The Integumentary System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nerve Block of Lateral Femoral Cutaneous Nerve of the Thigh
18VTLLAA 1 Nerve block of lateral femoral cutaneous nerve of the thigh. Dr. Robert M Raw (MD) . MBChB, MFGP, MPraxMed, DA, FCA. Professor of Anesthesia retired Editor of Regional-Anesthesia.Com INDEX. 1. Introduction 2. Anatomy 3. Choice of local anesthetic 4. General indications 5. Complications and side effects 6. Conclusion ------------------------------------------------------------------------------------ 1. INTRODUCTION The lateral femoral cutaneous nerve of the thigh (LFCN) is the single human nerve most subject to anatomic variations. Figure #1shows the dermatome of LFCN. The nerve is small and mostly invisible under ultrasound scanning. For nerve block success, drug must be injected into four fascial compartments, each of which a variant nerve type may pass through in different individuals. 2. ANATOMY The lateral femoral cutaneous nerve is a sensory nerve supplying the skin on the lateral aspect of the thigh. That sensory area nearly reaches the thigh posterior midline and the thigh anterior midline. Its superior limit passes over the greater trochanter and its inferior limit nearly reaches the height of the patella. The typical LCNT, in 60% of patients, is a branch of the lumbar plexus deriving from the dorsal divisions of nerve roots L2 and L3. The LFCN forms within the psoas muscle, and exits the pelvis medial to the anterior superior iliac spine (ASIS) and under the inguinal ligament. It then passes over the sartorius muscle, under fascia lata, before branching into its final Figure 1. Classic dermatomal distribution of the divisions. In forty percent of patients the LFCN lateral femoral cutaneous nerve (LFCN), derived has completely different anatomy, but from Sobotta. fortunately the nerve always passes in proximity to the proximal sartorius muscle. -

Diapositiva 1
Ingegneria delle tecnologie per la salute Fondamenti di anatomia e istologia Apparato tegumentario aa. 2017-18 INTEGUMENTARY SYSTEM integumentary system = refers to skin and its accessory structures responsible for much more than simply human outward appearance: about 16% of body weight, covering an area of 1.5 to 2 m2 (= largest organ system in human body). • skin protects inner organs INTEGUMENTARY SYSTEM • skin = even not typical, but an organ, made of tissues that work together as a single structure to perform unique and critical functions • integumentary system = skin + its accessory structures, providing body with overall protection. • made of multiple layers of cells and tissues, which are held to underlying structures by connective tissue: deeper layer of skin is well vascularized (has numerous blood vessels) and also has numerous sensory, and autonomic and sympathetic nerve fibers ensuring communication to and from brain. INTEGUMENTARY SYSTEM Overview • Largest organ (15% of body weight) • Epidermis – keratinized stratified squamous epithelium • Dermis – connective tissue layer • Hypodermis • Thickness variable, normally 1-2 mm – dermis may thicken, up to 6 mm – stratum corneum layer increased • calluses on hands and feet Structure of the Skin 2 layers: epidermis + dermis SKIN: histology SKIN: histology SKIN: histology Cells of the Epidermis • Stem cells – undifferentiated cells in deepest layers • Keratinocytes – most of the skin cells • Melanocytes – synthesize pigment that shield UV • Tactile (merkel) cells – receptor cells associated with nerve fibers • Dendritic (langerhans) cells – macrophages guard against pathogens Cell and Layers of the Epidermis Epidermis: histology = composed of keratinized, stratified squamous epithelium, made of 4 or 5 layers of epithelial cells, depending on its location in body. -

Preparatory: 1 Venous Access and Medication Administration: 4
Preparatory: 1 Venous Access and Medication Administration: 4 W4444444444444444444444444444444444444444444444444444444444444444444444444444444444444444444444444444444444444 UNIT TERMINAL OBJECTIVE 1-4 At the completion of this unit, the EMT-Critical Care Technician student will be able to safely and precisely access the venous circulation and administer medications. COGNITIVE OBJECTIVES At the completion of this unit, the EMT-Critical Care Technician student will be able to: 1-4.1 Review the specific anatomy and physiology pertinent to medication administration. (C-1) 1-4.2 Review mathematical principles. (C-1) 1-4.3 Review mathematical equivalents. (C-1) 1-4.4 Differentiate temperature readings between the Centigrade and Fahrenheit scales. (C-3) 1-4.5 Discuss formulas as a basis for performing drug calculations. (C-1) 1-4.6 Calculate oral and parenteral drug dosages for all emergency medications administered to adults, infants and children. (C-2) 1-4.7 Calculate intravenous infusion rates for adults, infants, and children. (C-2) 1-4.8 Discuss legal aspects affecting medication administration. (C-1) 1-4.9 Discuss the "six rights" of drug administration and correlate these with the principles of medication administration. (C-1) 1-4.10 Discuss medical asepsis and the differences between clean and sterile techniques. (C-1) 1-4.11 Describe use of antiseptics and disinfectants. (C-1) 1-4.12 Describe the use of universal precautions and body substance isolation (BSI) procedures when administering a medication. (C-1) 1-4.13 Describe the indications, equipment needed, techniques utilized, precautions, and general principles of peripheral venous cannulation (Including saline locks). (C-1) 1-4.14 Describe the indications, equipment needed, techniques utilized, precautions, and general principles of intraosseous needle placement and infusion. -

CHAPTER 4 the Integumentary System
CHAPTER 4 The Integumentary System LEARNING OBJECTIVES Upon completion of this chapter, you should be able to: • Name the two layers of the skin. • Name the accessory structures of the integumentary system. • Build and pronounce medical terms of the integumentary system. • Name the disorders and treatments relating to the integumentary system. • Name the major classifi cations of pharmacologic agents used to treat skin disorders. • Analyze and defi ne the new terms introduced in this chapter. • Interpret abbreviations associated with the integumentary system. 53 54 PART TWO • BODY SYSTEMS Introduction The largest organ of the body is the skin. The skin covers the entire body—more than 20 square feet on average—and weighs about 24 pounds. It is part of the integumentary system, which also includes the accessory structures: hair, nails, and sebaceous (oil) and sudoriferous (sweat) glands. Integumentum is Latin for “covering” or “shelter.” The physician who specializes in the diag- nosis and treatment of skin disorders is called a dermatologist (dermat/o being one of the com- bining forms for skin). Coupling the root dermat/o with the previously learned suffi x -logy gives us the term dermatology , which is the term for the specialty practice that deals with the skin. Word Elements The major word elements that relate to the integumentary system consist of various anatomical components, accessory structures, colors of the skin, and abnormal conditions. The Word Ele- ments table lists many of the roots, their meanings, and examples associated -

Handbook ESRA
TECHNIQUES HEAD & NECK 4 Intracranial surgery p. 3 Eye blocks p. 5 Face anatomy p. 16 Face particularity p. 23 Ophtalmic nerve blocks p. 27 Maxillary nerve blocks p. 33 Mandibular nerve blocks p. 46 THORAX & ABDOMEN 50 Epidural anaesthesia in Cardio-thoracic surgery p. 50 Ilioinguinal-Iliohypogastric block p. 55 Peri-umbilical & Rectus sheath block p. 57 Pudendal block p. 58 UPPER LIMB 61 Choice of a technique p. 61 Brachial plexus anatomy p. 65 Interscalen block p. 68 Supraclavicular blocks p. 73 Infraclavicular blocks p. 80 Axillary block p. 83 LOWER LIMB 90 Lumbar plexus block p. 90 Iliofascial block p. 100 Obturator block p. 102 Sciatic blocks o Sciatic blocks - parasacral nerve approach p. 109 o Sciatic blocks - posterior popliteal approach p. 115 Ankle blocks p. 119 AXIAL BLOCKS 123 Lumbar epidural p. 123 OBSTETRICS AXIAL BLOCKS 126 Epidural p. 126 PERIPHERAL BLOCKS Pudendal block p. 58 2 Aknowledgement The provenience of the materials included in this handbook is from the Learning Zone on the official site of “European Society of Regional Anesthesia and Pain Therapy”. http://www.esra-learning.com/ 2007 3 HEAD & TABLE OF CONTENTS NECK • Intracranial surgery • Eye blocks • Face anatomy • Face particularity • Ophtalmic nerve blocks • Maxillary nerve blocks • Mandibular nerve blocks • Cervical plexus blocks HEAD & INTRACRANIAL SURGERY NECK Paul J. Zetlaoui, M.D. Kremlin-Bicetre - France In intra-cranial neurosurgery, scalp infiltration aims to prevent systematic and cerebral hemodynamic variations, contemporary of skin incision. The potential morbidity of these hypertension-tachycardia episodes, even in patients profoundly anaesthetized, is secondary in the increase of the cerebral blood flow and in its deleterious consequences on intra-cranial pressure in these compromised patients. -

The Development of an Intramuscular Injection Simulation for Nursing Students
Open Access Technical Report DOI: 10.7759/cureus.12366 The Development of an Intramuscular Injection Simulation for Nursing Students Julia Micallef 1 , Artur Arutiunian 1 , Adam Dubrowski 1 1. Health Sciences, Ontario Tech University, Oshawa, CAN Corresponding author: Adam Dubrowski, [email protected] Abstract Intramuscular (IM) injections are preferred over subcutaneous injections for administering medicine such as epinephrine and vaccines as the muscle tissue contains an increased vascular supply that provides ideal absorption of the drug being administered. However, administering an IM injection requires clinical judgment when choosing the injection site, understanding the relevant anatomy and physiology as well as the principles and techniques for administering an IM injection. Therefore, it is essential to learn and perform IM injections using injection simulators to practice the skill before administering to a real patient. Current IM injection simulators either favor realism at the expense of standardization or are expensive but do not provide a realistic experience. Therefore, it is imperative to develop an inexpensive but realistic intramuscular injection simulator that can be used to train nursing students so that they can be prepared for when they enter the clinical setting. This technical report aims to provide an overview of the development of an inexpensive and realistic deltoid simulator geared to teach nursing students the skill of IM injections. After development, the IM simulators were tested and validated by practicing nurses. An 18-item survey was administered to the nurses, and results indicated positive feedback about the realism of the simulator, in comparison to previous models used, such as the Wallcur® PRACTI-Injecta Pads (Wallcur LLC, San Diego, CA). -

Ch7 Basic Body Structure and Function Test&A
Chapter 7- Test Name: Basic Body Structure & Fuction Date: 1. Physiology is the study of A) what body parts look like and where they are located. B) the structure and function of the human body. C) how the various body parts work. D) how organisms are created. 2. The basic unit of life is A) a cell. B) a tissue. C) an organ. D) an organ system. 3. Which one of the following is like the cell's brain? A) The cytoplasm B) The cell nucleus C) The cell organelles D) The cell membrane 4. Which cell transports oxygen throughout the body? A) Red blood B) Epithelial C) Muscle D) Nerve 5. Which one of the following is considered connective tissue? A) Mucous membrane B) Blood C) Skin D) Glands 6. Which one of the following organs is included in the integumentary system? A) The fingernails B) The gallbladder C) The pancreas D) The ureters 7. What does epithelial tissue do? A) It connects tissues together. B) It produces movement. C) It conducts information. D) It protects the body. Page 1 8. Which statement correctly describes homeostasis? A) It causes problems by invading otherwise healthy tissues. B) It reduces the immune system's ability to fight off infection. C) It is a state of balance achieved by all of the organ systems working together. D) It occurs when the structure or function of an organ or organ system is abnormal. 9. The purpose of melanin is to A) keep the skin lubricated. B) aid in temperature regulation. C) give our skin, hair, and eyes color. -

The Digestive System
69 chapter four THE DIGESTIVE SYSTEM THE DIGESTIVE SYSTEM The digestive system is structurally divided into two main parts: a long, winding tube that carries food through its length, and a series of supportive organs outside of the tube. The long tube is called the gastrointestinal (GI) tract. The GI tract extends from the mouth to the anus, and consists of the mouth, or oral cavity, the pharynx, the esophagus, the stomach, the small intestine, and the large intes- tine. It is here that the functions of mechanical digestion, chemical digestion, absorption of nutrients and water, and release of solid waste material take place. The supportive organs that lie outside the GI tract are known as accessory organs, and include the teeth, salivary glands, liver, gallbladder, and pancreas. Because most organs of the digestive system lie within body cavities, you will perform a dissection procedure that exposes the cavities before you begin identifying individual organs. You will also observe the cavities and their associated membranes before proceeding with your study of the digestive system. EXPOSING THE BODY CAVITIES should feel like the wall of a stretched balloon. With your skinned cat on its dorsal side, examine the cutting lines shown in Figure 4.1 and plan 2. Extend the cut laterally in both direc- out your dissection. Note that the numbers tions, roughly 4 inches, still working with indicate the sequence of the cutting procedure. your scissors. Cut in a curved pattern as Palpate the long, bony sternum and the softer, shown in Figure 4.1, which follows the cartilaginous xiphoid process to find the ventral contour of the diaphragm. -

Pressure Ulcer Staging Guide
Pressure Ulcer Staging Guide Pressure Ulcer Staging Guide STAGE I STAGE IV Intact skin with non-blanchable Full thickness tissue loss with exposed redness of a localized area usually Reddened area bone, tendon, or muscle. Slough or eschar may be present on some parts Epidermis over a bony prominence. Darkly Epidermis pigmented skin may not have of the wound bed. Often includes undermining and tunneling. The depth visible blanching; its color may Dermis of a stage IV pressure ulcer varies by Dermis differ from the surrounding area. anatomical location. The bridge of the This area may be painful, firm, soft, nose, ear, occiput, and malleolus do not warmer, or cooler as compared to have subcutaneous tissue and these adjacent tissue. Stage I may be Adipose tissue ulcers can be shallow. Stage IV ulcers Adipose tissue difficult to detect in individuals with can extend into muscle and/or Muscle dark skin tones. May indicate "at supporting structures (e.g., fascia, Muscle risk" persons (a heralding sign of Bone tendon, or joint capsule) making risk). osteomyelitis possible. Exposed bone/ Bone tendon is visible or directly palpable. STAGE II DEEP TISSUE INJURY Partial thickness loss of dermis Blister Purple or maroon localized area of Reddened area presenting as a shallow open ulcer discolored intact skin or blood-filled Epidermis with a red pink wound bed, without Epidermis blister due to damage of underlying soft slough. May also present as an tissue from pressure and/or shear. The intact or open/ruptured serum-filled Dermis area may be preceded by tissue that is Dermis blister. -

Bio-Implant Reference Manual
Bio-Implant Reference Manual International Use Only Bio-Implant Reference Manual Saving Lives, Restoring Health is our business. Nowhere is the reality of death more evident than in the decision-making process surrounding tissue and organ donation. It’s a course of action that involves everything from the simple to the complex, from the sadly certain to the certainly optimistic. LifeNet Health takes this tragedy and turns it into hope. Our full line of allograft bio-implants maximizes the precious gift of donated tissue and provides surgeons with the tools they need to improve the lives of patients. By making the finest quality allograft bio-implants easily accessible, we continue to provide exemplary service to clinicians and hospitals. Every year, LifeNet Health distributes over 400,000 bio-implants to meet the urgent needs of hospitals and patients around the world. Our record of safety is unmatched. And our philosophy is simple: When partnering with a bio-implant supplier, your decision should not be based solely on fee, but rather on the overall value you and your patients expect and deserve. At LifeNet Health, we deliver that value by excelling in these critical areas – safety, quality, innovation, service, clinical effectiveness, supply chain reliability and and experience. With LifeNet Health as your primary bio-implant supplier, you are investing in the best possible value to ensure the well-being of your patients and the reputation of your hospital. This is the value of working with LifeNet Health. 2 757-464-4761 x 2000 (OUS) • 888-847-7831 (US & Canada) • ©2014 LifeNet Health, Virginia Beach, VA. -
The Integumentary System
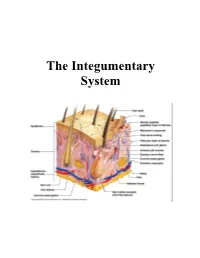
The Integumentary System THE INTEGUMENTARY SYSTEM Skin is the system of the body that makes an individual beautiful! Skin/fur coloration allows animals to be camouflaged. *The skin is the largest organ of the body. The skin and its derivatives (hair, nails, sweat and oil glands) make up the integumentary system. The total surface area of the skin is about 1.8 m² and its total weight is about 11 kg. The skin gives us our appearance and shape. Anatomy of the Skin • Skin is made up of two layers that cover a third fatty layer. The outer layer is called the epidermis; it is a tough protective layer. The second layer (located under the epidermis) is called the dermis; it contains nerve endings, sweat glands, oil glands, and hair follicles. Under these two skin layers is a fatty layer called the subcutaneous tissue, or hypodermis. 1 • The dermis is home to the oil glands. These are also called sebaceous glands, and they are always producing sebum. Sebum is your skin's own natural oil. It rises to the surface of your epidermis to keep your skin lubricated and protected. It also makes your skin waterproof. • Skin is alive! It's made of many thin sheets of flat, stacked cells. Older cells are constantly being pushed to the surface by new cells, which grow from below. When the old ones reach the top, they become wider and flatter as they get rubbed and worn by all your activity. And, sooner or later, they end up popping off like tiles blown from a roof in a strong wind. -
The Integumentary System (In Teg Yoo MEN Tuh Ree) Skin, Tissues, and You � the Integumentary System Is the Body’S Outer Covering
The Integumentary System (In teg yoo MEN tuh ree) Skin, Tissues, and You ! " The Integumentary system is the body’s outer covering. It has the task of physically separating the body from the external environment. This is the first key to homeostasis. ! " Homeostasis: The internal stability or “steady state” maintained by your body. We maintain a body temperature of 98.6ºF (37ºC) ! " The Integumentary system isn’t perfect. Cuts and other injuries break the barrier of the system and allow microorganisms to enter the body. Also, extensive exposure to the sun can cause damage to the tissue. Other harmful agents can damage the system as well. http://academic.kellogg.edu/herbrandsonc/bio201_mckinley/f5-1_layers_of_the_inte_c.jpg The Skin and Tissue Tissues ! " Your body contains 250 different types of cells. ! " Groups of similar cells with common function are called tissues. ! " Tissues protect the body, connect body parts together, some lift and move the body, some transmit http://asweknowit.net/images_edu/dwa5%20tissues.jpg information. Epithelial Tissue ! " Epithelial tissue: sheets of closely packed cells that cover the entire surface of your body and form the lining of your internal organs, many different types all serve the general function of protecting the tissues and organs they cover ! " In your respiratory system, ! " 1st type; line your windpipe and its major branches, cells secrete mucus which traps dust, pollen. etc. cilia sweep them up to throat to be swallowed, ! " 2nd type; lines narrower airways cells have smooth surface allows