Chapter 1: the Fanconi Anemia DNA Repair Pathway
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Structure and Function of the Human Recq DNA Helicases
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2005 Structure and function of the human RecQ DNA helicases Garcia, P L Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: https://doi.org/10.5167/uzh-34420 Dissertation Published Version Originally published at: Garcia, P L. Structure and function of the human RecQ DNA helicases. 2005, University of Zurich, Faculty of Science. Structure and Function of the Human RecQ DNA Helicases Dissertation zur Erlangung der naturwissenschaftlichen Doktorw¨urde (Dr. sc. nat.) vorgelegt der Mathematisch-naturwissenschaftlichen Fakultat¨ der Universitat¨ Z ¨urich von Patrick L. Garcia aus Unterseen BE Promotionskomitee Prof. Dr. Josef Jiricny (Vorsitz) Prof. Dr. Ulrich H ¨ubscher Dr. Pavel Janscak (Leitung der Dissertation) Z ¨urich, 2005 For my parents ii Summary The RecQ DNA helicases are highly conserved from bacteria to man and are required for the maintenance of genomic stability. All unicellular organisms contain a single RecQ helicase, whereas the number of RecQ homologues in higher organisms can vary. Mu- tations in the genes encoding three of the five human members of the RecQ family give rise to autosomal recessive disorders called Bloom syndrome, Werner syndrome and Rothmund-Thomson syndrome. These diseases manifest commonly with genomic in- stability and a high predisposition to cancer. However, the genetic alterations vary as well as the types of tumours in these syndromes. Furthermore, distinct clinical features are observed, like short stature and immunodeficiency in Bloom syndrome patients or premature ageing in Werner Syndrome patients. Also, the biochemical features of the human RecQ-like DNA helicases are diverse, pointing to different roles in the mainte- nance of genomic stability. -

What Is Fanconi Anemia and How Is It Diagnosed
Fanconi anemia and its diagnosis: Fanconi anemia (FA), named for the Swiss pediatrician Guido Fanconi, is an inherited disorder that can lead to bone marrow failure (aplastic anemia), leukemia and/or solid tumors, with oral and gynecologic tumors being the most common. FA is almost exclusively a recessive disorder: if both parents carry a defect (mutation) in the same FA gene, each of their children has a 25% chance of inheriting the defective gene from both parents. When this happens, the child will have FA. While the total number of FA patients is not documented worldwide, scientists estimate that the carrier frequency (carriers are people carrying a defect in one copy of a particular FA gene, whose other copy of that same FA gene is normal) for FA in the U.S. is 1 in 181. The incidence rate, or the likelihood of a child being born with FA, is about 1 in 131,000 in the U.S., with approximately 31 babies born with FA each year. Scientists have now discovered 19 FA genes [FANCA, -B, -C, -D1 (also known as BRCA2), D2, E, F, G, I, J, L, M, N, O, P, Q, RAD51, BRCA1, and T]. Mutations in these genes account for more than 95% of reported Fanconi anemia cases. Mutations in FANCA, FANCC and FANCG are the most common and account for approximately 85% of FA patients worldwide. FANCD1, FANCD2, FANCE, FANCF and FANCL account for 10%, while the remaining FA genes, FANCB, FANCI, FANCJ, FANCM, FANCN, FANCO, FANCP, and FANCQ represent less than 5%. Some individuals with FA do not appear to have mutations in these 19 genes, so we anticipate that additional FA genes will be discovered in the future. -

Regulation of DNA Cross-Link Repair by the Fanconi Anemia/BRCA Pathway
Downloaded from genesdev.cshlp.org on September 29, 2021 - Published by Cold Spring Harbor Laboratory Press REVIEW Regulation of DNA cross-link repair by the Fanconi anemia/BRCA pathway Hyungjin Kim and Alan D. D’Andrea1 Department of Radiation Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts 02215, USA The maintenance of genome stability is critical for sur- and quadradials, a phenotype widely used as a diagnostic vival, and its failure is often associated with tumorigen- test for FA. esis. The Fanconi anemia (FA) pathway is essential for At least 15 FA gene products constitute a common the repair of DNA interstrand cross-links (ICLs), and a DNA repair pathway, the FA pathway, which resolves germline defect in the pathway results in FA, a cancer ICLs encountered during replication (Fig. 1A). Specifi- predisposition syndrome driven by genome instability. cally, eight FA proteins (FANCA/B/C/E/F/G/L/M) form Central to this pathway is the monoubiquitination of a multisubunit ubiquitin E3 ligase complex, the FA core FANCD2, which coordinates multiple DNA repair activ- complex, which activates the monoubiquitination of ities required for the resolution of ICLs. Recent studies FANCD2 and FANCI after genotoxic stress or in S phase have demonstrated how the FA pathway coordinates three (Wang 2007). The FANCM subunit initiates the pathway critical DNA repair processes, including nucleolytic in- (Fig. 1B). It forms a heterodimeric complex with FAAP24 cision, translesion DNA synthesis (TLS), and homologous (FA-associated protein 24 kDa), and the complex resem- recombination (HR). Here, we review recent advances in bles an XPF–ERCC1 structure-specific endonuclease pair our understanding of the downstream ICL repair steps (Ciccia et al. -

Open Full Page
CCR PEDIATRIC ONCOLOGY SERIES CCR Pediatric Oncology Series Recommendations for Childhood Cancer Screening and Surveillance in DNA Repair Disorders Michael F. Walsh1, Vivian Y. Chang2, Wendy K. Kohlmann3, Hamish S. Scott4, Christopher Cunniff5, Franck Bourdeaut6, Jan J. Molenaar7, Christopher C. Porter8, John T. Sandlund9, Sharon E. Plon10, Lisa L. Wang10, and Sharon A. Savage11 Abstract DNA repair syndromes are heterogeneous disorders caused by around the world to discuss and develop cancer surveillance pathogenic variants in genes encoding proteins key in DNA guidelines for children with cancer-prone disorders. Herein, replication and/or the cellular response to DNA damage. The we focus on the more common of the rare DNA repair dis- majority of these syndromes are inherited in an autosomal- orders: ataxia telangiectasia, Bloom syndrome, Fanconi ane- recessive manner, but autosomal-dominant and X-linked reces- mia, dyskeratosis congenita, Nijmegen breakage syndrome, sive disorders also exist. The clinical features of patients with DNA Rothmund–Thomson syndrome, and Xeroderma pigmento- repair syndromes are highly varied and dependent on the under- sum. Dedicated syndrome registries and a combination of lying genetic cause. Notably, all patients have elevated risks of basic science and clinical research have led to important in- syndrome-associated cancers, and many of these cancers present sights into the underlying biology of these disorders. Given the in childhood. Although it is clear that the risk of cancer is rarity of these disorders, it is recommended that centralized increased, there are limited data defining the true incidence of centers of excellence be involved directly or through consulta- cancer and almost no evidence-based approaches to cancer tion in caring for patients with heritable DNA repair syn- surveillance in patients with DNA repair disorders. -

Gene Section Review
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL INIST-CNRS Gene Section Review XRCC2 (X-ray repair cross complementing 2) Paul R Andreassen, Helmut Hanenberg Division of Experimental Hematology and Cancer Biology, Cancer and Blood Diseases Institute, Cincinnati Children's Hospital Medical Center, Cincinnati OH, USA; [email protected] (PRA); Department of Pediatrics III, University Children's Hospital Essen, University Duisburg- Essen, Essen Germany; [email protected] (HH) Published in Atlas Database: November 2017 Online updated version : http://AtlasGeneticsOncology.org/Genes/XRCC2ID334ch7q36.html Printable original version : http://documents.irevues.inist.fr/bitstream/handle/2042/69759/11-2017-XRCC2ID334ch7q36.pdf DOI: 10.4267/2042/69759 This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2019 Atlas of Genetics and Cytogenetics in Oncology and Haematology Clinically, the only known FA-U patient in the Abstract world exhibits severe congenital abnormalities, but XRCC2 is one of five somatic RAD51 paralogs, all had not developed, by seven years of age, the bone of which have Walker A and B ATPase motifs. marrow failure and cancer that are often seen in Each of the paralogs, including XRCC2, has a patients from other FA complementation groups. function in DNA double-strand break repair by Keywords homologous recombination (HR). However, their Fanconi anemia, Breast Cancer Susceptibility, individual roles are not as well understood as that Tumor Suppressor, Homologous Recombination, of RAD51 itself. DNA Repair, RAD51 Paralog The XRCC2 protein forms a complex (BCDX2) with three other RAD51 paralogs, RAD51B, RAD51C and RAD51D. It is believed that the Identity BCDX2 complex mediates HR downstream of Other names: FANCU BRCA2 but upstream of RAD51, as XRCC2 is HGNC (Hugo): XRCC2 involved in the assembly of RAD51 into DNA damage foci. -
Genomic Profiling Reveals High Frequency of DNA Repair Genetic
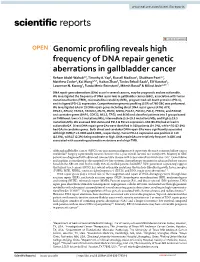
www.nature.com/scientificreports OPEN Genomic profling reveals high frequency of DNA repair genetic aberrations in gallbladder cancer Reham Abdel‑Wahab1,9, Timothy A. Yap2, Russell Madison4, Shubham Pant1,2, Matthew Cooke4, Kai Wang4,5,7, Haitao Zhao8, Tanios Bekaii‑Saab6, Elif Karatas1, Lawrence N. Kwong3, Funda Meric‑Bernstam2, Mitesh Borad6 & Milind Javle1,10* DNA repair gene aberrations (GAs) occur in several cancers, may be prognostic and are actionable. We investigated the frequency of DNA repair GAs in gallbladder cancer (GBC), association with tumor mutational burden (TMB), microsatellite instability (MSI), programmed cell death protein 1 (PD‑1), and its ligand (PD‑L1) expression. Comprehensive genomic profling (CGP) of 760 GBC was performed. We investigated GAs in 19 DNA repair genes including direct DNA repair genes (ATM, ATR , BRCA1, BRCA2, FANCA, FANCD2, MLH1, MSH2, MSH6, PALB2, POLD1, POLE, PRKDC, and RAD50) and caretaker genes (BAP1, CDK12, MLL3, TP53, and BLM) and classifed patients into 3 groups based on TMB level: low (< 5.5 mutations/Mb), intermediate (5.5–19.5 mutations/Mb), and high (≥ 19.5 mutations/Mb). We assessed MSI status and PD‑1 & PD‑L1 expression. 658 (86.6%) had at least 1 actionable GA. Direct DNA repair gene GAs were identifed in 109 patients (14.2%), while 476 (62.6%) had GAs in caretaker genes. Both direct and caretaker DNA repair GAs were signifcantly associated with high TMB (P = 0.0005 and 0.0001, respectively). Tumor PD‑L1 expression was positive in 119 (15.6%), with 17 (2.2%) being moderate or high. DNA repair GAs are relatively frequent in GBC and associated with coexisting actionable mutations and a high TMB. -

Understanding the Role of Rad52 in Homologous Recombination for Therapeutic Advancement
Author Manuscript Published OnlineFirst on October 15, 2012; DOI: 10.1158/1078-0432.CCR-11-3150 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. The Role of Rad52 in Homologous Recombination MOLECULAR PATHWAYS: Understanding the role of Rad52 in homologous recombination for therapeutic advancement Benjamin H. Lok 1,2 and Simon N. Powell 1 1 Memorial Sloan-Kettering Cancer Center, New York, NY 2 New York University School of Medicine, New York, NY Corresponding author: Simon N. Powell, MD PhD Department of Radiation Oncology, Memorial Sloan-Kettering Cancer Center, New York, NY Mailing address: 1250 1st Avenue, Box 33, New York, NY 10065 Telephone: 212-639-6072 Facsimile: 212-794-3188 E-mail: [email protected] Conflicts of interest. The authors have no potential conflict of interest to report. 1 Downloaded from clincancerres.aacrjournals.org on September 26, 2021. © 2012 American Association for Cancer Research. Author Manuscript Published OnlineFirst on October 15, 2012; DOI: 10.1158/1078-0432.CCR-11-3150 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. The Role of Rad52 in Homologous Recombination Table of Contents Abstract ......................................................................................................................................................... 2 Background .................................................................................................................................................. -

Further Insights Into the Regulation of the Fanconi Anemia FANCD2 Protein
University of Rhode Island DigitalCommons@URI Open Access Dissertations 2015 Further Insights Into the Regulation of the Fanconi Anemia FANCD2 Protein Rebecca Anne Boisvert University of Rhode Island, [email protected] Follow this and additional works at: https://digitalcommons.uri.edu/oa_diss Recommended Citation Boisvert, Rebecca Anne, "Further Insights Into the Regulation of the Fanconi Anemia FANCD2 Protein" (2015). Open Access Dissertations. Paper 397. https://digitalcommons.uri.edu/oa_diss/397 This Dissertation is brought to you for free and open access by DigitalCommons@URI. It has been accepted for inclusion in Open Access Dissertations by an authorized administrator of DigitalCommons@URI. For more information, please contact [email protected]. FURTHER INSIGHTS INTO THE REGULATION OF THE FANCONI ANEMIA FANCD2 PROTEIN BY REBECCA ANNE BOISVERT A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN CELL AND MOLECULAR BIOLOGY UNIVERSITY OF RHODE ISLAND 2015 DOCTOR OF PHILOSOPHY DISSERTATION OF REBECCA ANNE BOISVERT APPROVED: Dissertation Committee: Major Professor Niall Howlett Paul Cohen Becky Sartini Nasser H. Zawia DEAN OF THE GRADUATE SCHOOL UNIVERSITY OF RHODE ISLAND 2015 ABSTRACT Fanconi anemia (FA) is a rare autosomal and X-linked recessive disorder, characterized by congenital abnormalities, pediatric bone marrow failure and cancer susceptibility. FA is caused by biallelic mutations in any one of 16 genes. The FA proteins function cooperatively in the FA-BRCA pathway to repair DNA interstrand crosslinks (ICLs). The monoubiquitination of FANCD2 and FANCI is a central step in the activation of the FA-BRCA pathway and is required for targeting these proteins to chromatin. -

Use of the XRCC2 Promoter for in Vivo Cancer Diagnosis and Therapy
Chen et al. Cell Death and Disease (2018) 9:420 DOI 10.1038/s41419-018-0453-9 Cell Death & Disease ARTICLE Open Access Use of the XRCC2 promoter for in vivo cancer diagnosis and therapy Yu Chen1,ZhenLi1,ZhuXu1, Huanyin Tang1,WenxuanGuo1, Xiaoxiang Sun1,WenjunZhang1, Jian Zhang2, Xiaoping Wan1, Ying Jiang1 and Zhiyong Mao 1 Abstract The homologous recombination (HR) pathway is a promising target for cancer therapy as it is frequently upregulated in tumors. One such strategy is to target tumors with cancer-specific, hyperactive promoters of HR genes including RAD51 and RAD51C. However, the promoter size and the delivery method have limited its potential clinical applications. Here we identified the ~2.1 kb promoter of XRCC2, similar to ~6.5 kb RAD51 promoter, as also hyperactivated in cancer cells. We found that XRCC2 expression is upregulated in nearly all types of cancers, to a degree comparable to RAD51 while much higher than RAD51C. Further study demonstrated that XRCC2 promoter is hyperactivated in cancer cell lines, and diphtheria toxin A (DTA) gene driven by XRCC2 promoter specifically eliminates cancer cells. Moreover, lentiviral vectors containing XRCC2 promoter driving firefly luciferase or DTA were created and applied to subcutaneous HeLa xenograft mice. We demonstrated that the pXRCC2-luciferase lentivirus is an effective tool for in vivo cancer visualization. Most importantly, pXRCC2-DTA lentivirus significantly inhibited the growth of HeLa xenografts in comparison to the control group. In summary, our results strongly indicate that virus-mediated delivery of constructs built upon the XRCC2 promoter holds great potential for tumor diagnosis and therapy. -
FANCJ Regulates the Stability of FANCD2/FANCI Proteins and Protects Them from Proteasome and Caspase-3 Dependent Degradation
FANCJ regulates the stability of FANCD2/FANCI proteins and protects them from proteasome and caspase-3 dependent degradation Komaraiah Palle, Ph.D. (Kumar) Assistant Professor of Oncologic Sciences Abraham Mitchell Cancer Research Scholar Mitchell Cancer Institute University of South Alabama Outline • Fanconi anemia (FA) pathway • Role of FA pathway in Genome maintenance • FANCJ and FANCD2 functional relationship • FANCJ-mediated DDR in response to Fork-stalling Fanconi Anemia • Rare, inherited blood disorder. • 1:130,000 births Guido Fanconi 1892-1979 • Affects men and women equally. • Affects all racial and ethnic groups – higher incidence in Ashkenazi Jews and Afrikaners Birth Defects Fanconi anemia pathway • FA is a rare chromosome instability syndrome • Autosomal recessive disorder (or X-linked) • Developmental abnormalities • 17 complementation groups identified to date • FA pathway is involved in DNA repair • Increased cancer susceptibility - many patients develop AML - in adults solid tumors Fanconi Anemia is an aplastic anemia FA patients are prone to multiple types of solid tumors • Increased incidence and earlier onset cancers: oral cavity, GI and genital and reproductive tract head and neck breast esophagus skin liver brain Why? FA is a DNA repair disorder • FA caused by mutations in 17 genes: FANCA FANCF FANCM FANCB FANCG/XRCC9 FANCN/PALB2 FANCC FANCI RAD51C/FANCO FANCD1/BRCA2 FANCJ SLX4/FANCP FANCD2 FANCL ERCC2/XPF/FANCQ FANCE BRCA1/FANCS • FA genes function in DNA repair processes • FA patient cells are highly sensitive -

Fanconi Anemia, Bloom Syndrome and Breast Cancer
A multiprotein complex in DNA damage response network of Fanconi anemia, Bloom syndrome and Breast cancer Weidong Wang Lab of Genetics, NIA A Multi-protein Complex Connects Two Genomic Instability Diseases: Bloom Syndrome and Fanconi Anemia Bloom Syndrome . Genomic Instability: -sister-chromatid exchange . Cancer predisposition . Mutation in BLM, a RecQ DNA Helicase . BLM participates in: HR-dependent DSB repair Recovery of stalled replication forks . BLM works with Topo IIIa and RMI to Suppress crossover recombination Courtesy of Dr. Ian Hickson A Multi-protein Complex Connects Two Genomic Instability Diseases: Bloom Syndrome and Fanconi Anemia P I l o r t n o BLM IP kDa C HeLa BLAP 250 Nuclear Extract 200- BLM* FANCA* 116- TOPO IIIα* 97- BLAP 100 MLH1* BLM IP BLAP 75 * 66- RPA 70 IgG H 45- * 30- RPA32 IgG L 20- * 12- RPA14 Meetei et al. MCB 2003 A Multi-protein Complex Connects Two Genomic Instability Diseases: Bloom Syndrome and Fanconi Anemia P I A C N A F BLM IP HeLa FANCM= FAAP 250 BLAP 250 Nuclear Extract BLM* BLM* * FANCA* FANCA TOPO IIIα* TOPO IIIα* FAAP 100 BLAP 100 FANCB= FAAP 95 MLH1 FANCA IP BLM IP BLAP 75 BLAP 75 RPA70*/FANCG* RPA 70* FANCC*/FANCE* IgG H FANCL= FAAP 43 FANCF* RPA32* IgG L Meetei et al. MCB 2003 Meetei et al. Nat Genet. 2003, 2004, 2005 BRAFT-a Multisubunit Machine that Maintains Genome Stability and is defective in Fanconi anemia and Bloom syndrome BRAFT Super-complex Fanconi Anemia Bloom Syndrome Core Complex Complex 12 polypeptides 7 polypeptides FANCA BLM Helicase (HJ, fork, D-loop), fork FANCC regression, dHJ dissolution Topo IIIα Topoisomerase, FANCE dHJ dissolution FANCF BLAP75 RMI1 FANCG Stimulates dHJ dissolution. -

DNA Damage Response and Cancer Therapeutics Through the Lens of the Fanconi Anemia DNA Repair Pathway Sonali Bhattacharjee* and Saikat Nandi*
Bhattacharjee and Nandi Cell Communication and Signaling (2017) 15:41 DOI 10.1186/s12964-017-0195-9 REVIEW Open Access DNA damage response and cancer therapeutics through the lens of the Fanconi Anemia DNA repair pathway Sonali Bhattacharjee* and Saikat Nandi* Abstract Fanconi Anemia (FA) is a rare, inherited genomic instability disorder, caused by mutations in genes involved in the repair of interstrand DNA crosslinks (ICLs). The FA signaling network contains a unique nuclear protein complex that mediates the monoubiquitylation of the FANCD2 and FANCI heterodimer, and coordinates activities of the downstream DNA repair pathway including nucleotide excision repair, translesion synthesis, and homologous recombination. FA proteins act at different steps of ICL repair in sensing, recognition and processing of DNA lesions. The multi-protein network is tightly regulated by complex mechanisms, such as ubiquitination, phosphorylation, and degradation signals that are critical for the maintenance of genome integrity and suppressing tumorigenesis. Here, we discuss recent advances in our understanding of how the FA proteins participate in ICL repair and regulation of the FA signaling network that assures the safeguard of the genome. We further discuss the potential application of designing small molecule inhibitors that inhibit the FA pathway and are synthetic lethal with DNA repair enzymes that can be used for cancer therapeutics. Keywords: DNA repair, Fanconi Anemia (FA) signaling network, DNA damage response, Cancer therapeutics, Synthetic lethality, Combination Therapy Genomic instability, Interstrand crosslink (ICL), Homologous recombination, Translesion synthesis Background Additional clinical features included microcephaly, vitiligo Fanconi Anemia (FA), a rare genetic cancer-susceptibility and hypoplasia of the testes [8]. After nearly four decades syndrome is a recessive autosomal or X-linked genetic dis- another article reported an accumulation of large number ease [1–3].