Genetic Variant in CACNA1C Is Associated with PTSD in Traumatized Police Officers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Cell Adhesion and Specificity
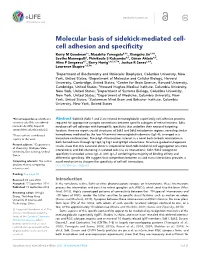
RESEARCH ARTICLE Molecular basis of sidekick-mediated cell- cell adhesion and specificity Kerry M Goodman1†, Masahito Yamagata2,3†, Xiangshu Jin1,4‡, Seetha Mannepalli1, Phinikoula S Katsamba4,5, Go¨ ran Ahlse´ n4,5, Alina P Sergeeva4,5, Barry Honig1,4,5,6,7*, Joshua R Sanes2,3*, Lawrence Shapiro1,5,7* 1Department of Biochemistry and Molecular Biophysics, Columbia University, New York, United States; 2Department of Molecular and Cellular Biology, Harvard University, Cambridge, United States; 3Center for Brain Science, Harvard University, Cambridge, United States; 4Howard Hughes Medical Institute, Columbia University, New York, United States; 5Department of Systems Biology, Columbia University, New York, United States; 6Department of Medicine, Columbia University, New York, United States; 7Zuckerman Mind Brain and Behavior Institute, Columbia University, New York, United States *For correspondence: bh6@cumc. Abstract Sidekick (Sdk) 1 and 2 are related immunoglobulin superfamily cell adhesion proteins columbia.edu (BH); sanesj@mcb. required for appropriate synaptic connections between specific subtypes of retinal neurons. Sdks harvard.edu (JRS); shapiro@ mediate cell-cell adhesion with homophilic specificity that underlies their neuronal targeting convex.hhmi.columbia.edu (LS) function. Here we report crystal structures of Sdk1 and Sdk2 ectodomain regions, revealing similar †These authors contributed homodimers mediated by the four N-terminal immunoglobulin domains (Ig1–4), arranged in a equally to this work horseshoe conformation. These Ig1–4 horseshoes interact in a novel back-to-back orientation in both homodimers through Ig1:Ig2, Ig1:Ig1 and Ig3:Ig4 interactions. Structure-guided mutagenesis Present address: ‡Department results show that this canonical dimer is required for both Sdk-mediated cell aggregation (via trans of Chemistry, Michigan State interactions) and Sdk clustering in isolated cells (via cis interactions). -

Supplementary Table 1: Adhesion Genes Data Set
Supplementary Table 1: Adhesion genes data set PROBE Entrez Gene ID Celera Gene ID Gene_Symbol Gene_Name 160832 1 hCG201364.3 A1BG alpha-1-B glycoprotein 223658 1 hCG201364.3 A1BG alpha-1-B glycoprotein 212988 102 hCG40040.3 ADAM10 ADAM metallopeptidase domain 10 133411 4185 hCG28232.2 ADAM11 ADAM metallopeptidase domain 11 110695 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 195222 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 165344 8751 hCG20021.3 ADAM15 ADAM metallopeptidase domain 15 (metargidin) 189065 6868 null ADAM17 ADAM metallopeptidase domain 17 (tumor necrosis factor, alpha, converting enzyme) 108119 8728 hCG15398.4 ADAM19 ADAM metallopeptidase domain 19 (meltrin beta) 117763 8748 hCG20675.3 ADAM20 ADAM metallopeptidase domain 20 126448 8747 hCG1785634.2 ADAM21 ADAM metallopeptidase domain 21 208981 8747 hCG1785634.2|hCG2042897 ADAM21 ADAM metallopeptidase domain 21 180903 53616 hCG17212.4 ADAM22 ADAM metallopeptidase domain 22 177272 8745 hCG1811623.1 ADAM23 ADAM metallopeptidase domain 23 102384 10863 hCG1818505.1 ADAM28 ADAM metallopeptidase domain 28 119968 11086 hCG1786734.2 ADAM29 ADAM metallopeptidase domain 29 205542 11085 hCG1997196.1 ADAM30 ADAM metallopeptidase domain 30 148417 80332 hCG39255.4 ADAM33 ADAM metallopeptidase domain 33 140492 8756 hCG1789002.2 ADAM7 ADAM metallopeptidase domain 7 122603 101 hCG1816947.1 ADAM8 ADAM metallopeptidase domain 8 183965 8754 hCG1996391 ADAM9 ADAM metallopeptidase domain 9 (meltrin gamma) 129974 27299 hCG15447.3 ADAMDEC1 ADAM-like, -

Longitudinal Genome-Wide Methylation Study of PTSD Treatment Using Prolonged Exposure and Hydrocortisone ✉ Ruoting Yang 1,4 , Changxin Xu2,4, Linda M
Translational Psychiatry www.nature.com/tp ARTICLE OPEN Longitudinal genome-wide methylation study of PTSD treatment using prolonged exposure and hydrocortisone ✉ Ruoting Yang 1,4 , Changxin Xu2,4, Linda M. Bierer2, Janine D. Flory2,3, Aarti Gautam1, Heather N. Bader2, Amy Lehrner2,3, Iouri Makotkine3, Frank Desarnaud3, Stacy A. Miller1, Marti Jett 1, Rasha Hammamieh1,5 and Rachel Yehuda2,3,5 © The Author(s) 2021 Epigenetic changes are currently invoked as explanations for both the chronicity and tenacity of post-traumatic stress disorder (PTSD), a heterogeneous condition showing varying, sometimes idiosyncratic responses to treatment. This study evaluated epigenetic markers in the context of a randomized clinical trial of PTSD patients undergoing prolonged-exposure psychotherapy with and without a hydrocortisone augmentation prior to each session. The purpose of the longitudinal epigenome-wide analyses was to identify predictors of recovery (from pretreatment data) or markers associated with symptom change (based on differences between pre- and post-therapy epigenetic changes). The results of these analyses identified the CREB–BDNF signaling pathway, previously linked to startle reaction and fear learning and memory processes, as a convergent marker predicting both symptom change and severity. Several previous-reported resilience markers were also identified (FKBP5, NR3C1, SDK1, and MAD1L1) to associate with PTSD recovery in this study. Especially, the methylation levels of FKBP5 in the gene body region decreased significantly as CAPS score decreased in responders, while no changes occurred in nonresponders. These biomarkers may have future utility in understanding clinical recovery in PTSD and potential applications in predicting treatment effects. Translational Psychiatry (2021) 11:398 ; https://doi.org/10.1038/s41398-021-01513-5 INTRODUCTION association with recovery, or that themselves change in associa- Plasticity of the epigenome is a mechanism through which tion with symptom severity. -

Towards Personalized Medicine in Psychiatry: Focus on Suicide
TOWARDS PERSONALIZED MEDICINE IN PSYCHIATRY: FOCUS ON SUICIDE Daniel F. Levey Submitted to the faculty of the University Graduate School in partial fulfillment of the requirements for the degree Doctor of Philosophy in the Program of Medical Neuroscience, Indiana University April 2017 ii Accepted by the Graduate Faculty, Indiana University, in partial fulfillment of the requirements for the degree of Doctor of Philosophy. Andrew J. Saykin, Psy. D. - Chair ___________________________ Alan F. Breier, M.D. Doctoral Committee Gerry S. Oxford, Ph.D. December 13, 2016 Anantha Shekhar, M.D., Ph.D. Alexander B. Niculescu III, M.D., Ph.D. iii Dedication This work is dedicated to all those who suffer, whether their pain is physical or psychological. iv Acknowledgements The work I have done over the last several years would not have been possible without the contributions of many people. I first need to thank my terrific mentor and PI, Dr. Alexander Niculescu. He has continuously given me advice and opportunities over the years even as he has suffered through my many mistakes, and I greatly appreciate his patience. The incredible passion he brings to his work every single day has been inspirational. It has been an at times painful but often exhilarating 5 years. I need to thank Helen Le-Niculescu for being a wonderful colleague and mentor. I learned a lot about organization and presentation working alongside her, and her tireless work ethic was an excellent example for a new graduate student. I had the pleasure of working with a number of great people over the years. Mikias Ayalew showed me the ropes of the lab and began my understanding of the power of algorithms. -

Epigenetic Biomarkers in Obesity, Weight Loss and Inflammation: a Role for Circadian Rhythm and Methyl Donors
Facultad de Farmacia y Nutrición Epigenetic biomarkers in obesity, weight loss and inflammation: a role for circadian rhythm and methyl donors Mirian Samblas García Pamplona, 2018 Facultad de Farmacia y Nutrición Memoria presentada por Dña. Mirian Samblas García para aspirar al grado de Doctor por la Universidad de Navarra. Mirian Samblas García El presente trabajo ha sido realizado bajo nuestra dirección en el Departamento de Ciencias de la Alimentación y Fisiología de la Facultad de Farmacia y Nutrición de la Universidad de Navarra y autorizamos su presentación ante el Tribunal que lo ha de juzgar. Pamplona, 26 de Febrero de 2018 VºBº Director VºBº Co-Director Dr. Fermín I. Milagro Yoldi Prof. J. Alfredo Martínez Hernández Este trabajo ha sido posible gracias a la financiación de diversas entidades: Ministerio de Economía y Competitividad (AGL2013-45554-R), Centro de Investigación Biomédica en Red de Fisiopatología de la Obesidad y Nutrición (CIBERObn), Instituo de Salud Carlos III (ISCIII), Centro de Investigación en Nutrición (Universidad de Navarra). La investigación que ha dado lugar a estos resultados ha sido impulsada por la beca predoctoral 2014-2015 del Centro de Investigación en Nutrición y las becas predoctoral 2015-2018 y de movilidad del Ministerio de Educación, Cultura y Deporte. “Necesitamos especialmente de la imaginación en las ciencias. No todo es matemáticas y no todo es simple lógica, también se trata de un poco de belleza y poesía” Maria Montessori Dedicado a las dos personas que me lo han dado todo, Mi aita Ray, Mi ama Ana Con especial cariño a, Mi hermana, Bea Mi sobrina, Aroa Mi abu, Esther Agradecimientos/Acknowledgements En estas líneas quisiera mostrar mi más sincero agradecimiento a todas aquellas personas e instituciones que han hecho posible la actual tesis. -

Global Identification of Hnrnp A1 Binding Sites for SSO-Based Splicing Modulation Gitte H
Bruun et al. BMC Biology (2016) 14:54 DOI 10.1186/s12915-016-0279-9 RESEARCH ARTICLE Open Access Global identification of hnRNP A1 binding sites for SSO-based splicing modulation Gitte H. Bruun1, Thomas K. Doktor1, Jonas Borch-Jensen1, Akio Masuda2, Adrian R. Krainer3, Kinji Ohno2 and Brage S. Andresen1* Abstract Background: Many pathogenic genetic variants have been shown to disrupt mRNA splicing. Besides splice mutations in the well-conserved splice sites, mutations in splicing regulatory elements (SREs) may deregulate splicing and cause disease. A promising therapeutic approach is to compensate for this deregulation by blocking other SREs with splice-switching oligonucleotides (SSOs). However, the location and sequence of most SREs are not well known. Results: Here, we used individual-nucleotide resolution crosslinking immunoprecipitation (iCLIP) to establish an in vivo binding map for the key splicing regulatory factor hnRNP A1 and to generate an hnRNP A1 consensus binding motif. We find that hnRNP A1 binding in proximal introns may be important for repressing exons. We show that inclusion of the alternative cassette exon 3 in SKA2 can be significantly increased by SSO-based treatment which blocks an iCLIP-identified hnRNP A1 binding site immediately downstream of the 5’ splice site. Because pseudoexons are well suited as models for constitutive exons which have been inactivated by pathogenic mutations in SREs, we used a pseudoexon in MTRR as a model and showed that an iCLIP-identified hnRNP A1 binding site downstream of the 5′ splice site can be blocked by SSOs to activate the exon. Conclusions: The hnRNP A1 binding map can be used to identify potential targets for SSO-based therapy. -

Exposure to Childhood Abuse Is Associated with Human Sperm DNA Methylation Andrea L
Roberts et al. Translational Psychiatry (2018) 8:194 DOI 10.1038/s41398-018-0252-1 Translational Psychiatry ARTICLE Open Access Exposure to childhood abuse is associated with human sperm DNA methylation Andrea L. Roberts 1, Nicole Gladish2,EvanGatev2,3, Meaghan J. Jones 2,YingChen4, Julia L. MacIsaac2, Shelley S. Tworoger4,5,S.BrynAustin6, Cigdem Tanrikut7, Jorge E. Chavarro4,5,8,AndreaA.Baccarelli9 and Michael S. Kobor 2,10 Abstract Offspring of persons exposed to childhood abuse are at higher risk of neurodevelopmental and physical health disparities across the life course. Animal experiments have indicated that paternal environmental stressors can affect sperm DNA methylation and gene expression in an offspring. Childhood abuse has been associated with epigenetic marks in human blood, saliva, and brain tissue, with statistically significant methylation differences ranging widely. However, no studies have examined the association of childhood abuse with DNA methylation in gametes. We examined the association of childhood abuse with DNA methylation in human sperm. Combined physical, emotional, and sexual abuse in childhood was characterized as none, medium, or high. DNA methylation was assayed in 46 sperm samples from 34 men in a longitudinal non-clinical cohort using HumanMethylation450 BeadChips. We performed principal component analysis and examined the correlation of principal components with abuse exposure. Childhood abuse was associated with a component that captured 6.2% of total variance in DNA methylation (p < 0.05). Next, we investigated the regions differentially methylated by abuse exposure. We identified 12 DNA regions differentially methylated by childhood abuse, containing 64 probes and including sites on genes associated with 1234567890():,; 1234567890():,; 1234567890():,; 1234567890():,; neuronal function (MAPT, CLU), fat cell regulation (PRDM16), and immune function (SDK1). -

Initiation of Antiviral B Cell Immunity Relies on Innate Signals from Spatially Positioned NKT Cells
Initiation of Antiviral B Cell Immunity Relies on Innate Signals from Spatially Positioned NKT Cells The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters. Citation Gaya, Mauro et al. “Initiation of Antiviral B Cell Immunity Relies on Innate Signals from Spatially Positioned NKT Cells.” Cell 172, 3 (January 2018): 517–533 © 2017 The Author(s) As Published http://dx.doi.org/10.1016/j.cell.2017.11.036 Publisher Elsevier Version Final published version Citable link http://hdl.handle.net/1721.1/113555 Terms of Use Creative Commons Attribution 4.0 International License Detailed Terms http://creativecommons.org/licenses/by/4.0/ Article Initiation of Antiviral B Cell Immunity Relies on Innate Signals from Spatially Positioned NKT Cells Graphical Abstract Authors Mauro Gaya, Patricia Barral, Marianne Burbage, ..., Andreas Bruckbauer, Jessica Strid, Facundo D. Batista Correspondence [email protected] (M.G.), [email protected] (F.D.B.) In Brief NKT cells are required for the initial formation of germinal centers and production of effective neutralizing antibody responses against viruses. Highlights d NKT cells promote B cell immunity upon viral infection d NKT cells are primed by lymph-node-resident macrophages d NKT cells produce early IL-4 wave at the follicular borders d Early IL-4 wave is required for efficient seeding of germinal centers Gaya et al., 2018, Cell 172, 517–533 January 25, 2018 ª 2017 The Authors. Published by Elsevier Inc. https://doi.org/10.1016/j.cell.2017.11.036 Article Initiation of Antiviral B Cell Immunity Relies on Innate Signals from Spatially Positioned NKT Cells Mauro Gaya,1,2,* Patricia Barral,2,3 Marianne Burbage,2 Shweta Aggarwal,2 Beatriz Montaner,2 Andrew Warren Navia,1,4,5 Malika Aid,6 Carlson Tsui,2 Paula Maldonado,2 Usha Nair,1 Khader Ghneim,7 Padraic G. -

RNA-Seq Analysis of Prostate Cancer in the Chinese Population Identifies Recurrent Gene Fusions, Cancer-Associated Long Noncodin
npg RNA-seq analysis of prostate cancer in Chinese population Cell Research (2012) 22:806-821. 806 © 2012 IBCB, SIBS, CAS All rights reserved 1001-0602/12 $ 32.00 npg ORIGINAL ARTICLE www.nature.com/cr RNA-seq analysis of prostate cancer in the Chinese population identifies recurrent gene fusions, cancer-associated long noncoding RNAs and aberrant alternative splicings Shancheng Ren1, *, Zhiyu Peng2, *, Jian-Hua Mao3, *, Yongwei Yu4, Changjun Yin5, Xin Gao6, Zilian Cui1, Jibin Zhang2, Kang Yi2, Weidong Xu1, Chao Chen2, Fubo Wang1, Xinwu Guo2, Ji Lu1, Jun Yang2, Min Wei1, Zhijian Tian2, Yinghui Guan3, Liang Tang1, Chuanliang Xu1, Linhui Wang1, Xu Gao1, Wei Tian2, Jian Wang2, Huanming Yang2, Jun Wang2, Yinghao Sun1 1Department of Urology, Shanghai Changhai Hospital, Second Military Medical University, Shanghai 200433, China; 2Beijing Ge- nomics Institute at Shenzhen, Shenzhen, Guangdong 518083, China; 3Life Sciences Division, Lawrence Berkeley National Labora- tory, One Cyclotron Road, Berkeley, CA 94720, USA; 4Department of Pathology, Shanghai Changhai Hospital, Second Military Medical University, Shanghai 200433, China; 5Department of Urology, Jiangsu Provincial People’s Hospital, Nanjing Medical University, Nanjing, Jiangsu 210029, China; 6Department of Urology, the Third Affiliated Hospital of Sun Yat Sen University, Guangzhou, Guangdong 510630, China There are remarkable disparities among patients of different races with prostate cancer; however, the mechanism underlying this difference remains unclear. Here, we present a comprehensive landscape of the transcriptome profiles of 14 primary prostate cancers and their paired normal counterparts from the Chinese population using RNA-seq, revealing tremendous diversity across prostate cancer transcriptomes with respect to gene fusions, long noncoding RNAs (long ncRNA), alternative splicing and somatic mutations. -
A Chromosome-Centric Human Proteome Project (C-HPP) To
computational proteomics Laboratory for Computational Proteomics www.FenyoLab.org E-mail: [email protected] Facebook: NYUMC Computational Proteomics Laboratory Twitter: @CompProteomics Perspective pubs.acs.org/jpr A Chromosome-centric Human Proteome Project (C-HPP) to Characterize the Sets of Proteins Encoded in Chromosome 17 † ‡ § ∥ ‡ ⊥ Suli Liu, Hogune Im, Amos Bairoch, Massimo Cristofanilli, Rui Chen, Eric W. Deutsch, # ¶ △ ● § † Stephen Dalton, David Fenyo, Susan Fanayan,$ Chris Gates, , Pascale Gaudet, Marina Hincapie, ○ ■ △ ⬡ ‡ ⊥ ⬢ Samir Hanash, Hoguen Kim, Seul-Ki Jeong, Emma Lundberg, George Mias, Rajasree Menon, , ∥ □ △ # ⬡ ▲ † Zhaomei Mu, Edouard Nice, Young-Ki Paik, , Mathias Uhlen, Lance Wells, Shiaw-Lin Wu, † † † ‡ ⊥ ⬢ ⬡ Fangfei Yan, Fan Zhang, Yue Zhang, Michael Snyder, Gilbert S. Omenn, , Ronald C. Beavis, † # and William S. Hancock*, ,$, † Barnett Institute and Department of Chemistry and Chemical Biology, Northeastern University, Boston, Massachusetts 02115, United States ‡ Stanford University, Palo Alto, California, United States § Swiss Institute of Bioinformatics (SIB) and University of Geneva, Geneva, Switzerland ∥ Fox Chase Cancer Center, Philadelphia, Pennsylvania, United States ⊥ Institute for System Biology, Seattle, Washington, United States ¶ School of Medicine, New York University, New York, United States $Department of Chemistry and Biomolecular Sciences, Macquarie University, Sydney, NSW, Australia ○ MD Anderson Cancer Center, Houston, Texas, United States ■ Yonsei University College of Medicine, Yonsei University, -

Dependent Protein Kinase CPK3 Is Required for Sphingolipid-Induced Cell Death in Arabidopsis
Cell Death and Differentiation (2013) 20, 209–217 & 2013 Macmillan Publishers Limited All rights reserved 1350-9047/13 www.nature.com/cdd 14-3-3-Regulated Ca2 þ -dependent protein kinase CPK3 is required for sphingolipid-induced cell death in Arabidopsis C Lachaud1,2,3,4, E Prigent1,2,4, P Thuleau1,2, S Grat1,2, D Da Silva1,2, C Brie`re1,2, C Mazars1,2 and V Cotelle*,1,2 In eukaryotic cells, sphingoid long chain bases (LCBs) such as sphingosine or phytosphingosine (PHS) behave as second messengers involved in various processes including programmed cell death (PCD). In plants, induction of PCD by LCBs has now been described, but the signalling pathway is still enigmatic. Using Arabidopsis, we identify new key steps in this pathway. We demonstrate that PHS induces activation of the calcium-dependent kinase CPK3, which phosphorylates its binding partners, the 14-3-3 proteins. This phosphorylation leads to the disruption of the complex and to CPK3 degradation. Using cpk3 knockout lines, we demonstrate that CPK3 is a positive regulator of LCB-mediated PCD. These findings establish 14-3-3-regulated CPK3 as a key component of the LCB pathway leading to PCD in plants. Cell Death and Differentiation (2013) 20, 209–217; doi:10.1038/cdd.2012.114; published online 31 August 2012 In eukaryotes, programmed cell death (PCD) is an integral sphingosine-dependent kinase 1 (SDK1), identified as the component of development and defence responses to various caspase-cleaved fragment of protein kinase C (PKC)d,12,13 stresses.1,2 PCD in animal cells is a complex -

SKA2 Methylation Is Associated with Decreased Prefrontal Cortical
SKA2 methylation is associated with decreased prefrontal cortical thickness and greater PTSD severity among trauma-exposed veterans Naomi Sadeh, VA Boston Healthcare System Jeffrey M. Spielberg, Boston University Mark W. Logue, VA Boston Healthcare System Erika J. Wolf, VA Boston Healthcare System Alicia K Smith, Emory University Joanna Lusk, VA Boston Healthcare System Jasmeet P. Hayes, VA Boston Healthcare System Emily Sperbeck, VA Boston Healthcare System William P. Milberg, VA Boston Healthcare System Regina E. McGlinchey, VA Boston Healthcare System Only first 10 authors above; see publication for full author list. Journal Title: Molecular Psychiatry Volume: Volume 21, Number 3 Publisher: Nature Publishing Group | 2016-03-01, Pages 357-363 Type of Work: Article | Post-print: After Peer Review Publisher DOI: 10.1038/mp.2015.134 Permanent URL: https://pid.emory.edu/ark:/25593/rptgj Final published version: http://dx.doi.org/10.1038/mp.2015.134 Copyright information: © 2016 Macmillan Publishers Limited. Accessed September 28, 2021 9:19 PM EDT HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Mol Psychiatry Manuscript Author . Author Manuscript Author manuscript; available in PMC 2016 May 18. Published in final edited form as: Mol Psychiatry. 2016 March ; 21(3): 357–363. doi:10.1038/mp.2015.134. SKA2 Methylation is associated with Decreased Prefrontal Cortical Thickness and Greater PTSD Severity among Trauma- Exposed Veterans Naomi Sadeh, Ph.D.1,3, Jeffrey M. Spielberg, Ph.D.2,3, Mark W. Logue, Ph.D.4, Erika J. Wolf, Ph.D.1,3, Alicia K. Smith, Ph.D.5, Joanna Lusk, B.A.1, Jasmeet P.