Abu Bakr Al-Razi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Naming of Moscows in the USA
Names, Vol. 37, No.1 (March 1989) The Naming of Moscows in the USA Irina Vasiliev Abstract Since 1800, at least forty-seven populated places in the United States have borne the name Moscow. The reasons for having been so named fall into four classes of placename type: commemorative, anticipatory, transfer, and mistake. The stories of these communities and their namings tell much about the growth of this country, the flow of in- formation within it, and each community's perception of itself. ***** The names Berlin, London; Moscow, and Paris evoke images of European sophistication and Old World charm. Here in the United States, these and other European and classical names have been applied as place names to communities that bear no resemblance to the original cities. We have all seen. them on our road maps: the Romes and the Petersburgs, the Viennas and Madrids. They have become commonplace to us. And there are many of each of them: not just one Rome, but thir- ty-five; not just one Cairo, but twenty-one. So the questions come up: Why were these communities named what they were? Who·were the people behind the naming? What were the reasons for the names they chose? It would be too large a task to examine all of the Old W orldnames that have been used across the United States in the last two hundred years. However, I have been able look at one name and determine the reasons for its widespread use. The name that I have chosen to look at is Moscow. -

The Evolution of Hospitals from Antiquity to the Renaissance
Acta Theologica Supplementum 7 2005 THE EVOLUTION OF HOSPITALS FROM ANTIQUITY TO THE RENAISSANCE ABSTRACT There is some evidence that a kind of hospital already existed towards the end of the 2nd millennium BC in ancient Mesopotamia. In India the monastic system created by the Buddhist religion led to institutionalised health care facilities as early as the 5th century BC, and with the spread of Buddhism to the east, nursing facilities, the nature and function of which are not known to us, also appeared in Sri Lanka, China and South East Asia. One would expect to find the origin of the hospital in the modern sense of the word in Greece, the birthplace of rational medicine in the 4th century BC, but the Hippocratic doctors paid house-calls, and the temples of Asclepius were vi- sited for incubation sleep and magico-religious treatment. In Roman times the military and slave hospitals were built for a specialised group and not for the public, and were therefore not precursors of the modern hospital. It is to the Christians that one must turn for the origin of the modern hospital. Hospices, originally called xenodochia, ini- tially built to shelter pilgrims and messengers between various bishops, were under Christian control developed into hospitals in the modern sense of the word. In Rome itself, the first hospital was built in the 4th century AD by a wealthy penitent widow, Fabiola. In the early Middle Ages (6th to 10th century), under the influence of the Be- nedictine Order, an infirmary became an established part of every monastery. -

August 21, 2012 at 3:30 PM Land Use Department SCHOOL FOR
" , **SECOND AMENDED** BOARD OF ADJUSTMENT Tuesday, August 21,2012 at 6:00 P.M. (Note New Time) 200 Lincoln Ave. Santa Fe NM City Council Chambers Field Trip - August 21, 2012 at 3:30 P.M. Land Use Department SCHOOL FOR ADVANCED RESEARCH 660 GARCIA STREET Meet at Reception (main building on left) A. ROLL CALL B. PLEDGE OF ALLEGIANCE C. APPROVAL OF AGENDA D. APPROVAL OF MINUTES: July 17, 2012 minutes E. FINDINGS/CONCLUSIONS: Case #2012-41. 614 Acequia Madre Special Use Permit F. OLD BUSINESS G. NEW BUSINESS Case #2012-77. 341 Magdalena Street Variance Jennifer and Brent Cline, owners, request a variance to allow garage doors to be set back 8 feet from the front property lines where 20 feet is required. The property is 0.2± acres and is zoned R-21 (Residential, 21 dwelling units per acre). (Dan Esquibel, Case Manager) Case #2012-69. Holy Trinity Orthodox Church Special Use Permit. Holy Trinity Orthodox Church requests a Special Use Permit for dormitory boarding and monastery use. The property is zoned R-1 (Residential, one dwelling unit per acre) and is located at 207 East Cordova Road. (William Lamboy, Case Manager) Case #2012-71. School for Advanced Research Special Use Permit. JenkinsGavin Design and Development, agents for School for Advanced Research, request a Special Use Permit to aI/ow a museum use at 660 Garcia Street. The property is zoned R-2 (Residential, two dwelling units per acre) and R-3 (Residential, three dwelling units per acre). (William Lamboy, Case Manager) H. BUSINESS FROM THE FLOOR I. -

SCX-920-System-Controller.Pdf
Infinity SCX 920 System Controller The Infinity SCX 920 is a stand-alone, programmable, microprocessor-based system controller that F E A T U R E S is used for Direct Digital Control of chillers, cooling towers, boilers, air handling units, perimeter • Stand-alone DDC for System radiation, lighting, etc. The Infinet’s true peer-to-peer communication protocol provides the Infinity Reliability SCX 920 with the ability to instantly communicate with Infinity network controllers such as the CX • Peer-to-Peer Communications 9200, as well as the entire network of Andover Infinity controllers. Up to 254 SCX 920s can be Provide Transparent Data networked with the Infinity CX family of controllers. Transfer • Plain English® Language The SCX 920 comes standard with a metal cover plate suitable for panel mounting (shown). Simplifies Programming An optional enclosure is available for wall mounting. • Universal Inputs and Outputs for Flexible Control Configurations COMMUNICATIONS Communication to the Infinity SCX 920 is handled via the Infinet bus, a twisted pair, half duplex RS-485 interface. • Expandable I/O Meets Additional Communication is accomplished with a token passing protocol which provides full transparent data transfer between all Point Count Needs Infinity controllers on the network. • Detachable Input/Output INPUTS Connectors for Easy Installation The Infinity SCX 920 is capable of sensing sixteen inputs. Each input can accept a digital (on/off), counter (up to 4 Hz), voltage (0-10 VDC), or temperature signal. • Full Function Manual Overrides Provide Status Feedback OUTPUTS • Optional Display/Keypad for Local The Infinity SCX 920 has eight Universal outputs providing pulse, variable voltage (0 - 20 VDC), variable current, (0 - 20mA) Information Control or on/off control of motors and lighting with Form C relays. -

Downloaded from Brill.Com10/04/2021 08:59:36AM Via Free Access
Chapter 12 Aristocrats, Mercenaries, Clergymen and Refugees: Deliberate and Forced Mobility of Armenians in the Early Medieval Mediterranean (6th to 11th Century a.d.) Johannes Preiser-Kapeller 1 Introduction Armenian mobility in the early Middle Ages has found some attention in the scholarly community. This is especially true for the migration of individuals and groups towards the Byzantine Empire. A considerable amount of this re- search has focused on the carriers and histories of individual aristocrats or noble families of Armenian origin. The obviously significant share of these in the Byzantine elite has even led to formulations such as Byzantium being a “Greco-Armenian Empire”.1 While, as expected, evidence for the elite stratum is relatively dense, larger scale migration of members of the lower aristocracy (“azat”, within the ranking system of Armenian nobility, see below) or non- aristocrats (“anazat”) can also be traced with regard to the overall movement of groups within the entire Byzantine sphere. In contrast to the nobility, however, the life stories and strategies of individuals of these backgrounds very rarely can be reconstructed based on our evidence. In all cases, the actual signifi- cance of an “Armenian” identity for individuals and groups identified as “Ar- menian” by contemporary sources or modern day scholarship (on the basis of 1 Charanis, “Armenians in the Byzantine Empire”, passim; Charanis, “Transfer of population”; Toumanoff, “Caucasia and Byzantium”, pp. 131–133; Ditten, Ethnische Verschiebungen, pp. 124–127, 134–135; Haldon, “Late Roman Senatorial Elite”, pp. 213–215; Whitby, “Recruitment”, pp. 87–90, 99–101, 106–110; Isaac, “Army in the Late Roman East”, pp. -

Why Did the Import of Dirhams Cease? Viacheslav Kuleshov Institutionen För Arkeologi Och Antikens Kultur Doktorandseminarium 2018-01-31 Kl
Why did the import of dirhams cease? Viacheslav Kuleshov Institutionen för arkeologi och antikens kultur Doktorandseminarium 2018-01-31 Kl. 15-17 1. Introduction The minting of post-reform Islamic silver coins (Kufic dirhams) started under the Umayyad period in 78 AH (697/698). Kufic dirhams were minted using a more or less stable design pattern for more than three centuries until around the middle of the 11th century. The most common are Abbasid and Samanid dirhams of mid-8th to mid- 10th centuries. The later coinages are those of the Buyid, Ziyarid, ‘Uqaylid, Marwanid and Qarakhanid dynasties. 2. Inflows of dirhams under the Abbasid period (750–945), and their silver content The inflow of Kufic dirhams from the Caliphate northwards started as early as around 750. By the beginning of the 9th century the first waves of early Islamic coined silver reached Gotland and Uppland in Sweden, where the oldest grave finds with coins have been discovered. The largest volumes of collected and deposited silver are particularly well recorded in Eastern Europe for the 850s to 860s, 900s to 910s, and 940s to 950s. Of importance is the fact that, as visual examination and many analyses of coins show, from the early 8th to the early 10th centuries an initially established silver content in coins was normally maintained at 92 to 96 per cent. In the first half of the 10th century the same or even higher fineness was typical of the early Samanid dirhams from Central Asia. Such fineness is also evident from colour and metal surface. 3. -

Byzantine Relations with Northern Peoples in the Tenth Century
CONSTANTINE PORPHYROGENITUS, DE ADMINISTRANDO IMPERIO Byzantine Relations with Northern Peoples in the Tenth Century INTRODUCTION Byzantine relations with Bulgaria were complicated in the early years of the tenth century: more complicated than many historians have allowed. The Bulgarian Tsar Symeon (c. 894-927) has been portrayed by both Byzantine and modern authors as an aggressor intent on capturing Constantinople from which he might rule a united Byzantine-Bulgarian empire. However, recent scholarship (notably the work of Bozhilov and Shepard) has questioned this, and maintained that Symeon's ambitions were more limited until the final years of his reign, the 920s, when he engineered a series of confrontations with the Byzantine Emperor Romanos I Lekapenos (920- 44). (We will cover these years elsewhere: see the letters of Nicholas Mystikos and Theodore Daphnopates.) Symeon's died on 27 May 927, and his successor Peter (d. 967) immediately launched a major invasion of the Byzantine administrative district of Macedonia. As one of four sons such a show of strength would have been necessary to secure the support of his father's boyars. However, the Bulgarian troops withdrew swiftly, at the same time razing the fortresses that they had held until then in Thrace, and this early performance was not repeated. Instead, it heralded forty years of apparent harmony and cooperation between the two major powers in the northern Balkans. The reason for the withdrawal, and the centrepiece of the enduring Bulgarian Byzantine accord was the marriage in 927 of Peter to Maria Lecapena, granddaughter of the (senior) ruling emperor Romanus I Lecapenus.Peter has generally been held to have presided over the dramatic decline of Bulgaria. -

Transcontinental Trade and Economic Growth
M. SHATZMILLER: TRANSCONTINENTAL TRADE AND ECONOMIC GROWTH Transcontinental Trade and Economic Growth in the Early Islamic Empire: The Red Sea Corridor in the 8th-10th Centuries Maya Shatzmiller The question of why and how sustained economic growth the long term, it surely qualifies as a ‘trend’ or a ‘cycle’ occurs in historical societies is most frequently studied in in historical economic growth.7 Several long-term fac- relation to the European model, otherwise known as the tors brought about a series of changes in the key econom- ‘Rise of the West’, the only model to have been studied ic components of the empire: an increase in monetary in detail so far.1 The debate continues over why western supply and circulation; the development and elaboration Europe forged ahead and remained so consistently, while of state fiscal institutions with an efficient system of tax other societies, including eastern Europe, were unable to collection; the creation of legal institutions to uphold stage their own ‘rise’ through intensive growth, maintain property rights; demographic growth resulting from both it consistently once it occurred, or indeed successfully internal population growth and the importing of slaves; emulate the European model. On the other hand, there is a increased output in the manufacturing sector as a result mounting feeling of dissatisfaction with the notion of ex- of increased division of labour; and finally, an increased clusiveness and uniqueness which accompanies the debate volume of trade, efficient markets, commercial techniques about ‘The Rise of the West/Europe’.2 Those who study and development of credit tools. It is the trade component non-Western societies suggest that alternative interpreta- that will concern us here, since it presents us with an ele- tions and comparative studies of economic growth do exist ment that is variable in a comparative context – the ele- and should be looked at, rather than simply accepting the ment being the role of intercontinental trade in economic European model at its face value. -
Did Comet HEINRICH-Swift-Tuttle Terminate Roman and Global Civilization? [ROME’S POPULATION CATASTROPHE: G
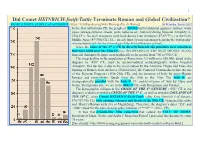
1 Did Comet HEINRICH-Swift-Tuttle Terminate Roman and Global Civilization? [ROME’S POPULATION CATASTROPHE: https://it.wikipedia.org/wiki/Demografia_di_Roma] G. Heinsohn, January 2021 In the first millennium CE, the people of ROME built residential quarters, latrines, water pipes, sewage systems, streets, ports, bakeries etc., but only during Imperial Antiquity (1- 230s CE). No such structures were built during Late Antiquity (4th-6th/7th c.) or the Early Middle Ages (8th-930s CE). [See already https://q-mag.org/gunnar-heinsohn-the-stratigraphy- of-rome-benchmark-for-the-chronology-of-the-first-millennium-ce.html] Since the ruins of the 3rd c. CE lie directly beneath the primitive new structures that were built after the 930s CE (i.e., BEGINNING OF THE HIGH MIDDLE AGES), Imperial Antiquity belongs stratigraphically to the period from 700 to 930s CE. The steep decline in the population of Rome from 1.5 million to 650,000, dated in the diagram to "450" CE, must be accommodated archaeologically within Imperial Antiquity. This decline is due to the crisis caused by the Antonine Plague and Fires, the burning of Rome's State Archives (Tabularium), the Comet of Commodus before the rise of the Severan Emperors (190s-230s CE), and the invasion of Italy by proto-Hunnic Iazyges and proto-Gothic Quadi from the 160s to the 190s. The 160s ff. are stratigraphically parallel with the 450s ff. CE and its invasion of Italy by Huns and Goths. Stratigraphically, we are in the 860s ff. CE, with Hungarians and Vikings. The demographic collapse in the CRISIS OF THE 6th CENTURY (“553” CE in the diagram) is identical with the CRISIS OF THE 3rd C., as well as with the COLLAPSE OF THE 10th C., when Comet HEINRICH-Swift-Tuttle (after King Heinrich I of Saxony; 876/919-936 CE) with ensuing volcanos and floods of the 930s CE ) damaged the globe and Henry’s Roman style city of Magdeburg). -
Medieval Population Dynamics to 1500
Medieval Population Dynamics to 1500 Part C: the major population changes and demographic trends from 1250 to ca. 1520 European Population, 1000 - 1300 • (1) From the ‘Birth of Europe’ in the 10th century, Europe’s population more than doubled: from about 40 million to at least 80 million – and perhaps to as much as 100 million, by 1300 • (2) Since Europe was then very much underpopulated, such demographic growth was entirely positive: Law of Eventually Diminishing Returns • (3) Era of the ‘Commercial Revolution’, in which all sectors of the economy, led by commerce, expanded -- with significant urbanization and rising real incomes. Demographic Crises, 1300 – 1500 • From some time in the early 14th century, Europe’s population not only ceased to grow, but may have begun its long two-century downswing • Evidence of early 14th century decline • (i) Tuscany (Italy): best documented – 30% -40% population decline before the Black Death • (ii) Normandy (NW France) • (iii) Provence (SE France) • (iv) Essex, in East Anglia (eastern England) The Estimated Populations of Later Medieval and Early Modern Europe Estimates by J. C. Russell (red) and Jan de Vries (blue) Population of Florence (Tuscany) Date Estimated Urban Population 1300 120,000 1349 36,000? 1352 41, 600 1390 60,000 1427 37,144 1459 37,369 1469 40,332 1488 42,000 1526 (plague year) 70,000 Evidence of pre-Plague population decline in 14th century ESSEX Population Trends on Essex Manors The Great Famine: Malthusian Crisis? • (1) The ‘Great Famine’ of 1315-22 • (if we include the sheep -

1 Making a Difference in Tenth-Century Politics: King
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by St Andrews Research Repository 1 Making a Difference in Tenth-Century Politics: King Athelstan’s Sisters and Frankish Queenship Simon MacLean (University of St Andrews) ‘The holy laws of kinship have purposed to take root among monarchs for this reason: that their tranquil spirit may bring the peace which peoples long for.’ Thus in the year 507 wrote Theoderic, king of the Ostrogoths, to Clovis, king of the Franks.1 His appeal to the ideals of peace between kin was designed to avert hostilities between the Franks and the Visigoths, and drew meaning from the web of marital ties which bound together the royal dynasties of the early-sixth-century west. Theoderic himself sat at the centre of this web: he was married to Clovis’s sister, and his daughter was married to Alaric, king of the Visigoths.2 The present article is concerned with a much later period of European history, but the Ostrogothic ruler’s words nevertheless serve to introduce us to one of its central themes, namely the significance of marital alliances between dynasties. Unfortunately the tenth-century west, our present concern, had no Cassiodorus (the recorder of the king’s letter) to methodically enlighten the intricacies of its politics, but Theoderic’s sentiments were doubtless not unlike those that crossed the minds of the Anglo-Saxon and Frankish elite families who engineered an equally striking series of marital relationships among themselves just over 400 years later. In the early years of the tenth century several Anglo-Saxon royal women, all daughters of King Edward the Elder of Wessex (899-924) and sisters (or half-sisters) of his son King Athelstan (924-39), were despatched across the Channel as brides for Frankish and Saxon rulers and aristocrats. -

The Tribal Territory of the Kurds Through Arabic Medieval Historiography Boris James
The tribal territory of the Kurds through Arabic medieval historiography Boris James To cite this version: Boris James. The tribal territory of the Kurds through Arabic medieval historiography: Spatial Dynamics, Territorial Categories, and Khaldunian Paradigm. Middle East Studies Association (North America) GatheringPanel : “ Before Nationalism : Land and Loyalty in the Middle East ”, Nov 2007, Montreal, Canada. halshs-00350118 HAL Id: halshs-00350118 https://halshs.archives-ouvertes.fr/halshs-00350118 Submitted on 5 Jan 2009 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. MESA 2007 Panel :Before Nationalism: Land and Loyalty in the Middle East The tribal territory of the Kurds through Arabic medieval historiography: spatial dynamics, territorial categories, and Khaldunian paradigm Boris James (IFPO/ University of Paris 10) In the 14th century an egyptian author, al-Maqrîzî writes : « You should know that nobody agrees on the definition of the Kurds. The ‘Ajam for instance indicate that the Kurds were the favourite food of the king Bayûrasf. He was ordering everyday that two human beings be sacrificed for him so he could consume their flesh. His Vizir Arma’il was sacrificing one and sparing the other who was sent to the mountains of Fârs.