7 OA Virological5ppcr2 P769-773.Indd
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of Registered Projects in RERA Punjab
List of Registered Real Estate Projects with RERA, Punjab as on 01st October, 2021 S. District Promoter RERA Type of Contact Details of Project Name Project Location Promoter Address No. Name Name Registration No. Project Promoter Amritsar AIPL Housing G T Road, Village Contact No: 95600- SCO (The 232-B, Okhla Industrial and Urban PBRERA-ASR02- Manawala, 84531 1. Amritsar Celebration Commercial Estate, Phase-III, South Infrastructure PC0089 Amritsar-2, Email.ID: Galleria) Delhi, New Delhi-110020 Limited Amritsar [email protected] AIPL Housing Village Manawala, Contact No: 95600- # 232-B, Okhla Industrial and Urban Dream City, PBRERA-ASR03- NH1, GT Road, 84531 2. Amritsar Residential Estate, Phase-III, South Infrastructure Amritsar - Phase 1 PR0498 Amritsar-2, Email.ID: Delhi, New Delhi-110020 Limited Punjab- 143109 [email protected] Golf View Corporate Contact No: 9915197877 Alpha Corp Village Vallah, Towers, Sector 42, Golf Model Industrial PBRERA-ASR03- Email.ID: Info@alpha- 3. Amritsar Development Mixed Mehta Link Road, Course Road, Gurugram- Park PM0143 corp.com Private Limited Amritsar, Punjab 122002 M/s. Ansal Buildwell Ltd., Village Jandiala Regd. Off: 118, Upper Contact No. 98113- Guru Ansal Buildwell Ansal City- PBRERA-ASR02- First Floor, 62681 4. Amritsar Residential (Meharbanpura) Ltd Amritsar PR0239 Prakash Deep Building, Email- Tehsil and District 7, Tolstoy Marg, New [email protected] Amritsar Delhi-110001 Contact No. 97184- 07818 606, 6th Floor, Indra Ansal Housing PBRERA-ASR02- Verka and Vallah Email Id: 5. Amritsar Ansal Town Residential Prakash, 21, Barakhamba Limited PR0104 Village, Amritsar. ashok.sharma2@ansals. Road, New Delhi-110001 com Page 1 of 220 List of Registered Real Estate Projects with RERA, Punjab as on 01st October, 2021 S. -

Pincode Officename Statename Minisectt Ropar S.O Thermal Plant
pincode officename districtname statename 140001 Minisectt Ropar S.O Rupnagar PUNJAB 140001 Thermal Plant Colony Ropar S.O Rupnagar PUNJAB 140001 Ropar H.O Rupnagar PUNJAB 140101 Morinda S.O Ropar PUNJAB 140101 Bhamnara B.O Rupnagar PUNJAB 140101 Rattangarh Ii B.O Rupnagar PUNJAB 140101 Saheri B.O Rupnagar PUNJAB 140101 Dhangrali B.O Rupnagar PUNJAB 140101 Tajpura B.O Rupnagar PUNJAB 140102 Lutheri S.O Ropar PUNJAB 140102 Rollumajra B.O Ropar PUNJAB 140102 Kainaur B.O Ropar PUNJAB 140102 Makrauna Kalan B.O Rupnagar PUNJAB 140102 Samana Kalan B.O Rupnagar PUNJAB 140102 Barsalpur B.O Ropar PUNJAB 140102 Chaklan B.O Rupnagar PUNJAB 140102 Dumna B.O Ropar PUNJAB 140103 Kurali S.O Mohali PUNJAB 140103 Allahpur B.O Mohali PUNJAB 140103 Burmajra B.O Rupnagar PUNJAB 140103 Chintgarh B.O Rupnagar PUNJAB 140103 Dhanauri B.O Rupnagar PUNJAB 140103 Jhingran Kalan B.O Rupnagar PUNJAB 140103 Kalewal B.O Mohali PUNJAB 140103 Kaishanpura B.O Rupnagar PUNJAB 140103 Mundhon Kalan B.O Mohali PUNJAB 140103 Sihon Majra B.O Rupnagar PUNJAB 140103 Singhpura B.O Mohali PUNJAB 140103 Sotal B.O Rupnagar PUNJAB 140103 Sahauran B.O Mohali PUNJAB 140108 Mian Pur S.O Rupnagar PUNJAB 140108 Pathreri Jattan B.O Rupnagar PUNJAB 140108 Rangilpur B.O Rupnagar PUNJAB 140108 Sainfalpur B.O Rupnagar PUNJAB 140108 Singh Bhagwantpur B.O Rupnagar PUNJAB 140108 Kotla Nihang B.O Ropar PUNJAB 140108 Behrampur Zimidari B.O Rupnagar PUNJAB 140108 Ballamgarh B.O Rupnagar PUNJAB 140108 Purkhali B.O Rupnagar PUNJAB 140109 Khizrabad West S.O Mohali PUNJAB 140109 Kubaheri B.O Mohali PUNJAB -

Details of Issued License to Travel Agent/Consultancy/Ticketing Agent/Ielts Centres in District Rupnagar 06-11-2020
Details of Issued License to Travel Agent/Consultancy/Ticketing Agent/IELTs Centres in District Rupnagar 06-11-2020 License Name of Travel License S.No Office Address Contact no. Licensee Photo No. agent Type Near Railway Kuljinder Singh Crossing s/o Shri Bhoop Travel 1 1 Nangal Chowk, 9872014536 Singh M/s. Moon Agency Rupnagar Stars Enterprises Shop No. 1-2, Nai Abadi Gali No. 1, Anandpur Sahib Now New Rattan lal s/o 98728- Address: Pohu Lal M/s. 89172 Travel 2 2 Opposite R.K. Travels 01887- Agency Railway Agent 230111 Station, Near Cooperative Bank, Railway Road, Shri Anandpur Sahib. Mukesh Kumar Shop No. 247, s/o Sh. Subhash Shastri Travel 3 3 Chand M/s. Rana Building 9855659586 Agency Manpower Railway Road Consultancy Nangal Jaimal Singh s/o Shop No. 51- Sh. Jagdish Ram 52, Mahavir Travel 4 4 M/s. V.V Market Nangal 9417558923 Agency Consultancy Township, Services Nangal Rahul Sharma s/o Shop no. 247, Sh. Suresh Kumar Railway Road Travel 5 5 9878421021 M/s.Shastri Nangal, Teh Agency Travels Nangal Jatinder Mohan s/o Sh. Inderjeet Shop No. 157, Travel 6 6 Mehta Ms. Main Market, 9872649305 Agency Mehta Cyber Teh. Nangal Cafe Raman Taluja s/o Shop No. 218, Sh. Ghuman Railway Road Travel 7 7 Chand Taluja Nangal 9814850449 Agency M/s. Taluja Township, Teh. Communications, Nangal Vikrant Verma Shop No. 95, s/o. Gurbakhsh Ward No. 1, Travel 8 8 7696534512 Rai Verma M/s. Sharma Store, Agency V.V. Consltant Teh. Nangal, Karnail Singh s/o Near Bus Sh. -

Government of Punjab Deptt of Housing and Urban Development (Housing - I Branch)
GOVERNMENT OF PUNJAB DEPTT OF HOUSING AND URBAN DEVELOPMENT (HOUSING - I BRANCH) NOTIFICATION No. 8/2/2001-4HG-1/14429 dated 23rd Dec, 2004. In exercise of powers conferred by section 2 (zi) of the Punjab Regional and Town Planning and Development Act., 1995 and all other powers enabling in this behalf, the Governor of Punjab is pleased to include the following roads in the list earlier notified (up to Sr. No. 26) as scheduled roads:- 1. Morinda – Kurali Road. 2. Morinda (from Km. 0.00 to 6.783) with off take at Km. 61.816 and meeting after crossing the Sirhind – Morinda railway line at Km. 67.800 of Ludhiana – Chandigarh Road i.e., National Highway 22. 3. Kiratpur Sahib – Garha Morah Road (Part of N.H. 21). 4. Kharar – Banur – Tapla Road up to Haryana Border. 5. S.A.S. Nagar – Chunni – Sirhind – Patiala Road. 6. Patiala – Nabha – Malerkotla – Jagraon – Nakodar Road. 7. Gobindgarh – Nabha Bhawanigarh Road. 8. Ludhiana – Malerkotla Sangrur Patran – Munak Road upto Haryana Border. 9. Khanna- Samrala – Machhiwara – Rahon – Nawanshehar Road. 10. Phagwara – Banga – Nawanshehar – Balachaur Road. 11. Phagwara (from Km. 79.85 to Km. 89.385) i.e., taking off from Phagwara – Banga Road to National Highway – 1. 12. Hoshiarpur – Phagwara Road. 13. Hoshiarpur Road up to Himachal Border ( N.H. 70). 14. Nakodar – Kapurthala – Bhulath – Tanda Road. 15. Rayya – Batala – Dera Baba Nanak Road. 16. Batala – Sri Hargobindpur Road. 17. Gurdaspur – Kahnowan – Sri Hargobindpur Road. 18. Gurdaspur – Tibbri Cantt. – Purana Shalla – Naushera Pattan – Mukerian Road. 19. Dakha Mullanpur – Barnala – Mansa – Sardulgarh Road upto Haryana Border. -

District Administration Sas Nagar ਜ਼ਿਲ੍ਹਾ
DISTRICT ADMINISTRATION SAS NAGAR ਜ਼ਿ쩍ਹਾ ꩍਰਸ਼ਾਸ਼ਨ ਘ ਨਗਰﹰਸਾਜ਼ਿਬਜਾਦਾ ਅਜੀਤ ਜ਼ਸ LIST OF VENDORS PROVIDING ESSENTIAL COMMODITIES 爼ਰੂਰੀ ਚੀ爼਼ਾਂ ꩍਰਦਾਨ ਕਰਨ ਵਾਲੇ ਵਵਕਰੇਤਾਵ਼ਾਂ ਦੀ ਸੂਚੀ LIST OF GROCERY SERVING DIRECTLY TO CUSTOMERS IN MOHALI Sr. Store & Shop Name Area Address Details Mobile-No. No. NEAR BALONGI SALES TAX BARRIER, 1 BHUSHAN ENTPERPRISES BALONGI KHARAR-CHANDIGARH ROAD, 9872740334 BADMAJRA SCO 14-15, NEAR POLICE STATION, 2 KAPIL TRADING CO. BALONGI 9814504794, 9814804794 BALONGI 3 SHRI RADHEY TRADERS BALONGI BALONGI 9518417009 4 VEER JI DEPARTMENTAL STORE BALONGI DASHMESH NAGAR, BALONGI 9988547676 SHOP NO. 1, SECTOR 66B, NEAR 5 BHAVYA TRADING CO. KAMBALA 9646183790 ATTA CHAKKI, KAMBALA PHASE 10, 6 AMRITSAR PROVISION STORE # 920, PHASE 10, MOHALI 9872733187 MOHALI PHASE 10, 7 BAKERS HOME PHASE 10, MOHALI 7696544983 MOHALI PHASE 10, 8 RISING SUN DEPARTMENTAL STORE SCF 35, PHASE 10, MOHALI 9517510001 MOHALI PHASE 10, 9 SUBHASH DEPARTMENTAL STORE SCF 57, PHASE 10, MOHALI 8427821201 MOHALI PHASE 11, 10 AMIT DEPARTMENTAL STORE SCF 89, PHASE 11, MOHALI 9056516453 MOHALI PHASE 11, 11 BHARAT TRADING CO. SCF 92, PHASE 11, MOHALI 9888658883, 7696616149 MOHALI PHASE 11, 12 GULATI STORE # 1303/2, PHASE 11, MOHALI 9855806806 MOHALI PHASE 11, 13 LUXMI KARYANA STORE HIG 638A, PHASE 11, MOHALI 9464161733 MOHALI PHASE 11, 14 MANISH SUPER STORE # 1302/3, PHASE 11, MOHALI 9888396274 MOHALI PHASE 11, 15 PAHWA DEPARTMENTAL STORE SCF 104, PHASE 11, MOHALI 8146551117 MOHALI PHASE 11, 16 SABHARWAL SUPER MARKET SCF 48, PHASE 11, MOHALI 9888691553 MOHALI PHASE 11, 17 SINGLA SUPER MARKET SCF 90, PHASE 11, MOHALI 9216700513 MOHALI 18 B.K. -

Department of Drugs Control License Register
License Register Department of Drugs Control Firm: 10134 To: 41348 Sr/Firm No Firm Name , I.C / Manager Firm Address Issue Dt Cold Stor. 24 Hr Open District / R.Pharmacist , Competent Person Renewal Dt Lic App Firm Cons Inspection Dt Circle:SAS Nagar 1 / R 22g medicos/ willow homes, dashmesh nagar,near aman city, 23/03/2017 - 23/03/2017 - 28/02/2017 YES/NO 33860 g.k. sharma/ kharar-140103 G.K. SHARMA SA3 10th, h. no. 342, ward no. 7, master PRO No R.P/No C.P Phon No:8437582476,8437582476,KHR colony kurali, distt. sas nagar *** 20-113769~22/03/22 *** 21-113770~22/03/22 2 / R a.k medicos/ chandigarh road,kurali, - 16/11/2016 - 30/11/2016 YES/NO 32881 achrinder kumar/ kurali- ACHRINDER KUMAR SA3 h. no. 229, master colony,ward no 7, PRO 27158-deepak singla/No C.P Phon No:9041062526,9041062526,KHR kurali, distt.sas nagar *** 20-106429~15/11/21 *** 21-106430~15/11/21 3 / W abhi medicos/ w.no. 9, singhpura road, kurali,kurali, 07/07/2011 - 07/07/2016 - 21/07/2016 YES/NO 27135 gulshan kumar s/o sh. lekh raj/ kurali-140103 Gulshan Kumar S/o Sh. Lekh Raj SA3 10+2, h. no. 167, new colony, sodhia PRO No R.P/gulshan kumar Phon No:9217923244,9217923244,KHR wala bagh, ward no. 10, kurali, distt. sas nagar *** 20B-104012~06/07/21 *** 21B-104013~06/07/21 4 / W advent pharma/ shop no. 2, opp. civil hospital,kharar, - - YES/NO 27132 rajesh arora/ kharar-140301 SA3 PRO No R.P/No C.P Phon No:9815347179,0,KHR *** 20B-/22515-OW~20/03/17 *** 21B-/22301-W~20/03/17 5 / RW aggarwal medical store/ landran road,kharar, 26/04/2016 - 26/04/2016 - 21/03/2016 YES/NO 27936 punit kumar aggarwal s/o late kharar-140301 Punit Kumar Aggarwal SA3 b.com / # 1993-a, ward no. -

Electric Buses…
LUTP REVIEW FOR THE PROJECT REPORT ON TECHNICAL AND FINACIAL VIABILITY OF ELECTRICAL BUSES IN CITY OF CHANDIGARH Presented by:- Amit Gupta CHANDIGARH FORMED IN 1966 CHANDIGARH AS UNION TERRITORY AND CAPITAL OF PUNJAB AND HARYANA PLANNED BY FRENCH ARCHITECT LE CORBUISER ONE OF THE PLANNED CITY OF INDIA IN GRID PATTERN IT HAS AREA OF 114 SQ.KMS AND POPULATION OF 1.05 MILLION WITH POPULATION DENSITY OF 9262 PER KM2 CHANDIGARH TRANSPORT FLEET FOUND IN 1966 WITH JUST 30 BUSES IN ITS FLEET PRESENTLY 533 BUSES(DIESEL) : 130 BUSES FOR INTER CITY OPERATIONS AND 403 FOR INTRA CITY/SUB URBAN OPERATIONS NO PRIVATE OPERATORS/BUSES CTU ROUTES TOTAL OPERATION OF 1,00,000 KMS DAILY FROM 4 DEPOTS 80,000 KMS IN LOCAL/SUB URBAN ON 60 ROUTES 40,000 KMS IN INTER CITY OPERATION ON 54 ROUTES DAILY RIDER SHIP IS 1.60 LAC PASSENGERS LOCAL ,TRICITY ROUTES OF CTU (DEPOT-II) Saketri 71 Mansa Devi Khuda PB Kaimbwala Alisher 18B High I.T Park Cantonment KALKA Civil 211 30A KUBHAHERI 23 Court 18 9A-9C 49 KHIZRABAD Sectt. 2D R.Garden Lake 254 10 Nada Shaib M.TOWN 1 2A-2C M.Majra 30 214 30B Ram Garh 2 3 4 5 6 M.COMP 21382 PEC SARANGPUR HB 5 4 21 KURALI 7 BARRIER 8 2F P.G.I 11 10 9 8 7 26 18 9 10 11 12 17 1238 16 15 14 20 PANCHKULA P.U CTU 15 ISBT 27 28 DHANAS 16 17 18 19 MW Railway Baltana Elante DHAKOLI Station 25 24 23 22 21 20 30 29 26 212 DERABASSI34 80 CHANDIGARH Ram 216 Darbar 17 ZIRAKPUR 38 37 36 35 34 33 32 31 Behlana 143 AIRPORT 39 79 MALOYA 40 41 42 43 44 45 46 47 CHHATBIR Phase-6 56 55 54 LEGEND 53 52 51 50 49 48 TOTAL ROUTE S 34 ISBT RLY. -

Sahibzada Ajit Singh Nagar
DISTRICT DISASTER MANAGEMENT PLAN SAHIBZADA AJIT SINGH NAGAR CONTENTS CHAPTER-01 INTRODUCTION CHAPTER-02 PROFILE OF DISTRICT SAS NAGAR CHAPTER 03 HAZARDS, RISK AND VULNERABILITY ASSESSMENT CHAPTER 04INSTITUTIONAL MECHANISM OF DISASTER MANAGEMENT CHAPTER 05 DISASTER MITIGATION PLAN CHAPTER 06 ACTION (RESPONSE) PLAN FOR EMERGENCY SUPPORT FUNCTIONS CHAPTER 07 DISASTER MANAGEMENT OF DISTRICT SAS NAGAR ANNEXURE 1 LIST OF IMPORTANT CONTACT NUMBERS LIST OF NODAL OFFICERS ANNEXURE 2: Phone Numbers of Kanungo, Sarpanch and Panchayat Secretary ANNEXURE 3: List of School with no. of rooms Unsafe school buildings ANNEXURE 4: List of Hospitals and Veterinary Hospitals . ANNEXURE 5: List of medical team for flood (Block wise) ANNEXURE 6 : List of employées of animal husbandry ANNEXURE 7: List of Firman, Drivers, Gurudwaras and palaces (banquet hall) ANNEXURE 8: List of employees, Food and supply department, contractor’s détails PWD ANNEXURE 9: List of vehicles, Manpower, retired personals, police department ANNEXURE 10:List of ambulance ANNEXURE 11: NGOs OF SAS NAGAR ANNEXURE 12: RESOURCE INVENTORY ANNEXURE 13: Telephone Nos. of all Fire Stations of Fire & Emergency Services, Police posts ANNEXURE 14: Role of District Government Departments/ Agencies in Disaster Management CHAPTER 01 INRODUCTION Disasters like flood whether natural or man-induced are creating a great loss to all sorts of life- human beings, animals, plants and resources- buildings, and infrastructure and above all cause psychological problems. Floods are increasing with the move to material civilization, urbanization and industrialization. With this new cult, even natural disasters are occurring because of the disturbances in natural equilibrium caused by the greed and lust of human beings to exploit natural resources to get rich quickly. -
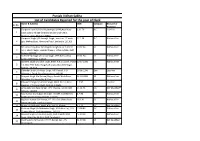
List of Candidates Rejected for the Post of Clerk
Punjab Vidhan Sabha List of Candidates Rejected for the post of Clerk Name & Address DOB Category Reason for Sr.No Rejection Gurpreet Kaur D/O Shri Rajinderpal ,#190,Akali Kaur 3.11.79 B.C. Less Fee 1 Singh colony village- bhavaat Daulat Singh wala, Zirakpur, distt. Mohali,140603 Gurpreet Singh S/O Kamaljit Singh , ward no. 17 main 27.1.94 B.C. Without Fee 2 gali, Mehraj Basti, Rampura Phool, Bathinda, 151103 Ms. Amardeep Kaur D/o Raghbir Singh, H.no 7, Street 30.07.94 SC Without Fee 3 no.1, Shanti Nagar, Beside Phase-1, Urban Estate, Distt Patiala. 147002 Sh Pardeep Singh S/o Jaspal Singh, VPO Nathu Wala 03.01.94 SC Without Fee 4 Jadid, Distt Moga. 142053 Jagmeet Singh S/o Sabh Singh, #584, A.K.S Colony, Phase 29.07.1990 S.C. Without Fee 5 - 2, Near Peer Baba Dargah, ZIrakpur,Distt SAS Nagar, Mohali - 140603 Davinder Singh S/o Kesar Singh, Vill. Panjoli, P.O 30.06.1996 Gen Less Fee 6 Miyanpur, Teh & Distt Roopnagar - 140108 Manjeet Singh S/o Gurmej Singh, Gaadri Wala Road, 21.10.1995 SC Without Fee 7 Ward No. 16, Street No. 8, Zira Talwinder Singh S/o Sohan Singh, Ward No.13, Bassi 1.2.97 S.C. Less Fee 8 Bandian, P.O Banur Distt. Mohali, 140601 Anita Devi D/o Raju Kumar, VPO Tharwa, Teh & Distt. 15.01.91 S.C. Not Qualified* 9 Ambala, 133004 Ravi Kumar S/o Subash Chander, #A-287, Gali NO.7/A, 4.7.92 S.C Without Fee 10 Radha Swami Colony, Fazilka, 152123 Rajinder Kumar S/o Umrao, # E-292, Gali Chitru Ram, 28.3.92 S.C Without Fee 11 Jattian Mohalla, Fazilka,152123 12 Bunty S/o Mahesh Chand, #96, Sec-14, Kharar 4.7.91 S.C Not Qualified Kuldeep -

Kharar Mullanpur Zirakpur Banur Chandigarh
KURALI NAYAGAON MULLANPUR KHARAR SAS NAGAR ZIRAKPUR NH 22 NH 21 PR 4 DERA BASSI MULLANPUR BANUR CHANDIGARH SAS NAGAR BOUNDARY (GIS) ZIRAKPUR OTHER LOCAL PLANNING AREA PR 6 HANDICRAFT CENTRE RESIDENTIAL JHAMPUR MIX USE 1 FLORAL MILE PR 5 MIX USE 2 COMMERCIAL FLORALMILE MANANA JHEURHERI M.C. RESERVE SITE W WHOLESALE CENTRE THASKA (AIRPORT BEHLOL PUR BOUNDARY ALIPUR EXPANSION) E EXPO HASAINPUR KANDALA TARAULI FLORALMILE M.R. INDUSTRY AND WAREHOUSE 56- U JAGATPUR Alpha U HASANPUR 56 MADANPUR 49 55 54 53 52 51 50 48 RESERVE SITE INSTITUTION 122 LANDIALI TO ZIRAKPUR (AIRPORT MOHALI EXPANSION) FOREST & OPEN SPACE RAIPUR BAR MAJRA U SHAFIPUR U KAURU MAJRA RESERVE SITE PARK BT DYALPUR DHARMGARH (AIRPORT E EXPANSION) SPORTS & RECREATION 123 U SIAHI MAJRA KAMBALI PR 7 JANDPUR SIHANPUR FLORAL MILE PR 5 57 58 59 60 61 62 63 RURAL CHHAT 121 64 65 WATER BODY DAUN R.U.B. & AGRICULTURE 120 USE U RURKA RIVER RESERVE 124 HARLALPUR BALONGI NARIANGARH U KUMBRA KAMBALA ROAD U 35'-0" WIDE SERVICE ROAD TARAF KUMBHRA STP BAKARPUR U MATAUR R BT 66- TO BE DEVELOPED AIRPORT FACILITIES AS PER AIRPORT AUTHORITY JHUNGIAN FATEHULLAHPUR CHACHU Beta OF INDIA NORMS U MAJRA PAPRI TRANSPORTATION BALLO MAJRA 35'-0" WIDE SERVICE ROAD 125 119 69 72 CLOVER'S 118 73 70 66- LEAF 71 68 67 66 JUNCTION Alpha DESUMAJRA RAILWAY R.U.B. KISHANPURA U U TO DERABASSI U UTILITY P A T I A L I K I R A O N A D I MAULI TO BE DEVELOPED D A S H M E S H C A N A L U BAIDWAN RESERVE SITE AS PER AIRPORT AUTHORITY BALIALI SOHANA OF INDIA NORMS CHILLA MATRAN BARI RURAL & AGRICULTURE PR 11 NH 21 D A S H M E S H C A N A L 74 82- 126 117 74- U Alpha EXISTING BUILT UP TO ROPAR Alpha 75 76 81 82 CHHAJJU MAJRA CHOE U 77 78 79 80 R.U.B. -
Road Accident Analysis Report
Road Safety Analysis and Identification of Accident Black Spots in S.A.S. Nagar District A Project Under September 2019 Road Safety Analysis and Identification of Accident Black Spots in S.A.S. Nagar District Detailed Report Analysis and Compilation at; Office of the Traffic Advisor Punjab, Second Floor, Punjab Police Complex, Sector 61, S.A.S. Nagar (Mohali) – Punjab – 160062 September 2019 Road Safety Analysis and Identification of Accident Black Spots in S.A.S. Nagar District Research Report Team Charanjeet Road Safety Engineer, S.A.S. Nagar District Project Punjab Vision Zero Edited By Arbab Ahmad Project Manager, Punjab Vision Zero Project Navdeep K. Asija Traffic Advisor Punjab GIS Support Maninder Singh GIS Specialist Saanjh Control Room Police Lines, Ludhiana for S.A.S. Nagar Police Station Boundary Map With Active Support From; Table of Contents EXECUTIVE SUMMARY ..................................................................................................................................... i 1.1. About S.A.S. Nagar Police ............................................................................................................. 1 1.2. Road Accident Scenario in SAS Nagar District............................................................... 3 2. Detailed Road Accidents Analysis of SAS Nagar areas....................................................... 5 2.1. Police Station Wise Road Fatalities ....................................................................................... 5 2.2. Police Station Wise Summary of Accidental -

Plp 2016-17 Sas Nagar
PLP 2016-17 SAS NAGAR Executive Summary Potential Linked Credit Plan is a comprehensive documentation of potentials for rural economic activities, both in physical and financial terms. The PLPs represent an effort at making projections of credit requirements in different sectors in the district taking into account the long term potential, availability of infrastructure, marketing support, credit absorption capacity and other strengths and weaknesses of the credit delivery system at the district level. The theme for the PLP 2016-17 shall be "Accelerating the pace of capital formation in agriculture and allied sector”. SAS Nagar District was created by carving out 2 blocks (Sialba Majri and Kharar) from Ropar district and one block (Derabassi) from Patiala district to function as the 18th district of Punjab w.e.f 14 April 2006. The district has been formed to achieve growth and development as this area is emerging as major I.T.hub of Nothern India. It is officially named after the eldest son of Guru Gobind Singh, Sahibzada Ajit Singh. It, along with Chandigarh and Panchkula, forms a part of the Chandigarh Tricity. Administratively, the district is divided into 3 tehsil viz.,Derabassi, Mohali & Kharar. The important towns in the district are Kharar, Kurali, Mohali, Zirakpur & Dera Bassi. Kharar tehsil is the largest administrative unit of the new district with 192 villages followed by Dera Bassi Tehsil with 132 villages. In all, the district has 3 development blocks consisting of 419 villages. The district is spread over geographical area of 1110 sq. kms. The rural area constitues 1021.77 sq. kms.