Bilateral Greater Occipital Nerve Block for Headache After Corrective Spinal Surgery: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vertebral Column and Thorax
Introduction to Human Osteology Chapter 4: Vertebral Column and Thorax Roberta Hall Kenneth Beals Holm Neumann Georg Neumann Gwyn Madden Revised in 1978, 1984, and 2008 The Vertebral Column and Thorax Sternum Manubrium – bone that is trapezoidal in shape, makes up the superior aspect of the sternum. Jugular notch – concave notches on either side of the superior aspect of the manubrium, for articulation with the clavicles. Corpus or body – flat, rectangular bone making up the major portion of the sternum. The lateral aspects contain the notches for the true ribs, called the costal notches. Xiphoid process – variably shaped bone found at the inferior aspect of the corpus. Process may fuse late in life to the corpus. Clavicle Sternal end – rounded end, articulates with manubrium. Acromial end – flat end, articulates with scapula. Conoid tuberosity – muscle attachment located on the inferior aspect of the shaft, pointing posteriorly. Ribs Scapulae Head Ventral surface Neck Dorsal surface Tubercle Spine Shaft Coracoid process Costal groove Acromion Glenoid fossa Axillary margin Medial angle Vertebral margin Manubrium. Left anterior aspect, right posterior aspect. Sternum and Xyphoid Process. Left anterior aspect, right posterior aspect. Clavicle. Left side. Top superior and bottom inferior. First Rib. Left superior and right inferior. Second Rib. Left inferior and right superior. Typical Rib. Left inferior and right superior. Eleventh Rib. Left posterior view and left superior view. Twelfth Rib. Top shows anterior view and bottom shows posterior view. Scapula. Left side. Top anterior and bottom posterior. Scapula. Top lateral and bottom superior. Clavicle Sternum Scapula Ribs Vertebrae Body - Development of the vertebrae can be used in aging of individuals. -

Skeletal System? Skeletal System Chapters 6 & 7 Skeletal System = Bones, Joints, Cartilages, Ligaments
Warm-Up Activity • Fill in the names of the bones in the skeleton diagram. Warm-Up 1. What are the 4 types of bones? Give an example of each. 2. Give 3 ways you can tell a female skeleton from a male skeleton. 3. What hormones are involved in the skeletal system? Skeletal System Chapters 6 & 7 Skeletal System = bones, joints, cartilages, ligaments • Axial skeleton: long axis (skull, vertebral column, rib cage) • Appendicular skeleton: limbs and girdles Appendicular Axial Skeleton Skeleton • Cranium (skull) • Clavicle (collarbone) • Mandible (jaw) • Scapula (shoulder blade) • Vertebral column (spine) • Coxal (pelvic girdle) ▫ Cervical vertebrae • Humerus (arm) ▫ Thoracic vertebrae • Radius, ulna (forearm) ▫ Lumbar vertebrae • Carpals (wrist) • Metacarpals (hand) ▫ Sacrum • Phalanges (fingers, toes) ▫ Coccyx • Femur (thigh) • Sternum (breastbone) • Tibia, fibula (leg) • Ribs • Tarsal, metatarsals (foot) • Calcaneus (heel) • Patella (knee) Functions of the Bones • Support body and cradle soft organs • Protect vital organs • Movement: muscles move bones • Storage of minerals (calcium, phosphorus) & growth factors • Blood cell formation in bone marrow • Triglyceride (fat) storage Classification of Bones 1. Long bones ▫ Longer than they are wide (eg. femur, metacarpels) 2. Short bones ▫ Cube-shaped bones (eg. wrist and ankle) ▫ Sesamoid bones (within tendons – eg. patella) 3. Flat bones ▫ Thin, flat, slightly curved (eg. sternum, skull) 4. Irregular bones ▫ Complicated shapes (eg. vertebrae, hips) Figure 6.2 • Adult = 206 bones • Types of bone -

Anatomical Study of the Superior Cluneal Nerve and Its Estimation of Prevalence As a Cause of Lower Back Pain in a South African Population
Anatomical study of the superior cluneal nerve and its estimation of prevalence as a cause of lower back pain in a South African population by Leigh-Anne Loubser (10150804) Dissertation to be submitted in full fulfilment of the requirements for the degree Master of Science in Anatomy In the Faculty of Health Science University of Pretoria Supervisor: Prof AN Van Schoor1 Co-supervisor: Dr RP Raath2 1 Department of Anatomy, University of Pretoria 2 Netcare Jakaranda Hospital, Pretoria 2017 DECLARATION OF ORIGINALITY UNIVERSITY OF PRETORIA The Department of Anatomy places great emphasis upon integrity and ethical conduct in the preparation of all written work submitted for academic evaluation. While academic staff teach you about referencing techniques and how to avoid plagiarism, you too have a responsibility in this regard. If you are at any stage uncertain as to what is required, you should speak to your lecturer before any written work is submitted. You are guilty of plagiarism if you copy something from another author’s work (e.g. a book, an article, or a website) without acknowledging the source and pass it off as your own. In effect, you are stealing something that belongs to someone else. This is not only the case when you copy work word-for-word (verbatim), but also when you submit someone else’s work in a slightly altered form (paraphrase) or use a line of argument without acknowledging it. You are not allowed to use work previously produced by another student. You are also not allowed to let anybody copy your work with the intention of passing if off as his/her work. -

Required List of Bones and Markings
REQUIRED LIST OF BONES AND MARKINGS Axial Skeleton Skull Cranial Bones (8) Frontal Bone (1) Supraorbital foramina Supraorbital ridges or margins Parietal Bones (2) Temporal Bones (2) External auditory meatus Mastoid process Styloid process Zygomatic process Mandibular fossa Foramen lacerum Carotid foramen Jugular foramen Stylomastoid foramen Internal auditory meatus Occipital Bone (1) Foramen magnum Occipital condyles Ethmoid Bone (1) Cribriform plate Olfactory foramina in cribriform plate Crista galli Perpendicular plate (forms superior part of nasal septum) Middle nasal concha Superior nasal concha Sphenoid Bone (1) Foramen ovale Foramen rotundum Sella turcica Greater wing Lesser wing Optic foramen Inferior orbital fissure Superior orbital fissure Pterygoid processes Skull (cont’d) Facial Bones (14) Lacrimal Bones (2) Lacrimal fossa Nasal Bones (2) Inferior Nasal Conchae (2) Vomer (1) (forms inferior portion of nasal septum) Zygomatic Bones (2) Temporal process (forms zygomatic arch with zygomatic process of temporal bone) Maxillae (2) Alveoli Palatine process (forms anterior part of hard palate) Palatine Bones (2) (form posterior part of hard palate) Mandible (1) Alveoli Body Mental foramen Ramus Condylar process (mandibular condyle) Coronoid process Miscellaneous (Skull) Paranasal sinuses are located in the ethmoid bone, sphenoid bone, frontal bone, and maxillae Zygomatic arch (“cheekbone”) is composed of the zygomatic process of the temporal bone and the temporal process of the zygomatic bone 2 pairs of nasal conchae (superior and middle) are part of the ethmoid bone. 1 pair (inferior) are separate facial bones. All the scroll-like conchae project into the lateral walls of the nasal cavity. Hard palate (“roof of mouth”) is composed of 2 palatine processes of the maxillae and the 2 palatine bones (total of 4 fused bones). -

Lumbarisation of the First Sacral Vertebra a Rare Form of Lumbosacral Transitional Vertebra
Int. J. Morphol., 33(1):48-50, 2015. Lumbarisation of the First Sacral Vertebra a Rare Form of Lumbosacral Transitional Vertebra Lumbarización de la Primera Vertebra Sacra: Rara Forma de Una Vertebra de Transición Lumbosacral Mallikarjun Adibatti* & Asha, K.** ADIBATTI, M. & ASHA, K. Lumbarisation of the first sacral vertebra a rare form of lumbosacral transitional vertebra. Int. J. Morphol., 33(1):48-50, 2015. SUMMARY: In the lumbosacral region, anatomical variations occur with changes in the number of sacral vertebra either by deletion of first sacral vertebra or by the union of fifth lumbar or first coccygeal vertebra with sacrum. Lumbasacral transitional vertebrae (LSTV) is the most common congenital anomalies of the lumbosacral region. It most commonly involves the fifth lumbar vertebra showing signs of fusion to the sacrum known as sacralisation or the first sacral vertebra shows signs of transition to a lumbar configuration commonly known as lumbarisation. Complete transition can result in numerical abnormalities of the lumbar and sacral vertebral segments. Lumbarisation of first sacral vertebra is seen with a very low incidence of 2%. Knowledge of presence of such vertebral variation will be helpful for the clinicians to diagnose and treat patients with low back pain. Although sacralisation of fifth lumbar vertebrae is most commonly seen when compared to lumbarisation of first sacral vertebrae, we report here a case of lumbarisation of first sacral vertebrae for its rarity among the LSTV and clinical implications. KEY WORDS: Vertebrae; Sacrum; Sacralisation; Lumbarisation; Transitional vertebrae. INTRODUCTION RESULTS The sacrum is formed by the fusion of five sacral During routine Osteology classes, we observed the vertebras. -

Chapter 02: Netter's Clinical Anatomy, 2Nd Edition
Hansen: Netter's Clinical Anatomy, 2nd Edition - with Online Access 2 BACK 1. INTRODUCTION 4. MUSCLES OF THE BACK REVIEW QUESTIONS 2. SURFACE ANATOMY 5. SPINAL CORD 3. VERTEBRAL COLUMN 6. EMBRYOLOGY FINAL 1. INTRODUCTION ELSEVIERl VertebraeNOT prominens: the spinous process of the C7- vertebra, usually the most prominent The back forms the axis (central line) of the human process in the midline at the posterior base of body and consists of the vertebral column, spinal cord, the neck supporting muscles, and associated tissues (skin, OFcon- l Scapula: part of the pectoral girdle that sup- nective tissues, vasculature, and nerves). A hallmark of ports the upper limb; note its spine, inferior human anatomy is the concept of “segmentation,” and angle, and medial border the back is a prime example. Segmentation and bilat l Iliac crests: felt best when you place your eral symmetry of the back will be obvious as you hands “on your hips”; an imaginary horizontal study the vertebral column, the distribution of the line connecting the crests passes through the spinal nerves, the muscles of th back, and its vascular spinous process of the L4 vertebra and the supply. intervertebral disc of L4-L5, a useful landmark Functionally, the back is involved in three primary for a lumbar puncture or epidural block tasks: l Posterior superior iliac spines: an imaginary CONTENThorizontal line connecting these two points l Support: the vertebral column forms the axis of passes through the spinous process of S2 (second the body and is critical for our upright posture sacral segment) (standing or si ting), as a support for our head, as an PROPERTYattachment point and brace for move- 3. -

Vertebral Column
Vertebral Column • Backbone consists of Cervical 26 vertebrae. • Five vertebral regions – Cervical vertebrae (7) Thoracic in the neck. – Thoracic vertebrae (12) in the thorax. – Lumbar vertebrae (5) in the lower back. Lumbar – Sacrum (5, fused). – Coccyx (4, fused). Sacrum Coccyx Scoliosis Lordosis Kyphosis Atlas (C1) Posterior tubercle Vertebral foramen Tubercle for transverse ligament Superior articular facet Transverse Transverse process foramen Facet for dens Anterior tubercle • Atlas- ring of bone, superior facets for occipital condyles. – Nodding movement signifies “yes”. Axis (C2) Spinous process Lamina Vertebral foramen Transverse foramen Transverse process Superior articular facet Odontoid process (dens) •Axis- dens or odontoid process is body of atlas. – Pivotal movement signifies “no”. Typical Cervical Vertebra (C3-C7) • Smaller bodies • Larger spinal canal • Transverse processes –Shorter – Transverse foramen for vertebral artery • Spinous processes of C2 to C6 often bifid • 1st and 2nd cervical vertebrae are unique – Atlas & axis Typical Cervical Vertebra Spinous process (bifid) Lamina Vertebral foramen Inferior articular process Superior articular process Transverse foramen Pedicle Transverse process Body Thoracic Vertebrae (T1-T12) • Larger and stronger bodies • Longer transverse & spinous processes • Demifacets on body for head of rib • Facets on transverse processes (T1-T10) for tubercle of rib Thoracic Vertebra- superior view Spinous process Transverse process Facet for tubercle of rib Lamina Superior articular process -
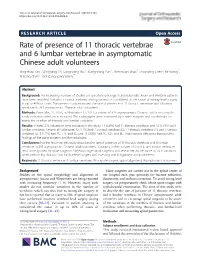
Rate of Presence of 11 Thoracic Vertebrae and 6 Lumbar Vertebrae In
Yan et al. Journal of Orthopaedic Surgery and Research (2018) 13:124 https://doi.org/10.1186/s13018-018-0835-9 RESEARCHARTICLE Open Access Rate of presence of 11 thoracic vertebrae and 6 lumbar vertebrae in asymptomatic Chinese adult volunteers Ying-zhao Yan1, Qing-ping Li2, Cong-cong Wu1, Xiang-xiang Pan1, Zhen-xuan Shao1, Shao-qing Chen2, Ke Wang1, Xi-bang Chen1 and Xiang-yang Wang1* Abstract Background: An increasing number of studies on spinal morphology in asymptomatic Asian and Western patients have been reported. Variation in spinal anatomy among patients is considered as the cause of wrong-level surgery in up to 40% of cases. The present study examined the rate of presence of 11 thoracic vertebrae and 6 lumbar vertebrae in 293 asymptomatic Chinese adult volunteers. Methods: From May 27, 2016, to November 11, 2017, a cohort of 325 asymptomatic Chinese adults meeting the study exclusion criteria was recruited. The radiographs were examined by a spine surgeon and a radiologist to assess the number of thoracic and lumbar vertebrae. Results: In total, 293 volunteers were included in this study: 17 (5.8%) had 11 thoracic vertebrae, and 16 (5.5%) had 6 lumbar vertebrae. Among all volunteers, 12 (4.1%) had 7 cervical vertebrae (C), 11 thoracic vertebrae (T), and 5 lumbar vertebrae (L); 5 (1.7%) had 7C, 11T, and 6L; and 11 (3.8%) had 7C, 12T, and 6L. There was no difference between the findings of the spine surgeon and the radiologist. Conclusions: For the first time, this study describes the rate of presence of 11 thoracic vertebrae and 6 lumbar vertebrae in 293 asymptomatic Chinese adult volunteers. -

Superior Cluneal Neuralgia from Iliocostal Impingement
PAIN ISSN 2575-9841 MEDICINE ©2020, American Society of Interventional Pain Physicians© CASE Volume 4, Number 3, p 77-83p REPORTS Received: 2019-07-29 SUPERIOR CLUNEAL NEURALGIA FROM Accepted: 2019-10-03 Published: 2020-05-29 ILIOCOSTAL IMPINGEMENT TREATED WITH PHENOL NEUROLYSIS: A CASE REPORT Heath B. McAnally, MD1,2 Andrea M. Trescot, MD3 Background: Superior cluneal neuralgia (SCN) is an increasingly recognized yet still frequently overlooked cause of chronic lumbosacral and buttock pain. While historically attributed generally to iatrogenic iliac crest injury (bone marrow biopsy or bone graft harvest), more recently it is recognized as occurring in the absence of any trauma, with idiopathic entrapment resulting in compression neuropathy. Iliocostal impingement syndrome (IIS) is an even less commonly considered condition whereby the lower costal margin repetitively contacts and irritates the iliac crest, primarily occurring unilaterally and owing to severe scoliosis, but also in the context of severe vertebral column height loss. Case Report: We report here a case of an elderly woman with a 3-inch reported height loss over the decades who had suffered with chronic and intractable right lumbosacral and gluteal pain, and whom, on the basis of physical examination, we diagnosed presumptively with both SCN and with IIS as the underlying patho- physiologic mechanism. After undergoing successful diagnostic fluoroscopically guided superior cluneal nerve block, she was offered phenol denervation and enjoyed 9 months of reported 90% improvement in her symptoms, with gradual return to baseline over the next couple months. She has subsequently undergone repeat phenol denervation twice, with similarly good results. We believe this to be the first documented application of phenol neurolytic technique to SCN, and in the case of iliocostal impingement we argue that surgical release/resection or even peripheral nerve stimulation may not be effective owing to underlying compression/irritation diathesis from the inevitable pressure of the costal margin upon the iliac crest. -

Cervical Vertebrae 1 Cervical Vertebrae
Cervical vertebrae 1 Cervical vertebrae Cervical vertebrae or Cervilar Position of human cervical vertebrae (shown in red). It consists of 7 bones, from top to bottom, C1, C2, C3, C4, C5, C6 and C7. A human cervical vertebra Latin Vertebrae cervicales [1] Gray's p.97 [2] MeSH Cervical+vertebrae [3] TA A02.2.02.001 [4] FMA FMA:72063 In vertebrates, cervical vertebrae (singular: vertebra) are those vertebrae immediately inferior to the skull. Thoracic vertebrae in all mammalian species are defined as those vertebrae that also carry a pair of ribs, and lie caudal to the cervical vertebrae. Further caudally follow the lumbar vertebrae, which also belong to the trunk, but do not carry ribs. In reptiles, all trunk vertebrae carry ribs and are called dorsal vertebrae. In many species, though not in mammals, the cervical vertebrae bear ribs. In many other groups, such as lizards and saurischian dinosaurs, the cervical ribs are large; in birds, they are small and completely fused to the vertebrae. The transverse processes of mammals are homologous to the cervical ribs of other amniotes. Cervical vertebrae 2 In humans, cervical vertebrae are the smallest of the true vertebrae, and can be readily distinguished from those of the thoracic or lumbar regions by the presence of a foramen (hole) in each transverse process, through which passes the vertebral artery. The remainder of this article focuses upon human anatomy. Structure By convention, the cervical vertebrae are numbered, with the first one (C1) located closest to the skull and higher numbered vertebrae (C2-C7) proceeding away from the skull and down the spine. -
Bones of the Trunk
BONES OF THE TRUNK Andrea Heinzlmann Veterinary University Department of Anatomy and Histology 16th September 2019 VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) • the vertebral column composed of the vertebrae • the vertebrae form a horizontal chain https://hu.pinterest.com/pin/159877855502035893/ VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) along the vertebral column three major curvatures are recognized: 1. the DORSAL CONVEX CURVATURE – between the head and the neck 2. the DORSAL CONCAVE CURVATURE – between the neck and the chest 3. the DORSAL CONVEX CURVATURE – between the thorax and the lumbar region - in carnivores (Ca) there is an additional DORSAL CONVEXITY in the sacral region https://hu.pinterest.com/pin/159877855502035893/ VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) - corresponding to the regions of the body, we distinguish: 1. CERVICAL VERTEBRAE 2. THORACIC VERTEBRAE 3. LUMBAR VERTEBRAE 4. SACRAL VERTEBRAE 5. CAUDAL (COCCYGEAL) VERTEBRAE https://www.ufaw.org.uk/dogs/french-bulldog-hemivertebrae https://rogueshock.com/know-your-horse-in-9-ways/5/ BUILD OF THE VERTEBRAE each vertebrae presents: 1. BODY (CORPUS VERTEBRAE) 2. ARCH (ARCUS VERTEBRAE) 3. PROCESSES corpus Vertebra thoracica (Th13) , Ca. THE VERTEBRAL BODY (CORPUS VERTEBRAE) - the ventral portion of the vertebra ITS PARTS: 1. EXTREMITAS CRANIALIS (seu CAPUT VERTEBRAE) – convex 2. EXTREMITAS CAUDALIS (seu FOSSA VERTEBRAE) - concave Th13, Ca. THE VERTEBRAL BODY (CORPUS VERTEBRAE) 3. VENTRAL SURFACE of the body has a: - ventral crest (CRISTA VENTRALIS) 4. DORSAL SURFACE of the body carries : - the vertebral arch (ARCUS VERTEBRAE) Th13, Ca., lateral aspect Arcus vertebrae corpus Vertebra thoracica (Th13) , Ca., caudal aspect THE VERTEBRAL BODY (CORPUS VERTEBRAE) 6. VERTEBRAL ARCH (ARCUS VERTEBRAE) compraisis: a) a ventral PEDICULUS ARCUS VERTEBRAE b) a dorsal LAMINA ARCUS VERTEBRAE C7, Ca. -

The Vertebral Column Is 33 Vertebrae Held Together by Ligaments and Muscles, with Intervertebral Discs in Between
The vertebral column is 33 vertebrae held together by ligaments and muscles, with intervertebral discs in between. The vertebral column provides support and upright posture (attenuates loads) for the body. It is also a site for many muscle attachments. There are natural curves in the spine to help with the support and posture, as well as increasing the flexibility of the spine. The 33 vertebrae are divided into 5 sections, with each group having unique features designed for specific purposes. The groups are: cervical (7), thoracic (12), lumbar (5), sacrum (5), and coccyx (4). All vertebrae have a body, 2 transverse processes, a spinous process, superior/inferior articulating facets, lamina, pedicle, and a vertebral foramen. 1 There are anterior convex curves in the cervical and lumbar spines. Posterior concave curves occur in the thoracic and sacral-coccygeal spines. The curves of the spine may increase/decrease as the body’s center of gravity shifts (ex: pregnancy, weight gain/loss, trauma)—this is a result of trying to maintain in the upright position, the brain over the body’s center of gravity. 2 Scoliosis—excessive lateral curvature; side to side Kyphosis—hunchback; excessive curvature of thoracic Lordosis—swayback ; excessive curvature of lumbar 3 C1 and C2 are shaped differently than the other 5 cervical vertebrae to permit the head to rotate. C1 (atlas) = holds up the world (head) and is missing a body; it articulates with the occipital bone as well as rotating around the odontoid process (dens) of the C2 vertebrae (atlantoaxial joint). The atlantoaxial joint is what type of joint?? C2 (axis) = odontoid process projects up C3-C7 = the body is small and all the processes are short and blunted.