Effective Prevention Without Side Effects: a Study of Male
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
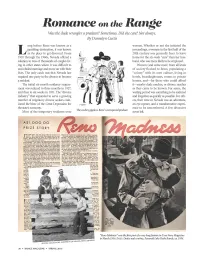
Romance on Tlw Range Was the Dude Wrangler a Predator? Sometimes
Romance on tlw Range Was the dude wrangler a predator? Sometimes. Did she care? Not always. By Donnelyn Curtis ong before Reno was known as a women. Whether or not she initiated the gambling destination, it was known proceedings, a woman in the first half of the L as the place to get divorced. From 20th century was generally freer to leave 1910 through the 1960s, Nevada offered a home for the six-week "cure" than her hus solution to tens of thousands of couples liv band, who was more likely to be employed. ing in other states where it was difficult to Women (and some men) from all levels end a failed marriage and move on with their of society flocked to Reno, populating a lives. The only catch was that Nevada law "colony" with its own culture, living in required one party in the divorce to become hotels, boardinghouses, rooms in private a resident. homes, and- for those who could afford The initial six-month residency require it- nearby dude ranches, or divorce ranches ment was reduced to three months in 1927, as they came to be known. For some, the and then to six weeks in 1931. The "divorce waiting period was something to be endured industry" that expanded to serve a growing and forgotten as quickly as possible. For oth number of migratory divorce seekers cush ers, their time in Nevada was an adventure, ioned the blow of the Great Depression for an eye-opener, and a transformative experi the state's economy. ence to be remembered. -

Romantic Realism
Romantic Realism http://www.thebookoflife.org/romantic-realism/ INTRODUCTION: We expect love to be the source of our greatest joys. But it is – of course – in practice, one of the most reliable routes to misery. Few forms of suffering are ever as intense as those we experience in relationships. Viewed from outside, love could be mistaken for a practice focused almost entirely on the generation of despair. We should, at least, try to understand our sorrows. Understanding does not magically remove problems, but it sets them in context, reduces our sense of isolation and persecution and helps us to accept that certain griefs are highly normal. The purpose of this essay is to help us develop an emotional skill we term Romantic Realism, defined as a correct awareness of what can legitimately be expected of love and the reasons why we will for large stretches of our lives be very disappointed by it, for no especially sinister or personal reasons. The problems begin because, despite all the statistics, we are inveterate optimists about how love should go. No amount of information seems able to shake us from our faith in love. A thousand divorces pass our doors; none seem relevant to us. We see relationship difficulties unfold around us all the time. But we retain a remarkable capacity to discount negative information. Despite the evidence of failures and loneliness, we cling to some highly ambitious background ideas of what relationships should be like – even if we have in reality never seen such unions in train anywhere near us. The ideal relationship is the equivalent of the snow leopard; our loyalty to it as a realistic possibility cannot be based on the evidence of our own experience. -

Received by the Supreme Court of California
Case No. _______________ IN THE SUPREME COURT OF THE STATE OF CALIFORNIA OLIVIA DE HAVILLAND, DBE, Plaintiff and Respondent, v. FX NETWORKS, LLC AND PACIFIC 2.1 ENTERTAINMENT GROUP, INC., Defendants and Appellants. After a Published Decision of the California Court of Appeal Second Appellate District, Division 3, Case No. B285629 Reversing a Ruling of the Los Angeles County Superior Court Case No. BC667011 The Honorable Holly E. Kendig, Dept. 42 PETITION FOR REVIEW Received by the Supreme Court of California HOWARTH & SMITH Don Howarth (SBN 53783) [email protected] *Suzelle M. Smith (SBN 113992) [email protected] Zoe E. Tremayne (SBN 310183) [email protected] 523 West Sixth Street, Suite 728 Los Angeles, CA 90014 Tel: (213) 955 – 9400 Fax: (213) 622 – 0791 Attorneys for Plaintiff and Respondent Olivia de Havilland, DBE 1 TABLE OF CONTENTS Page I. ISSUES PRESENTED .......................................................................... 9 II. THIS COURT SHOULD GRANT REVIEW ...................................... 9 III. BACKGROUND ................................................................................ 13 A. Factual Summary ......................................................................... 13 B. The Trial Court Ruling ................................................................. 17 C. The Appellate Opinion ................................................................. 26 IV. LEGAL ANALYSIS .......................................................................... 29 A. Anti-SLAPP Statute ................................................................ -

What Happens After the First Death Brad Wiewel (Austin, Texas)
CHAPTER 51 What Happens After the First Death BRAD WIEWEL (Austn, Texas) he loss of a spouse is often one of the most devastating experiences a person will encounter. Avoiding a Tcostly and uncertain future from that point forward involves proactively planning for that eventuality with a competent and concerned estate planning attorney. Getting from the graveside to a fulfilling life for the surviving spouse requires careful advance preparation. REMARRIAGE Perhaps the most overlooked aspect of “first death planning” is what happens if the survivor remarries. Nothing can bring more joy or more devastation than remarriage. The loss of a life-long spouse can be accompanied by depression, loneliness, and isolation. Men particularly seem vulnerable. No estate planning, a simple Will, accounts held in joint tenancy, or naming a new spouse as a beneficiary on life insurance and retirement assets can lead to a “Bimbo-Gigolo” problem. Because the surviving spouse has full control of this property if no prior planning is in place, he or she is perfectly capable of redirecting it to someone outside of your “family.” Experienced estate planning attorneys have heard numerous stories of wealth and heirlooms lost to a new husband or wife who seems to have little connection with the original family. One real life example involved an older couple who had accumulated a substantial estate. Mom died first, and the adult children arranged for a housekeeper to take care of dad. The housekeeper did an excellent job of taking care of dad, and soon enough dad and the housekeeper were getting married. A few weeks following their wedding they visited a lawyer to re-draft their Wills. -

Good of Marriage and the Morality of Sexual Relations John M
Notre Dame Law School NDLScholarship Journal Articles Publications 1997 Good of Marriage and the Morality of Sexual Relations John M. Finnis Notre Dame Law School, [email protected] Follow this and additional works at: https://scholarship.law.nd.edu/law_faculty_scholarship Part of the Family Law Commons, Jurisprudence Commons, and the Natural Law Commons Recommended Citation John M. Finnis, Good of Marriage and the Morality of Sexual Relations, 42 Am. J. Juris. 97 (1997). Available at: https://scholarship.law.nd.edu/law_faculty_scholarship/1092 This Article is brought to you for free and open access by the Publications at NDLScholarship. It has been accepted for inclusion in Journal Articles by an authorized administrator of NDLScholarship. For more information, please contact [email protected]. Forum: Sexual Morality and the Possibility of "Same-Sex Marriage" THE GOOD OF MARRIAGE AND THE MORALITY OF SEXUAL RELATIONS: SOME PHILOSOPHICAL AND HISTORICAL OBSERVATIONS JOHN FNNs Aquinas organized his account of the morality of sexual relations around the good of marriage. The good of marriage is one of the basic human goods to which human choice and action are directed by the first principles of practical reason.' Sex acts2 are immoral when they are I. ST I-II q. 94 a. 2c and Eth. V.12 n. 4 [1019] list the conjunctiomaris efeminae as a basic human good, and make it clear that here Aquinas has in mind the Roman law definition of marriage, which he quotes directly at the outset of his own early treatise on marriage, in IV Sent. d. 26 q. 1: "the mating of man with woman, which we call 'marriage.' {maris et feminae conjunctio, quam nos matrimonium appellamus). -

Older Women, Younger Men: Self and Stigma in Age-Discrepant Relationships Carol A
Clinical Sociology Review Volume 14 | Issue 1 Article 7 1-1-1996 Older Women, Younger Men: Self and Stigma in Age-Discrepant Relationships Carol A. B. Warren University of Kansas Follow this and additional works at: http://digitalcommons.wayne.edu/csr Recommended Citation Warren, Carol A. B. (1996) "Older Women, Younger Men: Self and Stigma in Age-Discrepant Relationships," Clinical Sociology Review: Vol. 14: Iss. 1, Article 7. Available at: http://digitalcommons.wayne.edu/csr/vol14/iss1/7 This Article is brought to you for free and open access by DigitalCommons@WayneState. It has been accepted for inclusion in Clinical Sociology Review by an authorized administrator of DigitalCommons@WayneState. Older Women, Younger Men: Self and Stigma in Age-Discrepant Relationships Carol A.B. Warren Department of Sociology University of Kansas Lawrence, KS 66045 ABSTRACT This study, based on intensive interviews with married, cohabiting and divorced older women and younger men, explores the impact of this type of age discrepancy on relationships and selves. Both the women and the men were aware of the stigmatizing potential of their relationships, in particular that the woman might be mistaken for the man's mother (which indeed sometimes happened). Although the couples' fear of audience response lessened over time, the im- pact of stigma on their sense of self remained. For the woman, her embodied self—body and face—was most problematic, and increas- ingly so as she aged. For the man, it was the cohort self: his lack of shared history with his wife, distance from his age peers, and pre- cipitation into other age-discrepant roles, such as grandfather. -

AFI PREVIEW Is Published by the Sat, Jul 9, 7:00; Wed, Jul 13, 7:00 to Pilfer the Family's Ersatz Van American Film Institute
ISSUE 77 AFI.com/Silver AFI SILVER THEATRE AND CULTURAL CENTER JULY 8–SEPTEMBER 14, 2016 44T H AFI LIFE ACHIEVEMENT AWARD HONOREE A FILM RESTROSPECTIVE THE COMPOSER B EHIND THE GREAT EST A MERICAN M OVIES O F OUR TIME PLUS GLORIOUS TECHNICOLOR ★ ’90S C INEMA N OW ★ JOHN C ARPENT E R LOONEY TUNES ★ KEN ADAM REMEMBERED ★ OLIVIA DE HAVILLAND CENTENNIAL Contents AFI Life Achievement Award: John Williams AFI Life Achievement Award: July 8–September 11 John Williams ......................................2 John Williams' storied career as the composer behind many of the greatest American films and television Keepin' It Real: '90s Cinema Now ................6 series of all time boasts hundreds of credits across seven decades. His early work in Hollywood included working as an orchestrator and studio pianist under such movie composer maestros as Bernard Herrmann, Ken Adam Remembered ..........................9 Alfred Newman, Henry Mancini, Elmer Bernstein and Franz Waxman. He went on to write music for Wim Wenders: Portraits Along the Road ....9 more than 200 television programs, including the groundbreaking anthology series ALCOA THEATRE Glorious Technicolor .............................10 and KRAFT TELEVISION THEATRE. Perhaps best known for his enduring collaboration with director Steven Spielberg, his scores are among the most iconic and recognizable in film history, from the edge-of-your- Special Engagements .................. 14, 16 seat JAWS (1975) motif to the emotional swell of E.T. THE EXTRA-TERRESTRIAL (1982) and the haunting UCLA Festival of Preservation ...............14 elegies of SCHINDLER'S LIST (1993). Always epic in scale, his music has helped define over half a century of the motion picture medium. -

Just a Gigolo Tab Chords and Lyrics by David Lee Roth
http://www.learn-classic-rock-songs.com Just A Gigolo Tab Chords And Lyrics By David Lee Roth Intro G-Am-D7-G-Am-D7 G Gmaj7 G6 Edim Am D7 Im just a gigolo, everywhere I go, people know the part I'm playing D G Paid for every dance, selling each romance, ooooh what they're saying F E7 There will come a day, youth will pass away Am Then what will they say about me Cm G E7 When the end comes I know they'll say just a gigolo Am D7 G Life goes on without me G Gmaj7 G6 Edim Am D7 Im just a gigolo, everywhere I go, people know the part I'm playing D G Paid for every dance, starting each romance, ooooh what they're saying F E7 There will come a day, youth will pass away Am Then what will they say about me Cm G E7 When the end comes I know they'll say just a gigolo Am D7 G Life goes on without me D7 G Gb F E Am D7 G 'Cause I aint got nobody, nobody cares for me nobody nobody cares for me Gb F E A7 I'm so sad and lonely sad and lonely sad and lonely D7sus Won't some sweet mama come and take a chance with me D7 Cause I aint so bad G C And Ill sing, sweet love songs, all of the time http://www.learn-classic-rock-songs.com http://www.learn-classic-rock-songs.com E7 She will only be, only, only be A7 D7 Bop bozadee bozadee bop zitty bop G Gb F E E7 Am D7 G I ain't got nobody, nobody cares for me, nobody, cares for me oh no Break- G-E7-Am-D7-G … G-Gb-F-E7-A7-Dsus-D7 …. -

Mistaking the CEO for a Gigolo Chapter 366-370
Mistaking the CEO for a Gigolo Chapter 366 “Are you trying to get me to leave?” A line appeared between Evan’s brows, and he was not happy about it. She just doesn’t want to talk to me, does she? Nicole shook her head and denied. “That’s not what I mean. I just don’t want to waste your precious time.” “Not at all. I don’t feel safe leaving Kyle and Juan here, so I’ll stay here for the night.” What? He plans to sleep here tonight? What does he mean by he doesn’t feel safe leaving Kyle and Juan here? He thinks I’ll abuse them? Since Evan had made it clear, she had no valid reason to kick him out. Moreover, he owned this house. But where is he going to sleep? “Well then. I’ll get Nina and Maya to sleep with me, and you’ll take their bedroom.” It was the same arrangement when he had a sleepover here quite some time ago. Evan thought about it and responded with a serious look, “Their beds are too small for an adult like me.” … Then what else do you want? An Alaskan king bed? If I gave you my bed, where am I going to sleep? She cleared her throat for a bit and plastered an awkward smile on her face, “It’s just one night, Mr. Seet. This is the best arrangement I can think of!” Instead of waiting for his reply, she immediately stood up and walked towards Nina’s and Maya’s room. -

Queer Kinship, Camp Aesthetics, and Juvenal's Ninth Satire
City University of New York (CUNY) CUNY Academic Works All Dissertations, Theses, and Capstone Projects Dissertations, Theses, and Capstone Projects 2010 Mensura Incognita: Queer Kinship, Camp Aesthetics, and Juvenal's Ninth Satire Michael Broder Graduate Center, City University of New York How does access to this work benefit ou?y Let us know! More information about this work at: https://academicworks.cuny.edu/gc_etds/1713 Discover additional works at: https://academicworks.cuny.edu This work is made publicly available by the City University of New York (CUNY). Contact: [email protected] MENSURA INCOGNITA QUEER KINSHIP, CAMP AESTHETICS, AND JUVENAL’S NINTH SATIRE by MICHAEL BRODER A dissertation submitted to the Graduate Faculty in Classics in partial fulfillment of the requirements for the degree of Doctor of Philosophy, The City University of New York 2010 ii © 2010 MICHAEL BRODER All Rights Reserved iii This manuscript has been read and accepted for the Graduate Faculty in Classics in satisfaction of the dissertation requirement for the degree of Doctor of Philosophy. Craig A. Williams Date Chair of Examining Committee Jennifer T. Roberts Date Acting Executive Officer Joel Allen Ronnie Ancona Craig A. Williams Supervision Committee THE CITY UNIVERSITY OF NEW YORK iv ABSTRACT MENSURA INCOGNITA QUEER KINSHIP, CAMP AESTHETICS, AND JUVENAL’S NINTH SATIRE by Michael Broder Adviser: Professor Craig Williams The dissertation addresses four problematic aspects of scholarship on Juvenal 9. The first two are matters of reception history: first, the poem has been understudied; and second, most major extant studies of the poem have been grossly or subtly homophobic. The other two problems are matters of literary criticism: Juvenal’s ninth satire has traditionally been read as an attack on homosexuality, when in fact it is neither an attack, nor is it about homosexuality. -

'I Don't Want to Be a Playa No More': an Exploration of the Denigrating Effects of 'Player' As a Stereotype Against Af
P a g e | 38 ‘I Don’t Want To be a Playa No More’: An Exploration of the Denigrating effects of ‘Player’ as a Stereotype Against African American Polyamorous Men Justin Leonard CLARDY Stanford University [email protected] Abstract: This paper shows how amatonormativity and its attendant social pressures converge at the intersections of race, gender, romantic relationality, and sexuality to generate peculiar challenges to polyamorous African American men in American society. Contrary to the view maintained in the “slut-vs-stud” phenomenon, I maintain that the label ‘player’ when applied to polyamorous African American men functions as a pernicious stereotype and has denigrating effects. Specifically, I argue that stereotyping polyamorous African American men as players estranges them from themselves and it constrains their agency by preemptively foreclosing the set of possibilities of what one’s sexual or romantic relational identities can be. Keywords: ethics, love, polyamory, stereotyping, race. “I don’t wanna be a playa no more” -Big Pun “In the case of black men, their subordination as a racial minority has more than canceled out their advantages as males in the larger society. Any understanding of their experience will have to come from an analysis of the complex problems they face as blacks and as men.” -Robert Staples Introduction This work is licensed under a Creative Commons Attribution 4.0 International License Analize© Justin – Journal Leonard of Gender Clardy and .Feminist ISSN 2344 Studies-2352 • New (Online). Series • -
Personality Profiles of Luxury Escorts: Psychoclinical Evidence in Prostitution Activity, Zimbabwe
vv ISSN: 2690-0815 DOI: https://dx.doi.org/10.17352/ijsrhc LIFE SCIENCES GROUP Received: 09 April, 2021 Research Article Accepted: 25 May, 2021 Published: 26 May, 2021 *Corresponding author: Dr. Giulio Perrotta, Personality profi les of luxury Psychologist sp.ing in Strategic Psychotherapy, Forensic Criminologist, Legal Advisor sp.ed SSPL, Researcher, Essayist, Institute for the study of escorts: Psychoclinical psychotherapies - ISP, Via San Martino della Battaglia no. 31, 00185, Rome, Italy, E-mail: evidence in prostitution Keywords: Escort; Luxury prostitution; Prostitution; MMPI-II; PICI-1; PSM-1 activity https://www.peertechzpublications.com Giulio Perrotta* Psychologist sp.ing in Strategic Psychotherapy, Forensic Criminologist, Legal Advisor sp.ed SSPL, Researcher, Essayist, Institute for the study of psychotherapies - ISP, Via San Martino della Battaglia no. 31, 00185, Rome, Italy Abstract Purpose: This research addresses the issue of the personality profi les of subjects who undertake the activity of luxury prostitution, understood as one or more acts aimed at offering sexual services in return for payment. In this research, the theme is aimed at the psychopathological investigation of the personalities, according to the PICI-1(TA), of all those subjects who voluntarily and without any constriction or obligation, freely decide to undertake this activity, for personal reasons. Methods: Clinical interview and administration of the MMPI-II, PICI-1 and PSM-1. Results: The research on a population sample of 838 persons showed that: 1) On the MMPI-II they reported pathological values on the scales of hypochondria, paranoia, depression, psychopathic deviance, hysteria, schizophrenia and hypomania; on the content scales, on the other hand, the scales of anxiety, depression, antisocial behaviour, social distress, anger, cynicism and family problems were pathological.