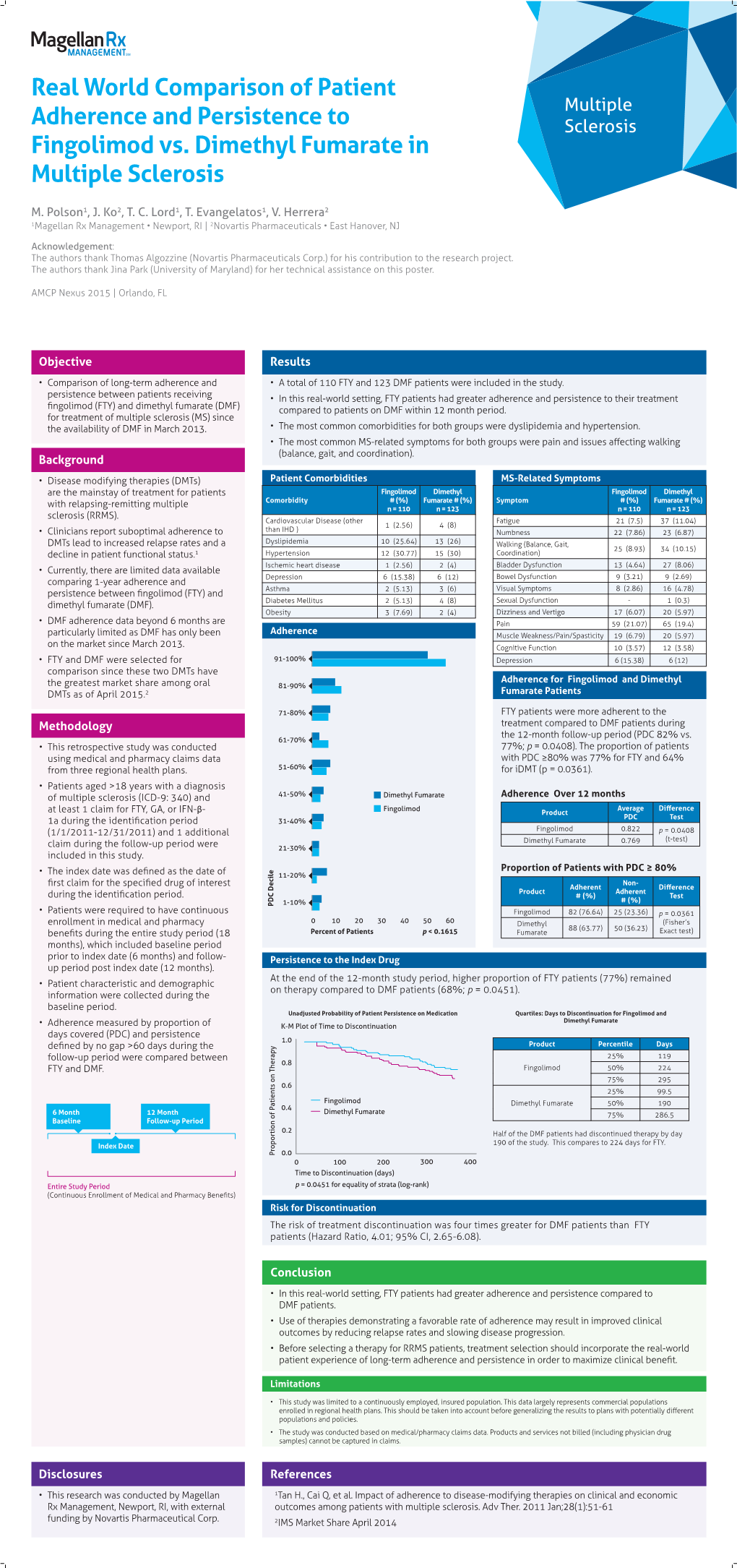
Real World Comparison of Patient Multiple Adherence and Persistence to Sclerosis Fingolimod Vs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Change of Fingolimod Patient Profiles Over Time
Journal of Personalized Medicine Article The Change of Fingolimod Patient Profiles over Time: A Descriptive Analysis of Two Non-Interventional Studies PANGAEA and PANGAEA 2.0 Tjalf Ziemssen 1,* and Ulf Schulze-Topphoff 2 1 Zentrum für Klinische Neurowissenschaften, Universitätsklinikum Carl Gustav Carus, D-01307 Dresden, Germany 2 Novartis Pharma GmbH, D-90429 Nuremberg, Germany; [email protected] * Correspondence: [email protected] Abstract: (1) Background: Fingolimod (Gilenya®) was the first oral treatment for patients with relapsing-remitting multiple sclerosis (RRMS). Since its approval, the treatment landscape has changed enormously. (2) Methods: Data of PANGAEA and PANGAEA 2.0, two German real-world studies, were descriptively analysed for possible evolution of patient profiles and treatment behavior. Both are prospective, multi-center, non-interventional, long-term studies on fingolimod use in RRMS in real life. Data of 4229 PANGAEA patients (recruited 2011–2013) and 2441 PANGAEA 2.0 patients (recruited 2015–2018) were available. Baseline data included demographics, RRMS characteristics and disease severity. (3) Results: The mean age of PANGAEA and PANGAEA 2.0 patients was similar (38.8 vs. 39.2 years). Patients in PANGAEA 2.0 had shorter disease duration (7.1 vs. 8.2 years) and fewer relapses in the year before baseline (1.2 vs. 1.6). Disease severity at baseline estimated by Citation: Ziemssen, T.; EDSS and SDMT was lower in PANGAEA 2.0 patients compared to PANGAEA (EDSS difference Schulze-Topphoff, U. The Change of 1.0 points; SDMT difference 3.3 points). (4) Conclusions: The results hint at an influence of changes in Fingolimod Patient Profiles over the treatment guidelines and the label on fingolimod patients profiles over time. -

Medical Review(S) Clinical Review
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 22-527 MEDICAL REVIEW(S) CLINICAL REVIEW Application Type NDA Application Number 22-527 Priority or Standard P Submit Date 12-21-2009 Received Date 12-21-2009 PDUFA Goal Date 9-21-2010 Division / Office FDA/ODE1 Reviewer Name Heather D. Fitter Review Completion Date August 26, 2010 Established Name Fingolimod (Proposed) Trade Name Gilenya Therapeutic Class S1P receptor modulator Applicant Novartis Formulation(s) Oral tablets Dosing Regimen 0.5 mg Indication(s) To reduce the frequency of relapses and delay the progression of disability in relapsing MS Intended Population(s) Relapsing Multiple Sclerosis Template Version: March 6, 2009 Clinical Review Heather D. Fitter, M.D. NDA 22-527 Fingolimod Table of Contents 1 RECOMMENDATIONS/RISK BENEFIT ASSESSMENT......................................... 7 1.1 Recommendation on Regulatory Action ............................................................. 7 1.2 Risk Benefit Assessment.................................................................................... 8 2 INTRODUCTION AND REGULATORY BACKGROUND ........................................ 8 2.1 Product Information ............................................................................................ 9 2.2 Table of Currently Available Treatments for the Proposed Indication................. 9 2.3 Availability of Proposed Active Ingredient in the United States ........................ 12 2.4 Important Safety Issues with Consideration to Related Drugs......................... -

Analysis of Changes in Disease Modifying Treatment in The
Abstract number 4CPS-109 ATC code: L04 - Immunosuppressive agents ANALYSIS OF CHANGES IN DISEASE MODIFYING TREATMENT IN THE MANAGEMENT OF PATIENTS WITH MULTIPLE SCLEROSIS Arancón Pardo A1, Sobrino Jiménez C1, Rodríguez Martín E1, Bilbao Gómez-Martino C1, Villamañán Bueno E1, Jiménez-Nácher I1, Moreno Ramos F1, González Fernández A1, Moreno Palomino M1, García-Trevijano M1, Herrero Ambrosio A1 1Hospital Universitario La Paz, Pharmacy Department, Madrid, Spain. BACKGROUND AND IMPORTANCE •Currently, several disease modifying drugs are approved for multiple sclerosis (MS). IFNβ-1b, IFNβ-1a, pegIFNβ-1a, glatiramer acetate, teriflunomide and dimethylfumarate are indicated for first-line therapy. Second-line treatment includes natalizumab, fingolimod, alemtuzumab, cladribine and ocrelizumab. When disease progresses, modifications between first-line drugs or switch to a second-line drug are proposed. It is essential to know their efficacy and security profiles, in order to decide which is the best option for each patient. AIM AND OBJECTIVES •To assess the reasons for changes in disease modifying drugs in MS patients in routine clinical practice. MATERIAL AND METHODS •We included patients with MS who changed their treatment between 23rd May 2018 and 26th March 2019. •The collected data were: Disease modifying drugs Reasons for treatment Duration of initial therapy before and after the modification modification RESULTS •42 patients had any treatment modification during the study period. •26 (62%) were women and mean age was 47 years (SD 9.3). •Median duration of previous treatment was 44 months (3-282). •Previous treatment was a first-line drug in 34 patients (81%) and modified treatment was a first-line drug in 24 (57%). -

Patient Focused Disease State and Assistance Programs
Patient Focused Disease State and Assistance Programs Medication Medication Toll-free Brand (Generic) Website number Additional Resources Allergy/Asthma Xolair (omalizumab) xolair.com 1-866-4-XOLAIR lung.org Cardiovascular Pradaxa (dabigatran) pradaxa.com 877-481-5332 heart.org Praluent (alirocumab) praluent.com 844-PRALUENT thefhfoundation.org Repatha (evolocumab) repatha.com 844-REPATHA Tikosyn (dofetilide) tikosyn.com 800-879-3477 Crohn’s Disease Cimzia (certolizumab pegol) cimzia.com 866-4-CIMZIA crohnsandcolitis.com Humira (adalimumab) humira.com 800-4-HUMIRA crohnsforum.com Stelara (ustekinumab) stelarainfo.com 877-STELARA Dermatology Cosentyx (secukinumab) cosentyx.com 844-COSENTYX psoriasis.org Dupixent (dupilumab) dupixent.com 844-DUPIXENT nationaleczema.org Enbrel (etanercept) enbrel.com 888-4-ENBREL Humira (adalimumab) humira.com 800-4-HUMIRA Otezla (apremilast) otezla.com 844-4-OTEZLA Stelara (ustekinumab) stelarainfo.com 877-STELARA Taltz (ixekizumab) taltz.com 800-545-5979 Hematology Aranesp (darbepoetin alfa) aranesp.com 805-447-1000 chemocare.com Granix (filgrastim) granixrx.com 888-4-TEVARX hematology.org Jadenu (deferasirox) jadenu.com 888-282-7630 Neulasta (pegfilgrastim) neulasta.com 800-77-AMGEN Neupogen (filgrastim) neupogen.com 800-77-AMGEN Nivestym (filgrastim) nivestym.com 800-879-3477 Zarxio (filgrastim) zarxio.com 800-525-8747 Zytiga (abiraterone) zytiga.com 800-JANSSEN Hepatitis B Baraclude (entecavir) baraclude.com 800-321-1335 cdc.gov Viread (tenofovir disoproxil viread.com 800-GILEAD-5 hepb.org fumarate) -

Dimethyl Fumarate Or Any of the Excipients of TECFIDERA Safely and Effectively
HIGHLIGHTS OF PRESCRIBING INFORMATION ___________________ CONTRAINDICATIONS ___________________ These highlights do not include all the information needed to use Known hypersensitivity to dimethyl fumarate or any of the excipients of TECFIDERA safely and effectively. See full prescribing information for TECFIDERA. (4) TECFIDERA. _______________ _______________ WARNINGS AND PRECAUTIONS TECFIDERA® (dimethyl fumarate) delayed-release capsules, for oral use • Anaphylaxis and angioedema: Discontinue and do not restart TECFIDERA Initial U.S. Approval: 2013 if these occur. (5.1) • Progressive multifocal leukoencephalopathy (PML): Withhold _________________ RECENT MAJOR CHANGES _________________ TECFIDERA at the first sign or symptom suggestive of PML. (5.2) Dosage and Administration, Blood Test Prior to • Lymphopenia: Obtain a CBC including lymphocyte count before initiating TECFIDERA, after 6 months, and every 6 to 12 months thereafter. Initiation of Therapy (2.2) 1/2017 9 Warnings and Precautions, PML (5.2) 2/2016 Consider interruption of TECFIDERA if lymphocyte counts <0.5 x 10 /L Warnings and Precautions, Liver Injury (5.4) 1/2017 persist for more than six months. (5.3) • Liver injury: Obtain serum aminotransferase, alkaline phosphatase, and total bilirubin levels before initiating TECFIDERA and during treatment, __________________ INDICATIONS AND USAGE _________________ as clinically indicated. Discontinue TECFIDERA if clinically significant TECFIDERA is indicated for the treatment of patients with relapsing forms of liver injury induced by TECFIDERA is suspected. (5.4) multiple sclerosis (1) _______________ DOSAGE AND ADMINISTRATION ______________ ___________________ ADVERSE REACTIONS ___________________ • Starting dose: 120 mg twice a day, orally, for 7 days (2.1) Most common adverse reactions (incidence ≥10% and ≥2% placebo) were • Maintenance dose after 7 days: 240 mg twice a day, orally (2.1) flushing, abdominal pain, diarrhea, and nausea. -

COMPARISON of the WHO ATC CLASSIFICATION & Ephmra/Intellus Worldwide ANATOMICAL CLASSIFICATION
COMPARISON OF THE WHO ATC CLASSIFICATION & EphMRA/Intellus Worldwide ANATOMICAL CLASSIFICATION: VERSION June 2019 2 Comparison of the WHO ATC Classification and EphMRA / Intellus Worldwide Anatomical Classification The following booklet is designed to improve the understanding of the two classification systems. The development of the two systems had previously taken place separately. EphMRA and WHO are now working together to ensure that there is a convergence of the 2 systems rather than a divergence. In order to better understand the two classification systems, we should pay attention to the way in which substances/products are classified. WHO mainly classifies substances according to the therapeutic or pharmaceutical aspects and in one class only (particular formulations or strengths can be given separate codes, e.g. clonidine in C02A as antihypertensive agent, N02C as anti-migraine product and S01E as ophthalmic product). EphMRA classifies products, mainly according to their indications and use. Therefore, it is possible to find the same compound in several classes, depending on the product, e.g., NAPROXEN tablets can be classified in M1A (antirheumatic), N2B (analgesic) and G2C if indicated for gynaecological conditions only. The purposes of classification are also different: The main purpose of the WHO classification is for international drug utilisation research and for adverse drug reaction monitoring. This classification is recommended by the WHO for use in international drug utilisation research. The EphMRA/Intellus Worldwide classification has a primary objective to satisfy the marketing needs of the pharmaceutical companies. Therefore, a direct comparison is sometimes difficult due to the different nature and purpose of the two systems. -

Hpra Drug Safety 66Th Newsletter Edition
FEBRUARY 2015 HPRA DRUG SAFETY 66TH NEWSLETTER EDITION 3 Mycophenolate mofetil (CellCept) and 4 Direct Healthcare Professional In this Edition Mycophenolic acid (Myfortic) - New warnings Communications published on about the risks of hypogammaglobulinaemia the HPRA website since the last 1 Eligard (leuprorelin acetate depot injection) and bronchiectasis Drug Safety Newsletter - Risk of lack of efficacy due to incorrect reconstitution and administration process 4 Tecfidera (dimethyl fumarate) - Progressive Multifocal Leukoencephalopathy (PML) has 2 Beta interferons – Risk of thrombotic occurred in a patient with severe microangiopathy and nephrotic syndrome and prolonged lymphopenia Eligard (leuprorelin acetate depot injection) - Risk of lack of efficacy due to incorrect reconstitution and administration process Following identification of a signal and safe treatment of patients with It is available in six-monthly (45mg), of administration errors with Eligard prostate cancer. Lack of efficacy may three-monthly (22.5mg) and one- and concerns that such errors may occur due to incorrect reconstitution monthly (7.5mg) formulations. In impact on clinical efficacy, this issue of Eligard. the majority of patients, androgen was reviewed at EU level by the deprivation therapy (ADT) with Eligard Eligard is indicated for the treatment Pharmacovigilance Risk Assessment results in testosterone levels below the of hormone dependent advanced Committee (PRAC). A cumulative standard castration threshold (<50ng/ prostate cancer and for the treatment review of reported global cases dL; <1.7 nmol/L); and in most cases, of high risk localised and locally identified errors related to storage, patients reach testosterone levels advanced hormone dependent preparation and reconstitution of below <20ng/dL. prostate cancer in combination Eligard. -

The Real-World Patient Experience of Fingolimod and Dimethyl Fumarate
Wicks et al. BMC Res Notes (2016) 9:434 DOI 10.1186/s13104-016-2243-8 BMC Research Notes RESEARCH ARTICLE Open Access The real‑world patient experience of fingolimod and dimethyl fumarate for multiple sclerosis Paul Wicks1* , Lawrence Rasouliyan2, Bo Katic1, Beenish Nafees3, Emuella Flood3 and Rahul Sasané4 Abstract Background: Oral disease-modifying therapies offer equivalent or superior efficacy and greater convenience versus injectable options. Objectives: To compare patient-reported experiences of fingolimod and dimethyl fumarate. Methods: Adult relapsing-remitting multiple sclerosis patients treated with fingolimod or dimethyl fumarate were recruited from an online patient community and completed an online survey about treatment side effects, discon- tinuation, and satisfaction. Results: 281 patients in four groups completed the survey: currently receiving fingolimod (CF, N 61), currently receiving dimethyl fumarate (CDMF, N 129), discontinued fingolimod (DF, N 32) and discontinued= dimethyl fuma- rate (DDMF, N 59). Reasons for treatment= switch were to take oral treatment =(CF: 63.3 %, CDMF: 61.8 %), side effects of prior medication= (CF: 67.3 %, CDMF: 44.1 %) and lack of effectiveness of prior medication (CF: 38.8 %, CDMF: 31.4 %). Main reasons for discontinuation were side effects (DF: 46.9 %, DDMF: 67.8 %) and lack of effectiveness (DF: 25.0 %, DDMF: 15.3 %). CDMF patients had an increased risk of abdominal pain, flushing, diarrhea, and nausea. Treatment satisfaction was highest among CF patients followed by CDMF, DF, and then DDMF patients. Conclusions: Discontinuation was driven by experience of side effects. Patients currently taking dimethyl fumarate were more likely to experience a side effect versus patients currently taking fingolimod. -

Fingolimod (Gilenya)
Fingolimod (Gilenya) This factsheet is about fingolimod, a Whether you’ll be offered this or any other DMT disease modifying therapy (DMT) for depends on whether you qualify for it based relapsing multiple sclerosis (MS). on guidelines used by your neurologist. These come from NICE and the Association of British At the end of this factsheet you’ll find out where Neurologists and are based on a drug’s Europe- you can get more information on this drug, other wide licence. drugs for MS and the benefits of early treatment. In England there are also rules from NHS England about who can have the different DMTs and when. This factsheet doesn’t cover everything about Scotland, Wales and Northern Ireland also have this drug and shouldn’t be used in place of their own guidelines for many DMTs. advice from your MS specialist team. For more information speak to them and read the online information from the drug’s makers (see the Whether you can have a drug also depends on section More information and support). if the NHS where you live will pay for it. NHS England guidelines on this tend to follow what What is fingolimod? NICE says. Fingolimod is a drug that was first given a licence These people can have fingolimod: to be used against relapsing MS in the UK in 2011. In England and Northern Ireland: In 2012 the National Institute for Health and Care Excellence (NICE) gave the go ahead for it to be • People with ‘highly active relapsing remitting used on the NHS. -

Dimethyl Fumarate and Progressive Multifocal Leucoencephalopathy (PML)
Dimethyl fumarate and progressive multifocal leucoencephalopathy (PML) Introduction Dimethyl fumarate Psorinovo® is not registered through the Medicines Evaluation Board (MEB). It is a compounded drug made by GMP compounding pharmacy Mierlo Hout in the Netherlands, and used for the indication psoriasis [1]. Psorinovo® has been compounded by pharmacy Mierlo Hout for 28 years. According to Dutch law Mierlo Hout pharmacy is regarded as a supplying-pharmacy. ® Dimethyl fumarate, registered as Tecfidera , was granted marketing authorization in the Netherlands on 30 January 2014 and is indicated for the treatment of adult patients with relapsing remitting multiple sclerosis [2]. Progressive multifocal leukoencephalopathy (PML) is a severe demyelinating disease of the central nervous system caused by reactivation of the polyomavirus JC (JC virus). Asymptomatic primary infection with the JC virus occurs in childhood, antibodies can be found in 86% of adults. PML occurs almost exclusively in immunosuppressed individuals. There were only isolated cases reported of PML in patients without apparent immunosuppression. However, there are reports of PML affecting patients who have conditions associated with minimal or occult immunosuppression, such as hepatic cirrhosis and renal failure [3]. PML has also been reported in patients treated with drugs such as belatacept, brentuximab, efalizumab, fludarabine, glucocorticoids, infliximab, mycophenolate, rituximab, ruxolitinib and natalizumab. In some cases, these drugs were used in combination with other immunosuppressive medications (eg, cyclophosphamide, leflunomide, methotrexate). Many of the patients had an underlying hematologic malignancy or collagen vascular disease [3]. There is no specific treatment for PML. The main approach is restoring the host adaptive immune response, a strategy that appears to prolong survival. -
CIRCULAR 73 of 2015: Entry and Verification (E&V) Criteria for Identifying Beneficiaries with Risk Factors in Medical Scheme
CIRCULAR Reference: E&V version 9.1 Contact person: Carrie-Anne Cairncross Tel: 012 431 0412 Fax: 086 687 3979 E-mail: [email protected] Date: 11 December 2015 CIRCULAR 73 OF 2015: Entry and verification (E&V) criteria for identifying beneficiaries with risk factors in medical schemes The Council for Medical schemes (CMS) has published the guidelines for identifying medical scheme beneficiaries with risk factors in accordance with the entry and verification criteria. (http://www.medicalschemes.com/files/ITAP%20Documents/Vers9_1OfEVGdlns20151211.pdf) It is important that medical schemes and administrators take note of the updated version 9.1 and implement all the changes made in the guideline before they extract the data for the 2015 submission. The changes are listed below. 1. Parts 3 and 4, which relate to preparation and submission of data has been amended to reflect the submission of Scheme Risk Measurement (SRM) data via the Healthcare Utilisation Annual Statutory Returns (ASR) System. 2. Changes to clinical entry end verification criteria: 2.1. The provider type was changed from any registered medical practitioner to specialist ophthalmologist (Table 17) 2.2. Glaucoma was added to the list of conditions that need specialist diagnosis as stated in paragraph 5.17 2.3. Rheumatoid Arthritis was removed from paragraph 5.17 2.4. The note on the Rheumatoid Arthritis table i.e. “Where a patient is not using disease modifying anti-rheumatic medicines, the diagnosis must be verified by a specialist physician or rheumatologist” has been updated to state “Where a patient is using disease modifying anti-rheumatic medicines, the diagnosis must be verified by a specialist physician or rheumatologist.” 2.5. -

Patent No.: US 8952006 B2
USOO8952006B2 (12) United States Patent (10) Patent No.: US 8,952,006 B2 Cundy et al. (45) Date of Patent: *Feb. 10, 2015 (54) MORPHOLINOALKYL FUMARATE FOREIGN PATENT DOCUMENTS COMPOUNDS, PHARMACEUTICAL COMPOSITIONS, AND METHODS OF USE W. wo.5: 886 WO WO O2/O55063 T 2002 (71) Applicant: XenoPort, Inc., Santa Clara, CA (US) WO WO O2/O55066 T 2002 WO WOO3,087.174 10, 2003 (72) Inventors: Kenneth C. Cundy, Redwood City, CA WO WO 2005/023241 3, 2005 WO WO 2005/027899 3, 2005 (US); Suresh K. Manthati, Sunnyvale, WO WO 2006/037342 4/2006 CA (US); David J. Wustrow, Los Gatos, WO WO 2006/122652 11, 2006 CA (US) WO WO 2007/042034 4/2007 WO 2010/022177 A2 2, 2010 (73) Assignee: XenoPort, Inc., Santa Clara, CA (US) WO 2014/0964.25 A2 6, 2014 (*) Notice: Subject to any disclaimer, the term of this OTHER PUBLICATIONS patent is extended or adjusted under 35 U.S.C. 154(b) by 0 days. Cecil Textbook of Medicine, 20th edition (1996), vol. 2, pp. 2050 2057.* spent is Subject to a terminal dis- Cecil Textbook of Medicine, 20th edition (1996), vol. 2, pp. 1992 1996.* (21) Appl. No.: 13/761,864 Ey's statisfy it to (22) Filed: Feb. 7, 2013 com/2003/HEALTH/conditions/09/24/alzheimers.drug.ap/index. e f 9 html>. (65) Prior Publication Data Atreya et al., NF-kB in inflammatory bowel disease, J Intern Med (2008), 263(6): 591-6. US 2013/02O3753 A1 Aug. 8, 2013 Bardgett et al., NMDA receptor blockade and hippocampal neuronal loss impair fear conditioning and position habit reversal in C57B1/6 mice, Brain Res Bull (2003), 60: 131-142.