Supaul, Bihar DISTRICT DEMOGRAPHIC PROFILE1 Total Population 2,229,076
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bihar Military Police (BMP
FORM 1 (I) Basic Information Sl.No. Item Details 1. Name of the project/s-Bihar Military Police (B.M.P- Bihar Govt. Project 12)Supaul 2. S.No. in the schedule 3. Proposed capacity /area/length/tonnage to be Plot area=283382 sq.m handled/command area/lease area/number of wells to be TotalBuilt up drilled. area=31190.65sq.m 4. New/Expansion/Modernization NEW 5. Existing Capacity/Area etc. NIL 6. Category of Project i.e. ‘A’ or ‘B’ B 7. Does it attract the general condition? If yes, please specify. NO 8. Does it attract the specific condition? If yes, please specify. YES 9. Location - Supaul Thana no.-1 Plot/Survey/Khasra No. Khata no.-339 Village - Birpur Kesra no.-1020 Tehsil- BASHAANTPUR District SUPAUL,MAUJA-BHIMNAGAR State - BIHAR 10. Nearest railway station/airport along with distance in kms. 32kmRadhupur ( railway station) 11. Nearest Town, city, district Headquarters along with 62 km. Supaul Head Quarter distance in kms. 12. Village Panchayats, Zilla Parishad, Municipal Corporation, Birpur,Bhimnagar. Local body (complete postal addresses with telephone nos. supaul to be given) 13. Name of the applicant Dhananjay kumar (Senior Architect) 14. Registered Address Kautaliya nagar patna -14 15. Address for correspondence: Bihar police Building Name cconstruction corporation Designation (Owner/Partner /CEO) Sunil kumar. Pin code ADG CUM CMD E-mail 800014 Telephone No. [email protected] Fax No. 0612-2224529 0612-2224529 16. Details of Alternative Sites examined, if any. Location of Village-District-State these sites should be shown on a topo sheet. 1 NIL 2 3 17. -

District Plan 2011 - 12
I DISTRICT PLAN 2011 - 12 SUPAUL - i I Submitted by : District Planning Committee, Supaul Submitted to: Department of Planning & Development, Government of Bihar DISTRICT PLAN 2011 - 12 SUPAUL ¥ V *k g f II A © H f: © f&T SJkH*»»* Submitted by : District Planning Committee, Supaul Submitted to: Department of Planning & Development, Government of Bihar ACKNOWLEDGEMENTS For sustainable and planned economic development it is essential to formulate the Annual District Plan on the basis of available resources. As per the direction of the Department of Planning and Development, Government of Bihar, with an objective to prepare the effective Plan, we have collected relevant information and data ensuring the assimilation of district level important components from various departments as well as the priority sectors like Health, Education, Livelihood and Infrastructure etc. Keeping in view the past experience of formulation and implementation of various sectoral Action Annual Plans and recent directions of the department the Annual District Plan 2011 -12 for Rs. 103142.3 89 lakh has been prepared for the maximum utilization of available resources, so that the socio-economic development of the district can be further accelerated. I would like to thank Mr. Kunwar Jung Bahadur, Deputy Development Commissioner, Mr. D.N. Mishra, Regional Planning officer, Kosi Division, Mr. Prakash Yadav, District Planning Officer, Mr. Vivek Sharan (Ex. District Facihtator) and Mr. D P Karn, District Facihtator, GoI-UN Joint Convergence Program for their important contribution in formulation of Annual District Plan 2011 -12 for the district of Supaul. Mr. Brajesh Kumar Vikal, DPRO also deserves special thanks for his support in the Plan formulation. -
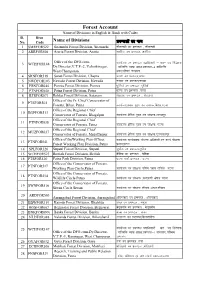
List of Forest Divisions with Code
Forest Account Name of Divisions in English & Hindi with Codes Sl. Divn No. Code Name of Divisions ize.Myksa dk uke 1 SMRFOR522 Sitamarhi Forest Division, Sitamarhi lhrke<h ou izze.My ] lhrke<h 2 ARRFOR504 Araria Forest Division, Araria vjfj;k ou ize.My] vjfj;k Office of the DFO-cum- 3 WCHFOR148 dk;kZy; ou ize.My inkf/kdkjh & lg& mi funs'kd Dy.Director,V.T.P.-2, Valmikinagar, okfYefd O;k?kz vkj{k]ize.My&2 okfYefd West Champaran uxj]if'pe pEikj.k 4 SRNFOR518 Saran Forest Division, Chapra lkj.k ou ize.My]Nijk 5 NWDFOR103 Nawada Forest Division, Nawada uoknk ou ize.My]uoknk 6 PRNFOR044 Purnea Forest Division, Purnea iwf.kZ;kWa ou izze.My ]iwf.kZ;kWa 7 PTNFOR040 Patna Forest Division, Patna iVuk ou izze.My ]iVuk 8 RTSFOR071 Rohtas Forest Division, Sasaram jksgrkl ou izze.My ] jksgrkl Office of the Pr. Chief Conservator of 9 PTSFOR501 Forests, Bihar, Patna dk;kZy;]iz/kku eq[; ou laj{kd]fcgkj]iVuk Office of the Regional Chief 10 BGPFOR513 Conservator of Forests, Bhagalpur dk;kZy; {kssf=; eq[; ou laj{kd]Hkkxyiqj Office of the Regional Chief 11 PTNFOR038 Conservator of Forests, Patna dk;kZy; {kssf=; eq[; ou laj{kd] iVuk Office of the Regional Chief 12 MUZFOR037 Conservator of Forests, Muzaffarpur dk;kZy; {ksf=; eq[; ou laj{kd]etq Q~Qjiqj Office of theWorking Plan Officer, dk;kZy; dk;Zokgd ;kstuk vf/kdkjh]ou dk; Z ;kstuk 13 PTNFOR041 Forest Working Plan Division, Patna izHkkx]iVuk 14 SPLFOR526 Supaul Forest Division, Supaul lqikSy ou ize.My]lqikSy 15 WCHFOR523 Bettiah Forest Division, Bettiah csfr;k ou izze.My ] csfr;k 16 PTSFOR530 Patna Park -

Deo List Bihar
Details of DEO-cum-DM Sl. No. District Name Name Designation E-mail Address Mobile No. 1 2 3 4 5 6 1 PASCHIM CHAMPARAN Kundan Kumar District Election Officer [email protected] 9473191294 2 PURVI CHAMPARAN Shirsat Kapil Ashok District Election Officer [email protected] 9473191301 3 SHEOHAR Avaneesh Kumar Singh District Election Officer [email protected] 9473191468 4 SITAMARHI Abhilasha Kumari Sharma District Election Officer [email protected] 9473191288 5 MADHUBANI Nilesh Ramchandra Deore District Election Officer [email protected] 9473191324 6 SUPAUL Sri Mahendra KUMAR District Election Officer [email protected] 9473191345 7 ARARIA Prashant Kumar District Election Officer [email protected] 9431228200 8 KISHANGANJ Aditya Prakash District Election Officer [email protected] 9473191371 9 PURNIA Rahul Kumar District Election Officer [email protected] 9473191358 10 KATIHAR Kanwal Tanuj District Election Officer [email protected] 9473191375 11 MADHEPURA Navdeep Shukla District Election Officer [email protected] 9473191353 12 SAHARSA Kaushal kumar District Election Officer [email protected] 9473191340 13 DARBHANGA Shri Thiyagrajan S. M. District Election Officer [email protected] 9473191317 14 MUZAFFARPUR Chandra Shekhar Singh District Election Officer [email protected] 9473191283 15 GOPALGANJ Arshad Aziz District Election Officer [email protected] 9473191278 16 SIWAN Amit Kumar Pandey District Election Officer [email protected] 9473191273 17 SARAN Subrat Kumar Sen District -
Observed Rainfall Variability and Changes Over Bihar State
CLIMATE RESEARCH AND SERVICES INDIA METEOROLOGICAL DEPARTMENT MINISTRY OF EARTH SCIENCES PUNE Observed Rainfall Variability and Changes over Bihar State Met Monograph No. : ESSO/IMD/HS/Rainfall Variability/04(2020)/28 Pulak Guhathakurta, Sudeepkumar B L, Preetha Menon, Ashwini Kumar Prasad, Neha Sangwan and S C Advani GOVERNMENT OF INDIA MINISTRY OF EARTH SCIENCES INDIA METEOROLOGICAL DEPARTMENT Met Monograph No.: ESSO/IMD/HS/Rainfall Variability/04(2020)/28 Observed Rainfall Variability and Changes Over Bihar State Pulak Guhathakurta, Sudeepkumar B L, Preetha Menon, Ashwini Kumar Prasad, Neha Sangwan and S C Advani INDIA METEOROLOGICAL DEPARTMENT PUNE - 411005 1 DOCUMENT AND DATA CONTROL SHEET 1 Document Title Observed Rainfall Variability and Changes Over Bihar State 2 Issue No. ESSO/IMD/HS/Rainfall Variability/04(2020)/28 3 Issue Date January 2020 4 Security Unclassified Classification 5 Control Status Uncontrolled 6 Document Type Scientific Publication 7 No. of Pages 27 8 No. of Figures 42 9 No. of References 4 10 Distribution Unrestricted 11 Language English 12 Authors Pulak Guhathakurta, Sudeepkumar B L, Preetha Menon, Ashwini Kumar Prasad, Neha Sangwan and S C Advani 13 Originating Division/ Climate Research Division/ Climate Application & Group User Interface Group/ Hydrometeorology 14 Reviewing and Director General of Meteorology, India Approving Authority Meteorological Department, New Delhi 15 End users Central and State Ministries of Water resources, agriculture and civic bodies, Science and Technology, Disaster Management Agencies, Planning Commission of India 16 Abstract India is in the tropical monsoon zone and receives plenty of rainfall as most of the annual rainfall during the monsoon season every year. However, the rainfall is having high temporal and spatial variability and due to the impact of climate changes there are significant changes in the mean rainfall pattern and their variability as well as in the intensity and frequencies of extreme rainfall events. -

Nepali Times
#421 17 - 23 October 2008 16 pages Rs 30 Weekly Internet Poll # 421 Q. Do you expect next year’s Dasain- Tihar to be better than this year’s? Total votes: 5,319 Weekly Internet Poll # 422. To vote go to: www.nepalitimes.com Q. Do you think it is a good idea for the NC to join the Maoist-led coalition? EDWIN KOO RIVER TO DESERT: Just 1.5 km upstream from the Kosi Barrage in Saptari, a bull wades through stagnant water. This is where the Kosi used to flow before it suddenly breached its embankment and changed course. See also: ‘Water world’, p 8-9. combatants. But the real unknown is whether Dahal can sell that plan to his guerrilla commanders in UN-supervised cantonments. Back to work Meanwhile, there are indications of further mellowing The government has a lot of catching up to do of the Maoist line. Finance Minister Baburam Bhattarai, he friendly mood of the Although sharp differences a consensus government. attending the World Bank/IMF festive season seems to have remain, both within parties in the “We need everyone on board annual meeting in Washington Taffected the top leaders of coalition and among each other, to fulfill our immediate goals of this week, surprised people there the NC and the Maoists, who have there seems to be a realisation that keeping the peace process on and in Nepal by saying his party been using tea party diplomacy progress on governance and track, to draft a new constitution was discussing dropping ‘Maoist’ this week to patch up differences. -

Geomorphological Studies and Flood Risk Assessment of Kosi River Basin Using Remote 2011-13 Sensing and Gis Techniques
Contents List of Tables ............................................................................................................................... 4 Lists of Figures ............................................................................................................................ 5 1. Introduction ........................................................................................................................ 7 1.1 General .......................................................................................................................... 7 1.2 Flood Risk Concept ....................................................................................................... 7 1.3 Background and Motivation ....................................................................................... 12 1.4 Research Questions and Objectives ............................................................................ 13 1.5 Study Area .................................................................................................................. 14 1.6 Organization of Thesis Chapters ................................................................................. 14 2. Literature Review ............................................................................................................. 16 2.1 General ........................................................................................................................ 16 2.2 Geomorphic Controls of Floods ................................................................................. -

Flood Disaster and Its Impact on the People in Kosi Region, Bihar
© 2019 IJRAR May 2019, Volume 6, Issue 2 www.ijrar.org (E-ISSN 2348-1269, P- ISSN 2349-5138) FLOOD DISASTER AND ITS IMPACT ON THE PEOPLE IN KOSI REGION, BIHAR Dr. Sanjiv Kumar Research Fellow Univ. Deptt. of Geography, T.M.B.U., Bhagalpur Introduction The Kosi, a trans-boundary river between Nepal and India is often referred to as the “Sorrow of Bihar”. The flow of the river contains excessive silt and sand, resulting in changing the courses of the river. During the past, the river has kept on changing its courses between Purnea district in the east and Darbhanga and Madhubani districts in the west. The recent disaster was created by the breach in the eastern Kosi embankment upstream of the Indian border at Kursela in the neighbouring Nepal on the 18th of August 2008. A tragedy of unparalleled dimension unleashed was over three million people living in 995 villages spreading in seven districts of Kosi region, viz. Supaul, Araria, Madhepura, Saharsa, Purnia, Khagaria and Katihar. Objectives: The purpose of the paper is to investigate the damage caused by the devastating floods due to the turbulent river Kosi recurrently and its impact on the socio-economic life of the people inhabiting in the region which is densely populated but with poor economy. The objective refers to the sustainability of an agricultural region to the occurrence of a natural disaster. The objective is to achieve in order to create a sustainable system in environmental, social and economic terms. The other objective aims to preserve or improve characteristics of the environment such as biodiversity, soil, and water and air quality. -

Journal Volume 19, June-July 2018
Journal Volume 19, June-July 2018 INDEX Sr. Page Name of the Research Paper Author No. No. 1 Ecological Light Pollution- Causes And Effects Arunima Bhattacharya 1-4 Genesis And Morphology of Coastal Potholes and Depressions : 2 Dr. Ajay Kamble 5-10 A Case Study From North Konkan, Maharashtra Analysis of Trends And Causes For Variations of Fluvial Dynamics Dr. Rajesh Kumar Mahato 3 And Sedimentation Behavior In Sapt Kosi River Basin of Bihar 11-17 Dr. Satyapriya Mahato Plain (India) And Mountainous Region of Eastern Nepal. Spatial Variations in Agricultural Productivity of Koppal District in 4 Dr. Basavaraj R. Bagade 18-23 Karnataka State Samsul Hoque Chronological and Chorological Dimensions of Literacy in Malda 5 A K M Anwaruzzaman 24-30 District with Special Reference to Gender Gap Nuruzzaman Kasemi Impact of PMGSY on Socio-Economic Development : A Case Rentu Biswas 6 Study of Chandpur- Kushabaria Road, MurshidabadTHE KOKAN GEOGRAPHERDistrict, West 31-39 A K M Anwaruzzaman Bengal Impact of Irrigation on Agricultural Productivity of Boro Paddy in 7 Subhasis Mondal 40-47 Bolpur Sub- Division Industrial Scenario and Potentialities of Industrial Development of Dr. Sanjib Majumder 8 Hooghly Industrial Region With Special Reference to Hooghly 48-55 Sandip Saha District Nanasaheb P. Kamble Survey of Avian Diversity in Selected Area (Kudal And Kankavli Bhagyashri K. Parab 9 56-60 Taluka) of Sindhudurg District, Maharashtra State, India Manish M. Joil Janvi P. Keluskar A Geographical Perspective of Spatio –Temporal Trend In Sex 10 Mr. Shridhar Pednekar 61-65 Ratio A Study Of Palghar District: 1981-2011‟ Kavita Saini 11 Spatio- Temporal Analysis of Social Crimes in Haryana 66-69 Sunil Kumar 12 jktLFkku esa i;ZVu % ,d fo'ys"k.kkRed v/;;u Dr. -

Master Plan of Agricultural Marketing in Eastern Development Region of Nepal
MASTER PLAN OF AGRICULTURAL MARKETING IN EASTERN DEVELOPMENT REGION OF NEPAL Final Report Submitted To Government of Nepal Ministry of Agricultural Development Department of Agriculture Agri. Business Promotion & Marketing Development Directorate (ABPMDD) Harihar Bhawan, Lalitpur Submitted By: Business Promotion Research and Communication Pvt. Ltd., (BPRC) Putalisadak, Kathmandu, Nepal Tel # 0977-01-4442853/4436617, Fax # 0977-01-4436617 Post Box # 19006, Email # [email protected] July 2017 (Ashad, 2074) Preface BPRC is pleased to undertake this Study "Master Plan of Agri-Marketing in Eastern Development Region of Nepal". BPRC expresses its gratitude to Agri Business Promotion and Marketing Development Directorate (ABPMDD) to having entrusted this important task. It also expresses gratitude to Mr. Laxman Prasad Paudel, Program Director and his team for expert guidance and for providing suggestions throughout the study period and report writing. BPRC is also thankful to ABDMDD team for their valuable, constructive comments and suggestions which were provided during Inception report and draft report presentations. We also express graduate to Senior Agriculture Marketing Officers Mr. Rajendra Prasad Pradhan and Mr. Puspa Raj Shahi for providing necessary instructions during final report preparation. BPRC acknowledges with gratitude the contribution made by study team of the project, with their valuable contribution the project was successfully brought to its conclusion. BPRC is most grateful to Mrs. Naina Dhakal, Team Leader for the successful execution of this project and for steering the whole tasks of conducting field study till its conclusion. In addition, BPRC conveys its appreciation to the contribution made by Chief and SMS of District Agriculture Development Offices, Agro-Vets, Traders, Wholesalers, Representative of District Development Committee, Member of Market Management Committee, Commercial Farmers Representatives and Agri-Cooperatives etc. -
Multiscale Integrated River Basin Management from a Hindu Kush Himalayan Perspective RESOURCE BOOK
RESOURCE BOOK Multiscale Integrated River Basin Management From a Hindu Kush Himalayan perspective RESOURCE BOOK Published by Multiscale International Centre for Integrated Mountain Development GPO Box 3226, Kathmandu, Nepal Integrated River ISBN 978 92 9115 6818 (printed) Copyright © 2019 978 92 9115 6825 (online) Basin Management International Centre for Integrated Mountain Production team Development (ICIMOD) A Beatrice Murray (Consultant editor) From a Hindu Kush Himalayan This work is licensed under a Creative Commons Samuel Thomas (Senior editor) perspective Attribution Non-Commercial, No Derivatives 4.0 Rachana Chettri (Editor) International License Kundan Shrestha (Editor) Mohd Abdul Fahad (Graphic designer) (https://creativecommons.org/licenses/by-nc-nd/4.0/) Anil Kumar Jha (Editorial assistance) Editors Note Photos: This publication may be reproduced in whole or in part Santosh Nepal, Arun B Shrestha, Chanda G Goodrich, Alex Treadway: pp iii, iv-v, vii, viii-ix, 2, 5, 7, 9, 11, 25, 30-31, and in any form for educational or nonprofit purposes Arabinda Mishra, Anjal Prakash, Sanjeev Bhuchar, 32-33, 44-45, 46-47, 48, 50-51, 52-53, 54-55, 56-57, 58-59, 63, without special permission from the copyright holder, Laurie A Vasily, Vijay Khadgi, Neera S Pradhan provided acknowledgement of the source is made. 68-69, 70-71, 73, 74, 77, 81, 84-85, 94-95, 96-97, 98-99, 101, ICIMOD would appreciate receiving a copy of any 111, 113, 117, 136, 148, 157, 165, 169, 186-187; publication that uses this publication as a source. No ICIMOD archive: pp 123, 132-133, 135, 139, 170; use of this publication may be made for resale or for any Jalal Naser Faqiryar: Cover, pp 18-19, 29, 86-87, 90-91, 126- other commercial purpose whatsoever without prior 127, 128-129, 140-141; permission in writing from ICIMOD. -

World Bank Document
MINISTRY OF ROAD TRANSPORT & HIGHWAY GOVERNMENT OF INDIA Public Disclosure Authorized CONSULTANCY SERVICES FOR DETAILED PROJECT REPORT FOR REHABILITATION AND UPGRADING TO 2 LANE/2 LANE WITH PAVED SHOULDER OF BIRPUR TO BIHPUR SECTION OF NH-106 (KM 0. 000 TO KM 136.00) (BIHAR) Package I SOCIAL IMPACT ASSESSMENT& RAP REPORT Public Disclosure Authorized Public Disclosure Authorized February – 2014 Public Disclosure Authorized Up gradation of Birpur- Bihpur Section of NH 106 in the State of Bihar Social Impact Assessment & RAP Social Impact Assessment & RAP Report (FINAL) TABLE OF CONTENTS S. Description Page No ABBREVIATIONS Executive Summary ES 1-7 1. PROJECT BACKGROUND AND INTRODUCTION 1-1 to 1-4 1.1 Project Background 1-1 1.2 Project Description 1-1 1.3 Approach and Methodology 1-3 2. SOCIO-ECONOMIC PROFILE OF THE PROJECT INFLUENCE ZONE 2-1 to 2-5 2.1 Introduction 2-1 2.2 Socio- Economic Status of Project influence District 2-1 2.2.1 Supaul District 2-1 2.2.2 Madhepura District 2-1 2.2.3 Saharsa District 2-2 2.3 Direct Impact Zone 2-2 2.4 Socio-Economic Profiling 2-3 2.5 Existing Public Amenities 2-4 2.5.1 Educational Service 2-4 2.5.2 Health CARE Service 2-4 2.5.3 Market Facility 2-4 2.5.4 Transport Facilities 2-4 3. ANALYSIS OF ALTERNATIVES & PROPOSED IMPROVEMENT 3-1 to 3-3 PLAN 3.1 Introduction 3-1 3.2 Design Considerations 3-1 3.3 Considerations of Alternatives 3-2 3.3.1 Proposed Realignments 3-2 Client : MoRT&H Up gradation of Birpur- Bihpur Section of NH 106 in the State of Bihar Social Impact Assessment & RAP 4.