DUNN BY PROORTHO STAFF Reduce or Eliminate Pain During Aligner Treatment 30 20 BY DR. JONATHAN L. NICOZISIS Traveling to the Greek Islands New Gaidge CEO BY DR. DANIELA LOEBL INTERVIEW WITH RYAN MOYNIHAN 32 OFFICE LOGISTICS 34 Traveling to Peru Disrupted: New Rules for a New BY DR. DAVID WALKER 56 Type of Customer Beyond Reminders: BY ANGELA WEBER, CMO ORTHOSYNETICS 40 Tapping the Potential of Texting Traveling to Spain BY DR. KEITH DRESSLER 44 BY DR. DAVID MAJERONI What Would You Do If an Aligner 46 Store Opened Down the Street? ORTHOPUNDIT.COM BY DR. JENNIFER EISENHUTH Traveling to Europe BY DR. BEN BURRIS & BRIDGET BURRIS 09 MARKETING/ H.R. INSIGHT Don't Piss Momma Off! SOCIAL MEDIA BY DR. BEN BURRIS 05 28 24 Go High or Go Low - Just Don't Get Utilize Group Interviews To Made to Measure: Stuck in the Middle Maximize Hiring Success The Dubious Relationship Between BY DR. LEON KLEMPNER AND AMY EPSTEIN, BY BRIDGET BURRIS Eugenics and Orthodontics MBA ANSWERS FROM THE BY DR. MARC ACKERMAN 52 EDGE 59 5 Keys to Capturing the Fastest The Economy Is Booming – Why Growing Referral Source 10 Isn’t Your Practice? BY NICK DUNCAN Interviews with Dr. Jeff Kozlowski BY DR. -

Distalization of the Mandibular Dentition with Mini-Implants to Correct a Class III Malocclusion with a Midline Deviation
CASE REPORT Distalization of the mandibular dentition with mini-implants to correct a Class III malocclusion with a midline deviation Kyu-Rhim Chung,a Seong-Hun Kim,b HyeRan Choo,c Yoon-Ah Kook,d and Jason B. Copee Uijongbu and Seoul, Korea, Philadelphia, Pa, and Dallas, Tex This article describes the orthodontic treatment for a young woman, aged 23 years 5 months, with a Class III malocclusion and a deviated midline. Two orthodontic mini-implants (C-implants, CIMPLANT Company, Seoul, Korea) were placed in the interdental spaces between the mandibular second premolars and first mo- lars. The treatment plan consisted of distalizing the mandibular dentition asymmetrically and creating space for en-masse retraction of the mandibular anterior teeth. C-implants were placed to provide anchorage for Class I intra-arch elastics. The head design of the C-implant minimizes gingival irritation during orthodontic treatment. Sliding jigs were applied buccally for distalization of the mandibular posterior teeth. The active treatment period was 18 months. Normal overbite and overjet were obtained, and facial balance was improved. (Am J Orthod Dentofacial Orthop 2010;137:135-46) very orthodontic tooth movement is accompa- patients. Therefore, several authors have attempted to nied by a reaction. This can make it difficult to treat this type of malocclusion by distal tooth movement Ecorrect a malocclusion by using intraoral appli- alone. For example, animal studies and clinical investi- ances alone, especially when complete distal movement gations have used conventional implants as absolute of the mandibular dentition is planned in nonsurgical anchorage2-4 and miniplates for intrusion or distalization Class III malocclusion treatment. -

Upper Anterior Intrusion with Mini-Implants to Correct Anterior Deep Bite in a Periodontally Compromised Class II Malocclusion
www.medigraphic.org.mx Revista Mexicana de Ortodoncia Vol. 2, No. 2 April-June 2014 pp 105-111 CASE REPORT Upper anterior intrusion with mini-implants to correct anterior deep bite in a periodontally compromised class II malocclusion. Case report Intrusión del segmento anterior superior con miniimplantes para eliminar la mordida profunda anterior en maloclusión clase II con compromiso periodontal. Reporte de un caso Carlos Eder Zamudio López,* Silvia Tavira Fernández§ ABSTRACT RESUMEN The use of mini-implants has revolutioned biomechanics in or- El uso de miniimplantes ha revolucionado la biomecánica de thodontics with better results as far as anchorage is concerned. We la ortodoncia con mejores resultados en cuanto al anclaje se have no limits when using these attachments depending only on refi ere. No hay límites al momento de utilizar estos aditamentos, our imagination. Anterior deep bites in severe class II malocclusion y depende únicamente de nuestra imaginación. Las mordidas patients are a common problem that causes orthodontists to focus profundas en la región anterior son un problema frecuente en therapy in biomechanics to eliminate the problem by extrusion of los pacientes con clase II severa, lo que nos obliga a enfocar posterior teeth or intrusion of the anterior. In this case, we decided nuestra terapéutica en una mecánica a corregir el problema to correct the anterior deep bite by intruding the incisors using as mediante la extrusión de los dientes posteriores, o bien, mediante anchorage two mini-implants. The case was compromised by perio- la intrusión de los dientes anteriores. En este caso, decidimos dontal disease with moderated loss of alveolar bone so we had to corregir la mordida profunda anterior mediante la intrusión de los choose biomechanics with a stable anchorage to achieve our goals. -
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations
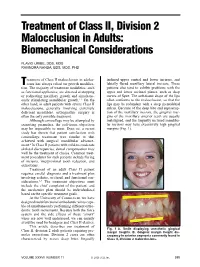
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD reatment of Class II malocclusion in adoles- inclined upper central and lower incisors, and Tcents has always relied on growth modifica- labially flared maxillary lateral incisors. These tion. The majority of treatment modalities, such patients also tend to exhibit problems with the as functional appliances, are directed at stopping upper and lower occlusal planes, such as deep or redirecting maxillary growth and simultane- curves of Spee. The soft-tissue drape of the lips ously stimulating mandibular growth.1-3 On the often conforms to the malocclusion, so that the other hand, in adult patients with severe Class II lips may be redundant with a deep mentolabial malocclusions, generally involving extremely sulcus. Because of the deep bite and supraerup- deficient mandibles, orthognathic surgery is tion of the maxillary incisors, the gingival mar- often the only possible treatment. gins of the maxillary anterior teeth are usually Although camouflage may be attempted by malaligned, and the lingually inclined mandibu- extracting premolars, the soft-tissue objectives lar incisors may have excessively high gingival may be impossible to meet. Even so, a recent margins (Fig. 1). study has shown that patient satisfaction with camouflage treatment was similar to that achieved with surgical mandibular advance- ment.4 In Class II patients with mild-to-moderate skeletal discrepancies, dental compensation may well be the treatment of choice. Common treat- ment procedures for such patients include flaring of incisors, interproximal tooth reduction, and extractions. Treatment of an adult Class II patient requires careful diagnosis and a treatment plan involving esthetic, occlusal, and functional con- siderations.5-7 The treatment objectives must include the chief complaint of the patient, and A the mechanics plan should be individualized based on the specific treatment goals. -

Invisalign Treatment Planning Guide 1 Align Technology, Inc
Table of Contents INTRODUCTION . 2 Getting Quality Clinical Outcomes with Invisalign. 2 Invisalign Applicability . 3 DIAGNOSIS AND TREATMENT OPTIONS 1. Crowding . 4 2. Spacing. 10 3. Narrow Arches . 16 4. Crossbite. 20 5. Deep Bite . 24 6. Open Bite . 28 7. Class II . 32 Invisalign 8. Class III . 38 CLINICAL NOTES Treatment IPR . 5 Tooth Size Discrepancy . 11 Planning Staging . 12 Auxiliary Treatment. 12 Guide Expansion . 17 Attachments. 25 Anchorage . 42 APPENDIX Prescription Form Tips. 44 Glossary . 46 Index. 48 Credits . 54 Invisalign Treatment Planning Guide 1 Align Technology, Inc. Introduction HOW TO USE THIS GUIDE Getting Quality Clinical The guide is organized by patient diagnosis. ABOUT THIS GUIDE Match your patient’s diagnosis to the appropriate Outcomes with Invisalign The goal of this guide is to provide you with a diagnosis decision tree to see some possible treat- decision making tool you can use while selecting ment options. Read the accompanying treatment Successful clinical outcomes with Invisalign and treatment planning your Invisalign cases. notes and evaluate your options given your start with attention to detail during case By outlining typically used Invisalign approaches Invisalign experience level. See Figure A, below. selection and treatment planning. Here are and discussing their complexity and predict- five guidelines for setting up your cases that ABOUT THIS SERIES ability, we hope to make the treatment planning pay great dividends later: This guide is the first in a three-part series options and implications more clear for you of Invisalign patient care references, comple- to evaluate. 1. Submit high quality records. Accurate menting the ClinCheck® Evaluation Guide PVS impressions and clear patient photos and (D4458) and the Invisalign Clinical Monitoring Align Technology is not a provider of medical, radiographs are critical for the creation of your Guide (D4219). -

Director's Remarks
The British Orthodontic Society Clinical Effectiveness Bulletin No.33 November 2014 Clinical Governance Directorate of the British Orthodontic Society Director’s Remarks Moving House! lthough this is the autumn edition of the 1st Prize Clinical Effectiveness Bulletin, I think there An audit of compliance in Orthodontics with has been something of a spring clean within Department of Health 2007 “Smokefree and A Smiling” guidance. the editorial ranks. This edition has been jointly produced by Kate House, the outgoing editor, and A.McMullin and S. Caldwell (University Dental Jadbinder Seehra, our new incoming editor. The Hospital Manchester). team have worked hard to produce an excellent Bulletin with an interesting range of articles. There 2nd Prize are some familiar themes again, patient satisfaction Use of the PAR index to assess outcomes of and multidisciplinary care, but some more varied orthognathic surgery in cleft lip and palate patients. projects looking at the periodontal health of our C. Rolland (VT dentist), C. Chambers (Bristol patients and their dietary habits, reflecting the wider Dental Hospital) and S. Deacon (Frenchay Hospital scope of our practice. and Bristol Dental Hospital). Knowing that audit is strong within our specialty, 3rd Prize I was interested to read that the Healthcare Quality Orthodontic treatment and orthognathic surgery – Improvement Partnership (HQIP), the organisation do we predict the length of treatment accurately? tasked with promoting quality in healthcare, in C. Dunbar, G. McIntyre (Dundee Dental Hospital) particular increasing the impact that clinical audit and S. Laverick (Ninewells Hospital, Dundee). has on healthcare quality in England and Wales, recently promoted its second ‘Audit Awareness Many congratulations to all the winning authors. -
The Orthodontic Treatment of Class III Malocclusion with Anterior Cross Bite and Severe Deep Bite
Volume 31 Issue 1 Article 6 2020 The Orthodontic Treatment of Class III Malocclusion with Anterior Cross Bite and Severe Deep Bite Chieh Yang School of Dentistry, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; Department of Orthodontics, Dental Clinics, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan Yu-Chuan Tseng School of Dentistry, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; Department of Orthodontics, Dental Clinics, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan, [email protected] Follow this and additional works at: https://www.tjo.org.tw/tjo Part of the Orthodontics and Orthodontology Commons Recommended Citation Yang, Chieh and Tseng, Yu-Chuan (2020) "The Orthodontic Treatment of Class III Malocclusion with Anterior Cross Bite and Severe Deep Bite," Taiwanese Journal of Orthodontics: Vol. 31 : Iss. 1 , Article 6. DOI: 10.30036/TJO.201903_31(1).0006 Available at: https://www.tjo.org.tw/tjo/vol31/iss1/6 This Case Report is brought to you for free and open access by Taiwanese Journal of Orthodontics. It has been accepted for inclusion in Taiwanese Journal of Orthodontics by an authorized editor of Taiwanese Journal of Orthodontics. Case Report THE ORTHODONTIC TREATMENT OF CLASS III MALOCCLUSION WITH ANTERIOR CROSS BITE AND SEVERE DEEP BITE Chieh Yang, Yu-Chuan Tseng School of Dentistry, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan Department of Orthodontics, Dental Clinics, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan This 22-year-old female presents with skeletal Class III malocclusion, complicated by anterior cross bite, deep bite, and congenital missing of bilateral mandibular second premolars. The treatment modality was full- mouth fixed edgewise appliances. -

Correcting Posterior Crossbites Complicated by Class III Malocclusions (A New Technique) Suhail A
Dental, Oral and Craniofacial Research Research Article ISSN: 2058-5314 Correcting posterior crossbites complicated by class III malocclusions (A new technique) Suhail A. Khouri* Orthodontist, Ballwin, Missouri, USA Abstract TThe objective of this study is to introduce a simplified alternative approach to the current modality used in posterior crossbites correction. It is believed that the interlocking relation of posterior teeth cusps, prevents transverse forces of the palatal expanders from eliciting the desired movement, rendering the crossbite correction an oranous task for orthodontists. Thus eliminating this cuspal blockage constitutes a key step to developing a simpler approach for correction. This diagnostic concept has lead the way to formulating an alternative, and clinically convenient treatment technique that not only corrects posterior crossbites, but also effectively corrects the often coexisting class III malocclusion simultaneously. Building composite bite raisers on mandibular posterior teeth, along with the intrusive effects of the V-Bends on super elastic wires, disengage the blocked cusps of posterior teeth, stop the patient’s mandibular shifted occlusion making any transverse corrective forces more effective in moving the malposed teeth segments. This methodical and clinically applicable technique utilizes a solid force system that delivers expanding / constricting mechanics acting on buccal, rather than the palatal sides of posterior teeth, launched by placing lasting intraoral V-Bends on super elastic archwires, using the Bendistal Pliers*. Whereas these V-Bends create light and consistent, apically directed forces on both, mandibular and maxillary anterior teeth to intrude and disengage them for the class III correction, an equal and opposite side effect forces intrudes and disengages posterior teeth cusps helping the correction of posterior crossbites in the same time. -
Simultaneous Intrusion and Distalization Using Miniscrews in the Maxillary Tuberosity
©2016 JCO, Inc. May not be distributed without permission. www.jco-online.com Simultaneous Intrusion and Distalization Using Miniscrews in the Maxillary Tuberosity VICENTE JAVIER SADA GARRALDA, DDS, MSD ini-implants can be used to manage severe results, including such demanding movements as Mdental crowding without extractions and to intrusion and arch expansion or narrowing.11-13 correct minor jaw malpositions without ortho- In an open-bite case with a mild skeletal gnathic surgery,1-4 eliminating the need for extra- Class II pattern and excessive lower facial height, oral anchorage and patient cooperation. Intruding traction from both upper and lower mini-implants the posterior segments to correct an open bite by can improve the efficiency of orthodontic treat- mandibular autorotation—traditionally difficult to ment. Another possibility is to use simultaneous achieve without extruding the incisors—is now traction from the maxillary tuberosity and the possible with skeletal anchorage. maxillary anterior region to intrude and distalize In this method of treatment, if miniscrews the upper teeth, as described in this article. are placed in interradicular spaces, the buccal teeth cannot be distalized because the implants will act Placement Procedure as stops. If they are placed in the palate, a device can be used to generate intrusive or distalizing When a mini-implant is placed in the maxil- forces on the posterior teeth without interference lary tuberosity, any lack of primary stability will from the mini-implants,5-7 but there are other dis- require relocation of the implant to an area with advantages: the risk of perforating the nasal cav- better bone. -

2018 Written Exam Reading List
THE AMERICAN BOARD OF ORTHODONTICS WRITTEN EXAMINATION 2018 READING LIST JOURNAL ARTICLES 1. Semipermanent replacement of missing maxillary lateral incisors by Roberto Ciarlantini, mini-implant retained pontics: A follow-up study, American Journal of Birte Melsen Orthodontics & Dentofacial Orthopedics, Volume 151, Issue 5, Pages 989–994, May 2017 2. Evolving concepts of heredity and genetics in orthodontics, American David S. Carlson Journal of Orthodontics and Dentofacial Orthopedics, Volume 148, Issue 6, Pages 922–938, December 2015 3. Early orthodontic treatment for Class II malocclusion reduces the Badri chance of incisal trauma: Results of a Cochrane systematic review, Thiruvenkatachari, et American Journal of Orthodontics and Dentofacial Orthopedics, Volume al. 148, Issue 1, Pages 47–59, July 2015 4. Association of orthodontic force system and root resorption: A Marina G. Roscoe, et systematic review, American Journal of Orthodontics and Dentofacial al. Orthopedics, Volume 147, Issue 5, Pages 610–626, May 2015 5. Evolution of occlusion and temporomandibular disorder in orthodontics: Jeffrey P. Okeson Past, present, and future, American Journal of Orthodontics and Dentofacial Orthopedics, Volume 147, Issue 5, Supplement, Pages S216–S223, May 2015 6. Prevalence of peg-shaped maxillary permanent lateral incisors: A Fang Hua, et al. meta-analysis, American Journal of Orthodontics and Dentofacial Orthopedics, Volume 144, Issue 1, Pages 97–109, July 2013 7. Effect of remineralizing agents on white spot lesions after orthodontic Hong Chen, et al. treatment: A systematic review, American Journal of Orthodontics and Dentofacial Orthopedics, Volume 143, Issue 3, Pages 376–382.e3, March 2013 8. Effectiveness of MI Paste Plus and PreviDent fluoride varnish for Greg J. -

Souvenir Copy
Souvenir Copy November2015 BOSNEWSSUPPLEMENT 1 8th International Orthodontic Congress 8th International Orthodontic Congress November2015 BOSNEWSSUPPLEMENT 2 8th International Orthodontic Congress ExCeL London 27 – 30 September 2015 Huge thanks are due to: Dina Slater To the Executive of the And last, but not least, James Spencer Orthodontic Technicians a massive thanks to the My Organising Committee: Ann Wright Association 6,000 delegates, without whom there would not Alex Cash To the BOS Board of To the Session Chairs have been a Congress. Stephen Chadwick Trustees Guy Deeming To the Poster Presenters I hope you enjoy this Andrew DiBiase To the WFO Executive souvenir supplement. Nigel Fox Committee To the Educational Grant Trevor Hodge Recipients Jonathan Sandler Ama Johal To the Speakers Chairman, 8th IOC Ben Lewis To the Exhibitors and Simon Littlewood To the World Village Day Sponsors Rye Mattick organisers Tania Murphy To the Stewards Alison Murray To the Executive of the Kevin O’Brien Orthodontic National To the Programme Session Julian O’Neill Group for Dental Nurses Authors Rishma Shah and Therapists November2015 BOSNEWSSUPPLEMENT 3 8th International Orthodontic Congress Saturday 26 September 2015 Pre-Congress Course Contemporary Treatment for Missing Teeth in Growing Patients. Autotransplantation – The Natural Choice, The Royal College of Surgeons, London Dr Ewa Czochrowska and Dr Pawel Plakwicz What a great start to the 8th International Orthodontic Congress - a carefully presented inspirational course by Eva and Pawel following 20 years’ experience of working together as a passionate, if gently combative, expert team. Dr Pawel highlighted the importance of the venue since John Hunter completed the first recorded transplantation of a human canine tooth to grow within a cockerel’s comb – the results remain on display within the Hunterian Museum.