Manipulating the Mind: the Ethics of Cognitive Enhancement
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
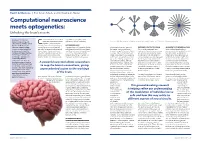
Computational Neuroscience Meets Optogenetics: Unlocking the Brain’S Secrets
Health & Medicine ︱ Prof Simon Schultz and Dr Konstantin Nikolic Computational neuroscience meets optogenetics: Unlocking the brain’s secrets Working at the interface omposed of billions of specialised responsible for perception, action Simplified models allow researchers to study how the geometry of a neuron’s “dendritic tree” affects its ability to process information. between engineering and nerve cells (called neurons) wired and memory. But this is changing. neuroscience, Professor Simon C together in complex, intricate Schultz and Dr Konstantin webs, the brain is inherently challenging LET THERE BE LIGHT Nikolic at Imperial College to study. Neurons communicate with A powerful new tool (invented by Boyden of Neurotechnology and Director of SHEDDING LIGHT ON THE BRAIN AN INSIGHT INTO NEURONAL GAIN London are developing tools each other by transmitting electrical and and Deisseroth just a little over a decade the Imperial Centre of Excellence in Their innovative approach uses Using two biophysical models of to help us understand the chemical signals along neural circuits: ago) allows researchers to map the brain’s Neurotechnology, Dr Konstantin Nikolic, sophisticated two-photon microscopy, neurons, genetically-modified to include intricate workings of the brain. signals that vary both in space and time. connections, giving unprecedented Associate Professor in the Department optogenetics and electrophysiology two distinct light-sensitive proteins Combining a revolutionary Until now, technical limitations in the access to the workings of the brain. Its of Electrical and Electronic Engineering, to measure (and disturb) patterns of (called opsins): channelrhodopsin-2 technology – optogenetics available research methods to study the impressive resolution enables precise and Dr Sarah Jarvis are taking a unique neuronal activity in vivo (in living tissue). -

Implantable Microelectrodes on Soft Substrate with Nanostructured Active Surface for Stimulation and Recording of Brain Activities Valentina Castagnola
Implantable microelectrodes on soft substrate with nanostructured active surface for stimulation and recording of brain activities Valentina Castagnola To cite this version: Valentina Castagnola. Implantable microelectrodes on soft substrate with nanostructured active sur- face for stimulation and recording of brain activities. Micro and nanotechnologies/Microelectronics. Universite Toulouse III Paul Sabatier, 2014. English. tel-01137352 HAL Id: tel-01137352 https://hal.archives-ouvertes.fr/tel-01137352 Submitted on 31 Mar 2015 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. THÈSETHÈSE En vue de l’obtention du DOCTORAT DE L’UNIVERSITÉ DE TOULOUSE Délivré par : l’Université Toulouse 3 Paul Sabatier (UT3 Paul Sabatier) Présentée et soutenue le 18/12/2014 par : Valentina CASTAGNOLA Implantable Microelectrodes on Soft Substrate with Nanostructured Active Surface for Stimulation and Recording of Brain Activities JURY M. Frédéric MORANCHO Professeur d’Université Président de jury M. Blaise YVERT Directeur de recherche Rapporteur Mme Yael HANEIN Professeur d’Université Rapporteur M. Pascal MAILLEY Directeur de recherche Examinateur M. Christian BERGAUD Directeur de recherche Directeur de thèse Mme Emeline DESCAMPS Chargée de Recherche Directeur de thèse École doctorale et spécialité : GEET : Micro et Nanosystèmes Unité de Recherche : Laboratoire d’Analyse et d’Architecture des Systèmes (UPR 8001) Directeur(s) de Thèse : M. -

ECE 5070: Neuroengineering and Neuroprosthetics
ECE 5070: Neuroengineering and Neuroprosthetics Course Description An overview of the broad field of Neuroengineering for graduate and senior undergraduate students with engineering or neuroscience backgrounds. Focusing on neural interfaces and prostheses, this course covers from basic neurophysiology and computational neuronal models to advanced neural interfaces and prostheses currently being actively developed in the field. Transcript Abbreviation: Neur Eng & Prosth Grading Plan: Letter Grade Course Deliveries: Classroom Course Levels: Undergrad, Graduate Student Ranks: Junior, Senior, Masters, Doctoral Course Offerings: Autumn Flex Scheduled Course: Never Course Frequency: Even Years Course Length: 14 Week Credits: 3.0 Repeatable: No Time Distribution: 3.0 hr Lec Expected out-of-class hours per week: 6.0 Graded Component: Lecture Credit by Examination: No Admission Condition: No Off Campus: Never Campus Locations: Columbus Prerequisites and Co-requisites: Prereq: 3050 or BME 3703; or Neurosc 3010; or Grad standing in Engineering or Neurosc. Exclusions: Not open to students with credit for 5194.03 or Neurosc 5070. Cross-Listings: Cross-listed in Neurosc. Course Rationale: Introduce students a vibrant, interdisciplinary field which integrates engineering and neuroscience principles for treating neurological disorders. The course is required for this unit's degrees, majors, and/or minors: No The course is a GEC: No The course is an elective (for this or other units) or is a service course for other units: Yes Subject/CIP Code: 14.1001 Subsidy Level: Doctoral Course Programs Abbreviation Description CpE Computer Engineering EE Electrical Engineering Course Goals Master principles of neural interfaces. Be competent with computational neural models. Be competent with design of common neuroprostheses. -

New Technologies for Human Robot Interaction and Neuroprosthetics
University of Plymouth PEARL https://pearl.plymouth.ac.uk Faculty of Science and Engineering School of Engineering, Computing and Mathematics 2017-07-01 Human-Robot Interaction and Neuroprosthetics: A review of new technologies Cangelosi, A http://hdl.handle.net/10026.1/9872 10.1109/MCE.2016.2614423 IEEE Consumer Electronics Magazine All content in PEARL is protected by copyright law. Author manuscripts are made available in accordance with publisher policies. Please cite only the published version using the details provided on the item record or document. In the absence of an open licence (e.g. Creative Commons), permissions for further reuse of content should be sought from the publisher or author. CEMAG-OA-0004-Mar-2016.R3 1 New Technologies for Human Robot Interaction and Neuroprosthetics Angelo Cangelosi, Sara Invitto Abstract—New technologies in the field of neuroprosthetics and These developments in neuroprosthetics are closely linked to robotics are leading to the development of innovative commercial the recent significant investment and progress in research on products based on user-centered, functional processes of cognitive neural networks and deep learning approaches to robotics and neuroscience and perceptron studies. The aim of this review is to autonomous systems [2][3]. Specifically, one key area of analyze this innovative path through the description of some of the development has been that of cognitive robots for human-robot latest neuroprosthetics and human-robot interaction applications, in particular the Brain Computer Interface linked to haptic interaction and assistive robotics. This concerns the design of systems, interactive robotics and autonomous systems. These robot companions for the elderly, social robots for children with issues will be addressed by analyzing developmental robotics and disabilities such as Autism Spectrum Disorders, and robot examples of neurorobotics research. -

Brain-Machine Interface: from Neurophysiology to Clinical
Neurophysiology of Brain-Machine Interface Rehabilitation Matija Milosevic, Osaka University - Graduate School of Engineering Science - Japan. Abstract— Long-lasting cortical re-organization or II. METHODS neuroplasticity depends on the ability to synchronize the descending (voluntary) commands and the successful execution Stimulation of muscles with FES was delivered using a of the task using a neuroprosthetic. This talk will discuss the constant current biphasic waveform with a 300μs pulse width neurophysiological mechanisms of brain-machine interface at 50 Hz frequency via surface electrodes. First, repetitive (BMI) controlled neuroprosthetics with the aim to provide transcranial magnetic stimulation (rTMS) intermittent theta implications for development of technologies for rehabilitation. burst protocol (iTBS) was used to induce cortical facilitation. iTBS protocol consists of pulses delivered intermittently at a I. INTRODUCTION frequency of 50 Hz and 5 Hz for a total of 200 seconds. Functional electrical stimulation (FES) neuroprosthetics Moreover, motor imagery protocol was used to display a can be used to applying short electric impulses over the virtual reality hand opening and closing sequence of muscles or the nerves to generate hand muscle contractions movements (hand flexion/extension) while subject’s hands and functional movements such as reaching and grasping. remained at rest and out of the visual field. Our work has shown that recruitment of muscles using FES goes beyond simple contractions, with evidence suggesting III. RESULTS re-organization of the spinal reflex networks and cortical- Our first results showed that motor imagery can affect level changes after the stimulating period [1,2]. However, a major challenge remains in achieving precise temporal corticospinal facilitation in a phase-dependent manner, i.e., synchronization of voluntary commands and activation of the hand flexor muscles during hand closing and extensor muscles [3]. -
Practical and Ethical Issues at the Intersection of Brain Science and Society
Emerging Neurotechnologies: Practical and Ethical Issues at the Intersection of Brain Science and Society James Giordano PhD Departments of Neurology and Biochemistry Neuroethics Studies Program, Pellegrino Center for Clinical Bioethics Georgetown University Medical Center Washington, DC, USA and EU-Human Brain Project SP-12 Uppsala University, Sweden Neuroscience… • Huge leaps using technology to study and understand how nervous systems and brains are structured and function. Allowed understanding at certain levels of causality: – Formal: Overall “workings” of biological systems – Material: Structure and functional roles of neurons, glia But not at others… – Efficient: How “grey stuff” actually makes “great stuff” – Final: For what? To what “ends”? Core Questions... What do we do with the information and capability we have? What do we do about the information and capability we don’t? Questions toward Innovation • Tools to Theory • Theory to Tools... ...to Theory AISC Approach Brain Science on the World Stage • EU Human Brain Project • US BRAIN initiative • China Brain Project • Japan Brain Project • Global NeuroS/T Economic Predictions 2025 – Asia – US/Western Europe – South America Neuroscience and Technologies (NeuroS/T) • Assessment – Biomarkers – Genetics/genomics – Imaging – Brain modeling/mapping • Interventional – Technopharmaceutics – P-Stim – Neurofeedback – Transcranial Modulation – Deep Brain Stimulation – BCI – Neuroprosthetics • Derivative – -Artificial neural networks – -AI technologies A-3: Actual Ability to Assess...Access...Affect To What Effect(s) and Ends? Neuroimaging – PET – CT – MR – fMR – DTI – MEG/qEEG Can we Scan the Brain to Depict Consciousness and/or “Read” Minds? text copyright, J. Giordano, 2014 Neurogenetics – Genotyping – Phenotyping – Proteomics – Genetic Intervention(s) Can we “Predict” or “Create” Present and Future “Selves”? text copyright, J. -
A Framework to Assess the Military Ethics of Human Enhancement Technologies
2017-06-09 DRDC-RDDC-2017-L167 Produced for: Paul Comeau, DRDC Chief Scientist Scientific Letter A Framework to Assess the Military Ethics of Human Enhancement Technologies Key Points . Human enhancements may be achieved through devices or drugs that augment or modify human performance. Militaries have used enhancements for years to improve soldier performance. Science and technology progress in human enhancements have outpaced regulatory policies. Emerging enhancements may raise ethical questions and face policy barriers that impede their development, evaluation and eventual adoption by the Canadian Armed Forces (CAF). It is imperative to consider the military ethical issues raised by human enhancement technologies before they are adopted by the CAF. A framework was developed to assess the military ethical issues associated with human enhancements. Identifying potential ethical issues early will enable policymakers to design policies that ensure the safe and ethical use of human enhancements, and will also allow the CAF to be prepared to deal with enhanced adversaries. Background Human enhancement has been defined in the literature in various ways.1-3 We define it herein as any science and technology (S&T) approach that temporarily or permanently modifies or contributes to human functioning. S&T efforts to enhance human health and performance are not new; vaccines (considered enhancements because they augment the immune system’s ability to protect against disease) have been used since the 18th century.4 Human enhancements permeate many aspects of society. Wearable health monitors like FitBits, which can inform changes in behaviour to improve health,5,6 are used by millions of people worldwide. -

Encyclopedia of Computational Neuroscience
Encyclopedia of Computational Neuroscience Dieter Jaeger • Ranu Jung Editors Encyclopedia of Computational Neuroscience With 1109 Figures and 71 Tables Editors Dieter Jaeger Ranu Jung Department of Biology Department of Biomedical Engineering Emory University Florida International University Atlanta, GA, USA Miami, FL, USA ISBN 978-1-4614-6674-1 ISBN 978-1-4614-6675-8 (eBook) ISBN 978-1-4614-6676-5 (print and electronic bundle) DOI 10.1007/978-1-4614-6675-8 Springer New York Heidelberg Dordrecht London Library of Congress Control Number: 2014958664 # Springer Science+Business Media New York 2015 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. Exempted from this legal reservation are brief excerpts in connection with reviews or scholarly analysis or material supplied specifically for the purpose of being entered and executed on a computer system, for exclusive use by the purchaser of the work. Duplication of this publication or parts thereof is permitted only under the provisions of the Copyright Law of the Publisher’s location, in its current version, and permission for use must always be obtained from Springer. Permissions for use may be obtained through RightsLink at the Copyright Clearance Center. Violations are liable to prosecution under the respective Copyright Law. The use of general descriptive names, registered names, trademarks, service marks, etc. -

Ethics in Published Brain–Computer Interface Research
Journal of Neural Engineering PERSPECTIVE Related content - Informed consent in implantable BCI Ethics in published brain–computer interface research: identification of research risks and recommendations for development of best practices research Eran Klein and Jeffrey Ojemann - Ethical issues in neuroprosthetics To cite this article: L Specker Sullivan and J Illes 2018 J. Neural Eng. 15 013001 Walter Glannon - Perspective Patrick Rousche, David M Schneeweis, Eric J Perreault et al. View the article online for updates and enhancements. This content was downloaded from IP address 128.189.236.17 on 21/01/2019 at 19:11 IOP Journal of Neural Engineering Journal of Neural Engineering J. Neural Eng. J. Neural Eng. 15 (2018) 013001 (6pp) https://doi.org/10.1088/1741-2552/aa8e05 15 Perspective 2018 Ethics in published brain–computer © 2018 IOP Publishing Ltd interface research JNEIEZ L Specker Sullivan2 and J Illes1 013001 1 National Core for Neuroethics, University of British Columbia, Vancouver, Canada 2 Center for Bioethics, Harvard Medical School, Boston, MA, United States of America L Specker Sullivan and J Illes E-mail: [email protected] Received 6 June 2017, revised 14 September 2017 Accepted for publication 21 September 2017 Published 8 January 2018 Printed in the UK Abstract Objective. Sophisticated signal processing has opened the doors to more research with human JNE subjects than ever before. The increase in the use of human subjects in research comes with a need for increased human subjects protections. Approach. We quantified the presence or 10.1088/1741-2552/aa8e05 absence of ethics language in published reports of brain–computer interface (BCI) studies that involved human subjects and qualitatively characterized ethics statements. -

Help, Hope, and Hype: Ethical Dimensions of Neuroprosthetics
Will brain and/or neural control of a prosthetic POLICY FORUM hand soon be a commonplace? brain processes occur unconsciously, and the highly complex computations in the brain are difficult to resolve. Human ac- countability for injuries caused in the use of such a symbiotic robot might occur in several ways. First, where there is a form of “veto” built into the system [e.g., override through voluntary ocular movements (1)], a person could be held liable for failing to exercise the veto, just as a driver may be re- sponsible for failing to apply brakes. Second, using an unpredictable or poorly TECHNOLOGY AND ETHICS controllable semiautonomous robot in cir- cumstances posing a risk of injury may be viewed as negligent (e.g., using it to pick up a Help, hope, and hype: Ethical baby, versus using it for other, less-risky activ- ities). Holding people responsible for injuries they inflict despite their lacking capacity or Downloaded from dimensions of neuroprosthetics control at the time of the injury is consistent with theories of moral and legal responsibil- Accountability, responsibility, privacy, and security are key ity (13), e.g., holding a driver responsible for injuries caused during an epileptic seizure if By Jens Clausen,1 Eberhard Fetz,2 John the fear of losing privacy and autonomy and the driver knowingly failed to take antisei- 3 4 Donoghue, Junichi Ushiba, Ulrike of self-dissolution. zure medication properly (14). Accordingly, http://science.sciencemag.org/ Spörhase,1 Jennifer Chandler,5 Niels These fears may seem exaggerated in light the user’s responsibility may transfer from Birbaumer,3,6 Surjo R. -

Cyborgs and Enhancement Technology
philosophies Article Cyborgs and Enhancement Technology Woodrow Barfield 1 and Alexander Williams 2,* 1 Professor Emeritus, University of Washington, Seattle, Washington, DC 98105, USA; [email protected] 2 140 BPW Club Rd., Apt E16, Carrboro, NC 27510, USA * Correspondence: [email protected]; Tel.: +1-919-548-1393 Academic Editor: Jordi Vallverdú Received: 12 October 2016; Accepted: 2 January 2017; Published: 16 January 2017 Abstract: As we move deeper into the twenty-first century there is a major trend to enhance the body with “cyborg technology”. In fact, due to medical necessity, there are currently millions of people worldwide equipped with prosthetic devices to restore lost functions, and there is a growing DIY movement to self-enhance the body to create new senses or to enhance current senses to “beyond normal” levels of performance. From prosthetic limbs, artificial heart pacers and defibrillators, implants creating brain–computer interfaces, cochlear implants, retinal prosthesis, magnets as implants, exoskeletons, and a host of other enhancement technologies, the human body is becoming more mechanical and computational and thus less biological. This trend will continue to accelerate as the body becomes transformed into an information processing technology, which ultimately will challenge one’s sense of identity and what it means to be human. This paper reviews “cyborg enhancement technologies”, with an emphasis placed on technological enhancements to the brain and the creation of new senses—the benefits of which may allow information to be directly implanted into the brain, memories to be edited, wireless brain-to-brain (i.e., thought-to-thought) communication, and a broad range of sensory information to be explored and experienced. -

Bayesian Inference for Biophysical Neuron Models Enables Stimulus
RESEARCH ARTICLE Bayesian inference for biophysical neuron models enables stimulus optimization for retinal neuroprosthetics Jonathan Oesterle1, Christian Behrens1, Cornelius Schro¨ der1, Thoralf Hermann2, Thomas Euler1,3,4, Katrin Franke1,4, Robert G Smith5, Gu¨ nther Zeck2, Philipp Berens1,3,4,6* 1Institute for Ophthalmic Research, University of Tu¨ bingen, Tu¨ bingen, Germany; 2Naturwissenschaftliches und Medizinisches Institut an der Universita¨ t Tu¨ bingen, Reutlingen, Germany; 3Center for Integrative Neuroscience, University of Tu¨ bingen, Tu¨ bingen, Germany; 4Bernstein Center for Computational Neuroscience, University of Tu¨ bingen, Tu¨ bingen, Germany; 5Department of Neuroscience, University of Pennsylvania, Philadelphia, United States; 6Institute for Bioinformatics and Medical Informatics, University of Tu¨ bingen, Tu¨ bingen, Germany Abstract While multicompartment models have long been used to study the biophysics of neurons, it is still challenging to infer the parameters of such models from data including uncertainty estimates. Here, we performed Bayesian inference for the parameters of detailed neuron models of a photoreceptor and an OFF- and an ON-cone bipolar cell from the mouse retina based on two-photon imaging data. We obtained multivariate posterior distributions specifying plausible parameter ranges consistent with the data and allowing to identify parameters poorly constrained by the data. To demonstrate the potential of such mechanistic data-driven neuron models, we created a simulation environment for external electrical stimulation of the retina and optimized stimulus waveforms to target OFF- and ON-cone bipolar cells, a current major problem of retinal neuroprosthetics. *For correspondence: [email protected] Competing interests: The Introduction authors declare that no Mechanistic models have been extensively used to study the biophysics underlying information proc- competing interests exist.