Morphology of Right Atrioventricular Valve Annulus and Leaflets in Autopsy Specimens
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pulmonary Valve Guideline
Pulmonary Valve What the Nurse Caring for a Patient with CHD Needs to Know Catherine Baxter, MSN, RN, CPNP-AC Nurse Practitioner, Pediatric Cardiac Surgery, Levine Children’s Hospital, Charlotte, NC Misty Ellis, MSN, CPNP-PC/AC Pediatric Cardiac Intensive Care Nurse Practitioner University of Louisville, Kosair Children’s Hospital Victoria Winter RN, MSN, CNS, CCRN Clinical Nurse IV, Adjunct Professor, Children’s Hospital Los Angeles and Azusa Pacific University School of Nursing Louise Callow, MSN, RN, CPNP Pediatric Cardiac Surgery Nurse Practitioner, University of Michigan, CS Mott Children’s Hospital Mary Rummell, MN, RN, CPNP, CNS, FAHA Clinical Nurse Specialist, Pediatric Cardiology/Cardiac Services, Oregon Health & Science University (Retired) Embryology Occurrence: o Defects of cardiac valves are the most common subtype of cardiac malformations o Account for 25% to 30% of all congenital heart defects o Most costly and relevant CHD o Wide spectrum of congenital defects in pulmonary valve Development of the heart valves occurs during the fourth to eighth weeks of gestation- after tubular heart looping o Walls of the tubular heart consist of an outer lining of myocardium and an inner lining of endocardial cells o Cardiac jelly, extensive extracellular matrix (ECM), separates the two layers o Cardiac jelly expands to form cardiac cushions at the sites of future valves . Outflow track (OT) valves = aortic and pulmonic valves Final valves derived from endothelial-mesenchymal cells with neural crest cells from the brachial arches Valves (Semilunar) have 3 equal cusp-shaped leaflets Aortic valve incorporates coronary arteries . Atrioventricular (AV) valves = mitral and tricuspid Final valves derived entirely from endocardial cushion tissue Leaflet formed without a cusp 1 Two leaflets associated with left ventricle (mitral) Three leaflets associated with right ventricle (tricuspid) Coordinated by complex interplay of: o Genetics o Signaling pathways that regulate cell apoptosis and proliferation o Environmental factors . -

4B. the Heart (Cor) 1
Henry Gray (1821–1865). Anatomy of the Human Body. 1918. 4b. The Heart (Cor) 1 The heart is a hollow muscular organ of a somewhat conical form; it lies between the lungs in the middle mediastinum and is enclosed in the pericardium (Fig. 490). It is placed obliquely in the chest behind the body of the sternum and adjoining parts of the rib cartilages, and projects farther into the left than into the right half of the thoracic cavity, so that about one-third of it is situated on the right and two-thirds on the left of the median plane. Size.—The heart, in the adult, measures about 12 cm. in length, 8 to 9 cm. in breadth at the 2 broadest part, and 6 cm. in thickness. Its weight, in the male, varies from 280 to 340 grams; in the female, from 230 to 280 grams. The heart continues to increase in weight and size up to an advanced period of life; this increase is more marked in men than in women. Component Parts.—As has already been stated (page 497), the heart is subdivided by 3 septa into right and left halves, and a constriction subdivides each half of the organ into two cavities, the upper cavity being called the atrium, the lower the ventricle. The heart therefore consists of four chambers, viz., right and left atria, and right and left ventricles. The division of the heart into four cavities is indicated on its surface by grooves. The atria 4 are separated from the ventricles by the coronary sulcus (auriculoventricular groove); this contains the trunks of the nutrient vessels of the heart, and is deficient in front, where it is crossed by the root of the pulmonary artery. -

Chapter 12 the Cardiovascular System: the Heart Pages
CHAPTER 12 THE CARDIOVASCULAR SYSTEM: THE HEART PAGES 388 - 411 LOCATION & GENERAL FEATURES OF THE HEART TWO CIRCUIT CIRCULATORY SYSTEM DIVISIONS OF THE HEART FOUR CHAMBERS Right Atrium Left Atrium Receives blood from Receives blood from the systemic circuit the pulmonary circuit FOUR CHAMBERS Right Ventricle Left Ventricle Ejects blood into the Ejects blood into the pulmonary circuit systemic circuit FOUR VALVES –ATRIOVENTRICULAR VALVES Right Atrioventricular Left Atrioventricular Valve (AV) Valve (AV) Tricuspid Valve Bicuspid Valve and Mitral Valve FOUR VALVES –SEMILUNAR VALVES Pulmonary valve Aortic Valve Guards entrance to Guards entrance to the pulmonary trunk the aorta FLOW OF BLOOD MAJOR VEINS AND ARTERIES AROUND THE HEART • Arteries carry blood AWAY from the heart • Veins allow blood to VISIT the heart MAJOR VEINS AND ARTERIES ON THE HEART Coronary Circulation – Supplies blood to the muscle tissue of the heart ARTERIES Elastic artery: Large, resilient vessels. pulmonary trunk and aorta Muscular artery: Medium-sized arteries. They distribute blood to skeletal muscles and internal organs. external carotid artery of the neck Arteriole: Smallest of arteries. Lead into capillaries VEINS Large veins: Largest of the veins. Superior and Inferior Vena Cava Medium-sized veins: Medium sized veins. Pulmonary veins Venules: the smallest type of vein. Lead into capillaries CAPILLARIES Exchange of molecules between blood and interstitial fluid. FLOW OF BLOOD THROUGH HEART TISSUES OF THE HEART THE HEART WALL Pericardium Outermost layer Serous membrane Myocardium Middle layer Thick muscle layer Endocardium Inner lining of pumping chambers Continuous with endothelium CARDIAC MUSCLE Depend on oxygen to obtain energy Abundant in mitochondria In contact with several other cardiac muscles Intercalated disks – interlocking membranes of adjacent cells Desmosomes Gap junctions CONNECTIVE TISSUE Wrap around each cardiac muscle cell and tie together adjacent cells. -

Arrhythmia Study Guide – 2 – Sinus and Atrial Rhythms
Arrhythmia Study Guide – 2 – Sinus and Atrial Rhythms Review of Conduction System: SA Node initiates electrical impulses at a rate of 60 – 100 BPM and is the primary pacemaker of the heart. The AV node recieves the impulse from the SA Node through the internodal pathways. The AV Node then delays relay ofthe impulse to the Bundle of His to allow the atria to empty into the ventricles before the ventricular contraction starts. The Bundle of His relays the impulse to the right and left bundle branches. The bundle branches relay to the Purkinje Fibers and the Purkinje Fibers deliver the impulse to the ventricular myocardium to trigger the ventricular contraction. If the SA Node fails to fire, or fires at a much slower rate, the AV node may take over as pacemaker at a rate of 40 - 60 BPM. If the AV Node fails or fires at a much slower rate, the Perkinjie fibers may act as pacemaker at a rate of 20 – 40 BPM. The ECG is a graph of the electrical activity of the heart. Knowing how the heart conducts the electrical impulses provides a strong basis for understanding the ECG strip – and figuring out what is or is not working correctly. SINUS RHYTHMS Rhythms that originate from the SA Node are characterized by upright uniform P-waves followed by a QRS complex. The P-R interval is constant, and the atrial (P-waves) and ventricular (QRS Complex) rhythms are regular. A rate less than 60 is bradycardic, 60 to 100 is normal, over 100 is tachycardic. -

Ventricular Anatomy for the Electrophysiologist (Part
Ventricular Anatomy for the REVIEW Electrophysiologist (Part II) SPECIAL 서울대학교 의과대학 병리학교실 서정욱 이화여자대학교 의학전문대학원 김문영 ABSTRACT The conduction fibers and Purkinje network of the ventricular myocardium have their peculiar location and immuno-histochemical characteristics. The bundle of His is located at the inferior border of the membranous septum, where the single trunk ramifies into the left and right bundle branches. The left bundle branches are clearly visible at the surface. The right bundles are hidden in the septal myocardium and it is not easy to recognize them. The cellular characters of the conduction bundles are modified myocardial cells with less cytoplasmic filaments. Myoglobin is expressed at the contractile part, whereas CD56 is expressed at the intercalated disc. A fine meshwork of synaptophysin positive processes is noted particularly at the nodal tissue. C-kit positive cells are scattered, but their role is not well understood. Purkinje cells are a peripheral continuation of bundles seen at the immediate subendocardium of the left ventricle. Key words: ■ conduction system ■ Purkinje network ■ pathology ■ arrhythmia ■ electrophysiology Introduction human heart. In this brief review, the histological characteristics of conduction cells, stained by The functional assessment of abnormal cardiac conventional and immuno-histochemical staining, are 3 rhythm and a targeted treatment based on demonstrated in the second part of the review. electrophysiologic studies are successful advances in cardiology.1 Morphological assessment or confirmation The characteristic location of the ventricular of hearts with such abnormalities is rare, not only due conduction system to the limited availability of human hearts but also inherent technological limitations of existing The atrioventricular node is situated in its technology.2 Classical morphological approaches and subendocardial location at the triangle of Koch. -

Note: Before Reading the Specific Defect
Pulmonary Valve Stenosis and Regurgitation What is it? The pulmonary valve opens to let blood flow from the right ventricle to the lungs. Narrowing of the pulmonary valve, known as valvular pulmonary stenosis (PS) causes the right ventricle to pump harder to get blood past the blockage. Normally the pulmonary valve has three cusps. If these cusps are malformed, the valve may become narrowed (stenotic) or leaky (regurgitant or insufficiency). Pulmonary valve stenosis is much more common than regurgitation. The stenosis and regurgitation or both can be mild, moderate or severe. What causes it? In most cases, the cause isn’t known. It’s a common type of heart defect. Babies born to mothers who had rubella (German measles) during pregnancy were more likely to develop pulmonary stenosis along with deafness and patent ductus arteriosus. Some patients can have other heart defects along with PS. How does it affect the heart? Normally the right side of the heart pumps blood to the lungs. In a person with PS, the pressure in the right-heart pumping chamber (right ventricle) is much higher than normal and the heart must work harder to pump blood out into the lung arteries. Over time this can cause damage to the overworked heart muscle. When the valve is regurgitant it can cause the right ventricle to enlarge. How does the PS affect me? If the PS is severe, adults may complain of chest pain, exercise intolerance or have no symptoms. Cyanosis is rare and usually occurs only when there is an atrial or ventricular septal defect as well. -

Cardiology Self Learning Package
Cardiology Self Learning Package Module 1: Anatomy and Physiology of the Module 1: Anatomy and Physiology of the Heart Heart. Page 1 Developed by Tony Curran (Clinical Nurse Educator) and Gill Sheppard (Clinical Nurse Specialist) Cardiology (October 2011) CONTENT Introduction…………………………………………………………………………………Page 3 How to use the ECG Self Learning package………………………………………….Page 4 Overview of the Heart…………………………………………………...…………..…….Page 5 Location, Size and Shape of the Heart…………………………………………………Page 5 The Chambers of the Heart…………….………………………………………..……….Page 7 The Circulation System……………………………………….………………..…………Page 8 The Heart Valve Anatomy………………………….…………………………..…………Page 9 Coronary Arteries…………………………………………….……………………..……Page 10 Coronary Veins…………………………………………………………………..……….Page 11 Cardiac Muscle Tissue……………………………………………………………..……Page 12 The Conduction System………………………………………………………………...Page 13 Cardiac Cycle……………………………………………………………………………..Page 15 References…………………………………………………………………………………Page 18 Module Questions………………………………………………………………………..Page 19 Module Evaluation Form………………………………………………………………..Page 22 [Module 1: Anatomy and Physiology of the Heart Page 2 Developed by Tony Curran (Clinical Nurse Educator) and Gill Sheppard (Clinical Nurse Specialist) Cardiology (October 2011) INTRODUCTION Welcome to Module 1: Anatomy and Physiology of the Heart. This self leaning package is designed to as tool to assist nurse in understanding the hearts structure and how the heart works. The goal of this module is to review: Location , size and shape of the heart The chambers of the heart The circulation system of the heart The heart’s valve anatomy Coronary arteries and veins Cardiac muscle tissue The conduction system The cardiac cycle This module will form the foundation of your cardiac knowledge and enable you to understand workings of the heart that will assist you in completing other modules. Learning outcomes form this module are: To state the position of the heart, the size and shape. -

Glossary of Commonly Used Heart and Vascular Terms
Glossary of Commonly Used Terms • Angina: Chest pain that occurs when an area of the heart muscle does not receive enough oxygen-rich blood. • Aorta: The largest artery in the body, it receives blood from the heart that has been oxygenated in the lungs, and delivers this blood to the body and brain. • Aortic Stenosis: A progressive disease that affects the aortic valve of the heart. • Aortic valve: The heart valve that regulates the one-way flow of blood from the left ventricle to the aorta. • Arteries: The blood vessels that carry oxygen-rich blood away from the heart and lungs. • Atria: The two upper chambers of the heart that receive blood returning from the body. • Balloon valvuloplasty: A procedure performed to open a narrowed heart valve using a thin tube called a catheter with a small balloon at its tip. The catheter is inserted through a small incision in the groin and then threaded up to the opening of the narrowed heart valve. The balloon is then inflated to stretch the valve open and relieve valve obstruction. • Bi-leaflet: A valve that has two leaflets that regulate the flow of blood. A normal aortic valve has three leaflets. • Calcification: A disease state in which calcium from the blood collects in the body tissues. When this occurs on the leaflets of the heart’s valves, it may cause them to harden and reduce their ability to open and close properly. • Cardiopulmonary bypass: Bypass of the heart and lungs. During this technique, which is often used during heart surgery, a heart-lung machine temporarily takes over the function of the heart and lungs. -

Redalyc.Conduction System in the Swine Heart: Essential Landmarks
Red de Revistas Científicas de América Latina, el Caribe, España y Portugal Sistema de Información Científica Mingsakul, Thaworn; Surachon, Preeyaporn; Somana, Reon Conduction System in the Swine Heart: Essential Landmarks for Gross Dissection Acta Scientiae Veterinariae, vol. 42, núm. 1, enero, 2014, pp. 1-8 Universidade Federal do Rio Grande do Sul Porto Alegre, Brasil Available in: http://www.redalyc.org/articulo.oa?id=289029240048 Acta Scientiae Veterinariae, ISSN (Printed Version): 1678-0345 [email protected] Universidade Federal do Rio Grande do Sul Brasil How to cite Complete issue More information about this article Journal's homepage www.redalyc.org Non-Profit Academic Project, developed under the Open Acces Initiative Acta Scientiae Veterinariae, 2014. 42: 1211. RESEARCH ARTICLE ISSN 1679-9216 Pub. 1211 Conduction System in the Swine Heart: Essential Landmarks for Gross Dissection Thaworn Mingsakul1, Preeyaporn Surachon1 & Reon Somana2 ABSTRACT Background: The components of the cardiac conduction system (CCS) were discovered almost two centuries and presented in the diagrammatic forms. This should be due to the diffi culty in distinguishing the CCS from the surrounding cardiac tissues and the lack of information concerning the precise landmarks for gross dissection. Furthermore the CCS in pig, the animal regarded as a suitable model for the assessment of catheter based intervention, has not been reported. The aims of the present study were to demonstrate the gross anatomic architecture of CCS in the swine heart, and to provide the valuable landmarks for the gross anatomic dissection of the CCS. Materials, Methods & Results: Twenty hearts of adult Large White pigs (Sus Scrofa domesticus) were used. -

PHV Short.Indd
Anatomy & physiology: The heart Cardiac electrical conductance A Sinoatrial (SA) node D Right bundle branch B Atrioventricular (AV) node E Left bundle branch A C Atrioventricular bundle of His F Purkinje fibres The sinoatrial (SA) node is the heart's natural pacemaker, B containing cells that generate electrical impulses which spread F through the atria, triggering contraction of the atria, forcing blood into the ventricles, and stimulating the atrioventricular A (AV) node. E The AV node is linked with the atrioventricular bundle of His C which transmits impulses to the left and right bundle branches and then to the Purkinje fibres which surround the ventricles. The electrical impulses travel through the Purkinje fibres D causing the ventricles to contract and blood forced out of the heart. F Electrocardiogram (ECG) Heart construction The heart is a muscular, cone-shaped organ located behind The ECG traces the course of the cardiac impulse by the sternum and is approximately the same size as the recording the change in electrical potential on the surface of patient's closed fist. the body. Various parts of the ECG are associated with the travel of electrical impulses though the heart. The heart walls are made up the three structures: the pericardium, myocardium and endocardium. The P wave represents atrial depolarisation which causes the atria to contract. The pericardium is a thick fibrous membrane which surrounds the heart. Its function is to anchor the heart and Q is when the impulses arrive at the atrioventricular (AV) prevents over distension (expanding too much). node. The myocardium is the central layer of the heart and is The QRS complex represents ventricular depolarisation and formed from cardiac muscle tissue, it is this muscle which atrial repolarisation (ventricles contract and atria relax and provides the force which pumps the blood around the body. -

Pulmonary Valve Preservation Strategies for Tetralogy of Fallot Repair Constantine Mavroudis, MD
Pulmonary Valve Preservation Strategies for Tetralogy of Fallot Repair Constantine Mavroudis, MD he optimal repair for tetralogy of Fallot is challenged by techniques and acceptance of high intraoperative right ventri- Tthe management of the small right ventricular outflow cular to left ventricular pressure ratios of 0.7 or less.6-10 tract (RVOT), which was initially solved by John Kirklin who Transannular patches, when necessary, involved a strategy of determined that the absence of the pulmonary valve could transatrial RVOT resection, transatrial VSD closure, and be well tolerated owing to low pulmonary artery pressure limited ventriculotomy, oftentimes not extending the incision and preserved right ventricular function.1 This assumption more than 1-2 cm. Under these circumstances, transannular was affirmed in a significant number of patients who tolerated patches were intentionally downsized and reconstructed the persistent effects of right ventricular volume overload for to result in right ventricular gradients of approximately many years. In a significant number of postoperative patients, 20 mm Hg.11,12 however, long-term complications of pulmonary regurgitation, More comprehensive valve-sparing techniques that in- residual ventricular septal defects (VSD), distal pulmonary cluded a supravalvar pantaloon autologous pericardial patch artery stenosis, right ventricular dysfunction, atrial or ven- for supravalvar pulmonary stenosis were highlighted by – tricular arrhythmias, and exercise intolerance2-5 required several authors.8 10 These -
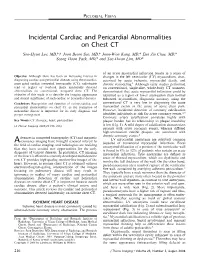
Incidental Cardiac and Pericardial Abnormalities on Chest CT
PICTORIAL ESSAY Incidental Cardiac and Pericardial Abnormalities on Chest CT Soo-Hyun Lee, MD,*w Joon Beom Seo, MD,* Joon-Won Kang, MD,* Eun Jin Chae, MD,* Seong Hoon Park, MD,* and Tae-Hwan Lim, MD* of an acute myocardial infarction results in a series of Objective: Although there has been an increasing interest in changes in the left ventricular (LV) myocardium, char- diagnosing cardiac and pericardial diseases using electrocardio- acterized by acute ischemia, myocardial death, and gram-gated cardiac computed tomography (CT), radiologists chronic remodeling.1 Although early studies performed tend to neglect or overlook many incidentally detected on conventional, single-slice, whole-body CT scanners, abnormalities on conventional, nongated chest CT. The demonstrated that acute myocardial infarction could be objective of this study is to describe the imaging appearance identified as a region of lower attenuation than normal and clinical significance of such cardiac or pericardial diseases. enhanced myocardium, diagnostic accuracy using the Conclusions: Recognition and detection of various cardiac and conventional CT is very low in diagnosing the acute pericardial abnormalities on chest CT as the evaluation of myocardial events as the cause of acute chest pain. noncardiac disease is important for its early diagnosis and However, incidental detection of coronary calcification 2,3 proper management. identifies individuals at risk for acute coronary events. Coronary artery calcification correlates highly with Key Words: CT, thoracic, heart, pericardium plaque burden but its relationship to plaque instability (J Thorac Imaging 2008;23:216–226) is low (Fig. 1). A mild degree of calcification characterizes patients with acute coronary events, whereas diffused high-attenuation calcific plaques are associated with chronic coronary events.4 dvances in computed tomography (CT) and magnetic LV myocardial aneurysms are relatively common resonance imaging have brought renewed interest to A sequelae of transmural myocardial infarction.