Mamoni FY12 Semi Annual Report Apr 30 2012
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Why Is Rema-Kalenga Wildlife Sanctuary Important? How Can You Help?
WHY IS REMA-KALENGA WILDLIFE SANCTUARY IMPORTANT? Photo: Samiul Mohsanin Rema-Kalenga Wildlife Sanctuary (RKWS) was established in 1982 and later expanded in 1996 to 1,795 hectares. This Sanctuary is located 130 km north-east Protecting forest in Rema-Kalenga of Dhaka, in Chunarughat Upazila, in Habiganj District. It is most easily accessed from Srimangal town, and its Wildlife Sanctuary stores 370 tons of eastern boundary is the border with Tripura State of India. CO2 per hectare for climate change The remote and reasonably intact tropical forests of mitigation Rema-Kalenga make it of high biodiversity value. Notable mammals include threatened primates (Bengal Slow Loris, Assamese Macaque, Northern Pig tailed Macaque, Over 600 species of plants, including HOW CAN YOU HELP? Phayre’s Leaf Monkey and Capped Langur), endangered 92 of 108 nationally red listed Fishing Cat, and nationally rare Black Giant Squirrel. Sadly Please support our efforts to strengthen Leopard and Royal Bengal Tiger are no longer present, species conservation. The work of Rema-Kalenga CMC and but were hunted here into the 1960s. In addition to a wide associated organizations involves local communities diversity of forest birds, Rema-Kalenga holds a breeding High vertebrate diversity, working with local government and Bangladesh colony of the critically endangered White-rumped Vulture, Forest Department. These activities depend on whose populations have been decimated since the late including 196 bird and 20 support from grants and outside resources. 1990s. The Forest Department has designated a large mammal species Rema-Kalenga CMC has a bank account. A/C area around and including RKWS as a “vulture safe zone”, no- 1024901018977, Pubali Bank, Chunarghat, and local communities are supporting the ban on lethal Hobiganj and can receive grants from domestic veterinary drugs. -

Mamoni Newsletter Issue 8, Jan-Mar 2017
MaMoni Health Systems Strengthening Project Issue 08 January- March Newsletter 2017 Community Skilled Birth Attendant (CSBA) e-register rolled out in Madhabpur Photo: Save the Children/Bashir Ahmed Save Photo: aMoni HSS project is collaborating with Measure Evaluation, icddrb and SIAP project to introduce electronic ManagementM Information System (eMIS) in Habiganj district. Recent months saw CSBA module (e-register) rolled out and incorporation of GIS map into the monitoring tool. Data from UH&FWC facility assessment has been integrated with the service statistics allowing presentation of multiple information in a logically segregated way. CSBA module has been rolled out in Madhabpur Upazila of Habiganj and Basail Upazila of Tangail. Training on General Patient, Family Planning and PAC e-registers were organized in all upazilas of Habiganj except Madhabpur, where all the service modules have already been rolled out. The reference document and manual for the e-registers have been developed and practiced during the training sessions. Simultaneously FWA e-register was introduced throughout Habiganj. aMoni HSS Project shared program experiences at the Community Health Workers’ Symposium held from 21st to 23rd FebruaryM 2017 in Kampala, Uganda. The symposium titled "Contribution of Community Health Workers (CHWs) toward Earlier all the DGFP CSBAs of Madhabpur, 13 in total, had received training on MNC e-register and started working on it. Again attainment of the Sustainable Development Goals (SDGs)" was organised by the School of Social Sciences Public Health team around 400 HAs and FWAs were trained on PRS application who have been collecting population data since. In Madhabpur, at Nottingham Trent University (NTU), Makerere University School of Public Health (MakSPH) and the Ugandan Ministry of some 92% of the population have been registered and given away Health ID cards. -

Evaluating the Reaching Out-Of-School Children Project in Bangladesh: a Baseline Study
EVALUATING THE REACHING OUT-OF-SCHOOL CHILDREN PROJECT IN BANGLADESH: A BASELINE STUDY Akhter U. Ahmed Submitted to the World Bank By the International Food Policy Research Institute 2033 K Street, N.W., Washington, D.C. 20006, U.S.A. In collaboration with the Data Analysis and Technical Assistance Limited 8/4 Block A, Lalmatia, Dhaka 1207, Bangladesh November 2006 In memory of Miss Salma Begum (field researcher), Mrs. Shandya Rani Ghosh (field researcher), and Mr. Mizanur Rahman (survey supervisor) who died in a tragic road accident on their way to a field-site to carry out surveys for this study i ACRONYMS AND ABBREVIATIONS CMC Center Management Committee DPE Directorate of Primary Education EFA Education for All ESP Education Service Provider ERP Education Resource Provider FFE Food for Education GER Gross Enrollment Rate GoB Government of Bangladesh GR Gratuitous Relief HSC Higher Secondary Certificate IFPRI International Food Policy Research Institute LC Learning Center LFP Labor Force Participation MoPME Ministry of Primary and Mass Education NER Net Enrollment Rate PD Project Director PEDPII Second Primary Education Development Program PESP Primary Education Stipend Program PKSF Palli Karma Sahayak Foundation PPS Probability Proportional to Size PTI Primary Training Institute ROSC Reaching Out-of-School Children SDC Swiss Agency for Development and Cooperation SFP School Feeding Program SKT Shishu Kallyan Trust SSC Secondary School Certificate TR Test Relief UEO Upazila Education Officer VGD Vulnerable Group Development VGF Vulnerable -
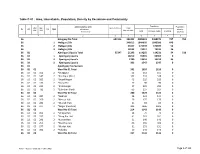
Table C-01 : Area, Households, Population, Density by Residence and Community
Table C-01 : Area, Households, Population, Density by Residence and Community Administrative Unit Population Population UN / MZ / Area in Acres Total ZL UZ Vill RMO Residence density WA MH Households Community Total In Households Floating [sq. km] 1 2 3 4 5 6 7 8 36 Habiganj Zila Total 651516 393302 2089001 2088274 727 792 36 1 Habiganj Zila 346612 1844035 1843386 649 36 2 Habiganj Zila 33157 171749 171697 52 36 3 Habiganj Zila 13533 73217 73191 26 36 02 Ajmiriganj Upazila Total 55347 21293 114265 114231 34 510 36 02 1 Ajmiriganj Upazila 18210 99365 99365 0 36 02 2 Ajmiriganj Upazila 2780 13353 13319 34 36 02 3 Ajmiriganj Upazila 303 1547 1547 0 36 02 Ajmiriganj Paurashava 36 02 01 Ward No-01 Total 341 1610 1610 0 36 02 01 103 2 *Durgapur 52 151 151 0 36 02 01 147 2 *Fatehpur (Part) 102 518 518 0 36 02 01 169 2 *Gupal Nagar 43 229 229 0 36 02 01 173 2 *Gusai Pur 27 90 90 0 36 02 01 235 2 *Krisnanagar 57 295 295 0 36 02 01 733 2 *Sukribari (Part) 60 327 327 0 36 02 02 Ward No-02 Total 280 1424 1424 0 36 02 02 087 2 *Debhati 25 121 121 0 36 02 02 260 2 *Mesuri Hati 29 175 175 0 36 02 02 281 2 *Munshi Hati 21 83 83 0 36 02 02 377 2 *Nogar (Paschim) 205 1045 1045 0 36 02 03 Ward No-03 Total 214 1143 1143 0 36 02 03 093 2 *Dhupa Hati 16 79 79 0 36 02 03 157 2 *Gang Par Hati 41 261 261 0 36 02 03 241 2 *Kumar Hati 31 140 140 0 36 02 03 253 2 *Maidha Para 66 369 369 0 36 02 03 277 2 *Mudak Hati 31 151 151 0 36 02 03 383 2 *Fokabaj 29 143 143 0 36 02 04 Ward No-04 Total 237 1133 1133 0 RMO: 1 = Rural, 2 = Urban and 3 = Other Urban Page 1 of 103 Table C-01 : Area, Households, Population, Density by Residence and Community Administrative Unit Population Population UN / MZ / Area in Acres Total ZL UZ Vill RMO Residence density WA MH Households Community Total In Households Floating [sq. -

Mamoni Health Systems Strengthening Activity
MaMoni Health Systems Strengthening Activity Quarterly Report January 1 – March 31, 2015 Submitted May 15, 2015 This document is made possible by the generous support of the American people through the support of the Office of Population, Health, Nutrition and Education, United States Agency for International Development, Bangladesh (USAID/Bangladesh) under the terms of Associate Cooperative Agreement No. AID-388-LA-13-00004 through MCHIP, managed by Jhpiego Corporation. The contents of this document are the responsibility of Jhpiego Corporation and do not necessarily reflect the views of USAID or the United States Government. Cover Photo Credit: Using a computer tablet, MaMoni HSS data collectors enter population information into a national registry system in Madhabpur Upazila, where the Routine Health Information System (RHIS) project is being piloted. Directorate General Health Services and Directorate General Family Planning service providers will use this electronic information to track clients and ensure services to the families. Photo Credit: Shimantik/Save the Children. MaMoni HSS – Year Two Second Quarterly Report April 2015 2 TABLE OF CONTENTS 1. Introduction ...................................................................................................................................7 2. Program Objectives and Key Activities ............................................................................................8 3. Results for Year 1 ........................................................................................................................ -

Bangladesh: Human Rights Report 2015
BANGLADESH: HUMAN RIGHTS REPORT 2015 Odhikar Report 1 Contents Odhikar Report .................................................................................................................................. 1 EXECUTIVE SUMMARY ............................................................................................................... 4 Detailed Report ............................................................................................................................... 12 A. Political Situation ....................................................................................................................... 13 On average, 16 persons were killed in political violence every month .......................................... 13 Examples of political violence ..................................................................................................... 14 B. Elections ..................................................................................................................................... 17 City Corporation Elections 2015 .................................................................................................. 17 By-election in Dohar Upazila ....................................................................................................... 18 Municipality Elections 2015 ........................................................................................................ 18 Pre-election violence .................................................................................................................. -

Zila Report : Habiganj
POPULATION & HOUSING CENSUS 2011 ZILA REPORT : HABIGANJ Bangladesh Bureau of Statistics Statistics and Informatics Division Ministry of Planning BANGLADESH POPULATION AND HOUSING CENSUS 2011 Zila Report: HABIGANJ October 2015 BANGLADESH BUREAU OF STATISTICS (BBS) STATISTICS AND INFORMATICS DIVISION (SID) MINISTRY OF PLANNING GOVERNMENT OF THE PEOPLE’S REPUBLIC OF BANGLADESH ISBN-978-984-33-8637-3 COMPLIMENTARY Published by Bangladesh Bureau of Statistics (BBS) Statistics and Informatics Division (SID) Ministry of Planning Website: www.bbs.gov.bd This book or any portion thereof cannot be copied, microfilmed or reproduced for any commercial purpose. Data therein can, however, be used and published with acknowledgement of their sources. Contents Page Message of Honorable Minister, Ministry of Planning …………………………………………….. vii Message of Honorable State Minister, Ministry of Finance and Ministry of Planning …………. ix Foreword ……………………………………………………………………………………………….. xi Preface …………………………………………………………………………………………………. xiii Zila at a Glance ………………………………………………………………………………………... xv Physical Features ……………………………………………………………………………………... xix Zila Map ………………………………………………………………………………………………… xx Geo-code ………………………………………………………………………………………………. xxi Chapter-1: Introductory Notes on Census ………………………………………………………….. 1 1.1 Introduction ………………………………………………………………………………… 1 1.2 Census and its periodicity ………………………………………………………………... 1 1.3 Objectives ………………………………………………………………………………….. 1 1.4 Census Phases …………………………………………………………………………… 2 1.5 Census Planning …………………………………………………………………………. -

Mamoni Health Systems Strengthening Activity (USAID Cooperative Agreement AID-388-LA-13-00004)
MaMoni Health Systems Strengthening Activity (USAID Cooperative Agreement AID-388-LA-13-00004) Quarterly Report January 01, 2018– March 31, 2018 Submitted April 30, 2018 Cover Photo Story: Nijhum Dwip looks forward to a healthy future “I would deliver at home as I did before”, Shaheena said when she was asked what she would do if the health center were not there. Shaheena had her second baby delivered at the Nijhum Dwip (a remote island in Hatiya upazila on the south of Bangladesh) Union Health and Family Welfare Centre (UH&FWC) on the day the facility started functioning. For Shaheena, delivering at a health facility was hardly an option before. Shaheena lives in a village in Nijhum Dwip. The nearest health facility from Nijhum Dwip was in Jahajmara union which was hard-to-reach and expensive, would take at least 2-3 hours journey by engine boat and rikshaw van. For about 30,000 people who call Nijhum Dwip their home, ‘delivery at home’ had therefore been the only option. On November 1, 2017, the remote island got its first health center equipped with sufficient essentials to provide a range of basic healthcare services including normal delivery services. Six weeks later, the Nijhum Dwip UH&FWC started providing 24/7 normal delivery services to the community. Now the people of Nijhum Dwip, one of the hardest-to-reach areas in Bangladesh, have the option to avail normal delivery services by skilled birth attendants around-the-clock and free of cost. The establishment of the Nijhum Dwip UH&FWC represents a novel initiative undertaken by the district family planning department and local government with MaMoni HSS project playing the facilitation role. -

Mamoni Integrated Safe Motherhood, Newborn Care, Family Planning Project
MaMoni Integrated Safe Motherhood, Newborn Care, Family Planning Project Dilara Begum of Turong village, Companiganj, Sylhet, gave birth to a baby girl in 2010 who did not move or breathe. The village doctor declared her dead. Thanks to MaMoni’s health promotion activities through community health workers, the local traditional birth attendant was able to revive this beautiful girl, Takmina Begum, who will turn four early next year. Annual Report October 1, 2012‐September 30, 2013 Submitted November 8, 2013 MaMoni FY13 Annual Report Submitted November 8, 2013 Page 1 List of Abbreviations ACCESS Access to Clinical and Community Maternal, Neonatal and Women’s Health Services ANC Antenatal Care A&T Alive and Thrive CAG Community Action Group CC Community Clinic CG/CCMG Community Group/Community Clinic Management Group CHW Community Health Workers CM Community Mobilization/Community Mobilizer CPR Contraceptive Prevalence Rate CS Civil Surgeon CSBA Community Skilled Birth Attendant CV Community Volunteer DDFP Deputy Director, Family Planning DGFP Directorate General of Family Planning DGHS Directorate General of Health Services ELCO Eligible Couple (for FP) EmOC Emergency Obstetric Care ENA Essential Nutrition Action ENC Essential Newborn Care ETAT Emergency Triage, Assessment and Treatment of Sick Newborn FIVDB Friends in Village Development, Bangladesh FPI Family Planning Inspector FWA Family Welfare Assistant FWV Family Welfare Visitor GOB Government of Bangladesh HA Health Assistant ICDDR,B International Centre for Diarrhoeal Diseases -

Mamoni FY'12 Annual Report Oct 2011-Sep 2012
MaMoni Integrated Safe Motherhood, Newborn Care and Family Planning Project Sr. Secretary, MOH&FW, Md. Humayun Kabir, learning how expecting mothers are mapped and tracked in Shibpasha union of Ajmiriganj, Habiganj district. “…The contribution USAID supported MaMoni has made in providing service in this remote and hard-to-reach area is imitable. Particularly, the initiative to increase institutional delivery here is very encouraging…”, he wrote. Annual Report October 1, 2011 – September 30, 2012 Submitted October 31, 2012 MaMoni FY’12 Annual Report | October 31, 2012 0 List of Abbreviations ACCESS Access to Clinical and Community Maternal, Neonatal and Women’s Health Services ACPR Associates for Community Population Research AED Academy for Educational Development A&T Alive and Thrive CAG Community Action Group CC Community Clinic CCMG Community Clinic Management Group CHW Community Health Workers CM Community MobiliZation/Community MobiliZer CS Civil Surgeon CSM Community Supervisor/MobiliZer DDFP Deputy Director, Family Planning DGFP Directorate General of Family Planning DGHS Directorate General of Health Services EmOC Emergency Obstetric Care ENC Essential Newborn Care FIVDB Friends in Village Development, Bangladesh FPI Family Planning Inspectors FWA Family Welfare Assistant FWV Family Welfare Visitors GOB Government of Bangladesh ICDDR,B International Centre for Diarrhoeal Diseases Research, Bangladesh IYCF Infant and Young Child Feeding IMCI Integrated Management of Childhood Illnesses MCH Maternal and child health MCHIP Maternal and Child Health Integrated Program MNH Maternal and newborn health MOH&FW Ministry of Health and Family Welfare MWRA Married Women of Reproductive Age PHC Primary Health Care PNC Postnatal Care SBA Skilled Birth Attendant SMC Social Marketing Company SSFP Smiling Sun Franchise Project TBA Traditional birth attendant UPHCP Urban Primary Health Care Project WRA White Ribbon Alliance MaMoni FY’12 Annual Report | October 31, 2012 1 TABLE OF CONTENTS A. -

List of Upazilas of Bangladesh
List Of Upazilas of Bangladesh : Division District Upazila Rajshahi Division Joypurhat District Akkelpur Upazila Rajshahi Division Joypurhat District Joypurhat Sadar Upazila Rajshahi Division Joypurhat District Kalai Upazila Rajshahi Division Joypurhat District Khetlal Upazila Rajshahi Division Joypurhat District Panchbibi Upazila Rajshahi Division Bogra District Adamdighi Upazila Rajshahi Division Bogra District Bogra Sadar Upazila Rajshahi Division Bogra District Dhunat Upazila Rajshahi Division Bogra District Dhupchanchia Upazila Rajshahi Division Bogra District Gabtali Upazila Rajshahi Division Bogra District Kahaloo Upazila Rajshahi Division Bogra District Nandigram Upazila Rajshahi Division Bogra District Sariakandi Upazila Rajshahi Division Bogra District Shajahanpur Upazila Rajshahi Division Bogra District Sherpur Upazila Rajshahi Division Bogra District Shibganj Upazila Rajshahi Division Bogra District Sonatola Upazila Rajshahi Division Naogaon District Atrai Upazila Rajshahi Division Naogaon District Badalgachhi Upazila Rajshahi Division Naogaon District Manda Upazila Rajshahi Division Naogaon District Dhamoirhat Upazila Rajshahi Division Naogaon District Mohadevpur Upazila Rajshahi Division Naogaon District Naogaon Sadar Upazila Rajshahi Division Naogaon District Niamatpur Upazila Rajshahi Division Naogaon District Patnitala Upazila Rajshahi Division Naogaon District Porsha Upazila Rajshahi Division Naogaon District Raninagar Upazila Rajshahi Division Naogaon District Sapahar Upazila Rajshahi Division Natore District Bagatipara -

Inventory of LGED Road Network, March 2005, Bangladesh
The Chief Engineer Local Government Engineering Department PREFACE It is a matter of satisfaction that LGED Road Database has been published through compilation of data that represent all relevant information of rural road network of the country in a structured manner. The Rural Infrastructure Maintenance Management Unit of LGED (former Rural Infrastructure Maintenance Cell) took up the initiative to create a road inventory database in mid nineties to register all of its road assets country-wide with the help of customized software called, Road and Structure Database Management System. The said database was designed to accommodate all relevant information on the road network sequentially and the system was upgraded from time to time to cater the growing needs. In general, the purpose of this database is to use it in planning and management of LGED's rural road network by providing detailed information on roads and structures. In particular, from maintenance point of view this helps to draw up comprehensive maintenance program including rational allocation of fund based on various parameters and physical condition of the road network. According to recent road re-classification, LGED is responsible for construction, development and maintenance of three classes of roads, which has been named as Upazila Road, Union Road and Village Road (category A & B) in association with Local Government Institution. The basic information about these roads like, road name, road type, length, surface type, condition, structure number with span, existing gaps with length, etc. has been made available in the road inventory. Side by side, corresponding spatial data are also provided in the road map comprising this document.