Selected Mast Cell Disorder Medical and Scientific References
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Updates in Mastocytosis
Updates in Mastocytosis Tryptase PD-L1 Tracy I. George, M.D. Professor of Pathology 1 Disclosure: Tracy George, M.D. Research Support / Grants None Stock/Equity (any amount) None Consulting Blueprint Medicines Novartis Employment ARUP Laboratories Speakers Bureau / Honoraria None Other None Outline • Classification • Advanced mastocytosis • A case report • Clinical trials • Other potential therapies Outline • Classification • Advanced mastocytosis • A case report • Clinical trials • Other potential therapies Mastocytosis symposium and consensus meeting on classification and diagnostic criteria for mastocytosis Boston, October 25-28, 2012 2008 WHO Classification Scheme for Myeloid Neoplasms Acute Myeloid Leukemia Chronic Myelomonocytic Leukemia Atypical Chronic Myeloid Leukemia Juvenile Myelomonocytic Leukemia Myelodysplastic Syndromes MDS/MPN, unclassifiable Chronic Myelogenous Leukemia MDS/MPN Polycythemia Vera Essential Thrombocythemia Primary Myelofibrosis Myeloproliferative Neoplasms Chronic Neutrophilic Leukemia Chronic Eosinophilic Leukemia, NOS Hypereosinophilic Syndrome Mast Cell Disease MPNs, unclassifiable Myeloid or lymphoid neoplasms Myeloid neoplasms associated with PDGFRA rearrangement associated with eosinophilia and Myeloid neoplasms associated with PDGFRB abnormalities of PDGFRA, rearrangement PDGFRB, or FGFR1 Myeloid neoplasms associated with FGFR1 rearrangement (EMS) 2017 WHO Classification Scheme for Myeloid Neoplasms Chronic Myelomonocytic Leukemia Acute Myeloid Leukemia Atypical Chronic Myeloid Leukemia Juvenile Myelomonocytic -

Green Teeth Associated Hyperbilirubinemia in Primary Dentition
https://doi.org/10.5933/JKAPD.2017.44.3.378 J Korean Acad Pediatr Dent 44(3) 2017 ISSN (print) 1226-8496 ISSN (online) 2288-3819 Green Teeth Associated Hyperbilirubinemia in Primary Dentition Min Kyung Park1†, Yeji Sun1†, Chung-Min Kang1, Hyo-Seol Lee2, Je Seon Song1 1Department of Pediatric Dentistry, College of Dentistry, Yonsei University 2Department of Pediatric Dentistry, College of Dentistry, Kyung-Hee University Abstract There are many reasons for tooth discoloration. An increase in the bilirubin level may cause tooth discolorations. Such cases are rare, but most involve tooth discoloration with a greenish hue. The purpose of this case report is to describe green discoloration of the primary dentition in the presence of neonatal hyperbilirubinemia. 2 boys aged 16 and 22-months presented with chief complaints of erupting teeth of abnormal color. Their primary teeth exhibited a greenish discoloration along enamel hypoplasia. Both patients were born prematurely with a low birth weight and had been diagnosed with neonatal hyperbilirubinemia. Systematic diseases can affect the hard tissue of teeth during their formation and result in changes in tooth color. Periodic follow-ups are required for establishing a normal dental condition and meeting the esthetic needs of patients. A pediatric dentist may be the first person to observe patients with discoloration in their primary dentition. In such cases the dentist can deduce the systematic disease responsible for this discoloration. Key words : Green teeth, Intrinsic discoloration, Hyperbilirubinemia, Bilirubin Ⅰ. Introduction ative materials infiltrate into the tooth structure, their removal is impossible[5-8]. Tooth discoloration can be an esthetic prob- There are many reasons for tooth discoloration, which can lem, and it is one of main reasons why patients visit dentists. -
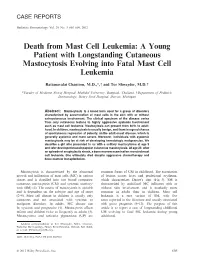
Death from Mast Cell Leukemia: a Young Patient with Longstanding Cutaneous Mastocytosis Evolving Into Fatal Mast Cell Leukemia
CASE REPORTS Pediatric Dermatology Vol. 29 No. 5 605–609, 2012 Death from Mast Cell Leukemia: A Young Patient with Longstanding Cutaneous Mastocytosis Evolving into Fatal Mast Cell Leukemia Rattanavalai Chantorn, M.D.,*, and Tor Shwayder, M.D. *Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand, Department of Pediatric Dermatology, Henry Ford Hospital, Detroit, Michigan Abstract: Mastocytosis is a broad term used for a group of disorders characterized by accumulation of mast cells in the skin with or without extracutaneous involvement. The clinical spectrum of the disease varies from only cutaneous lesions to highly aggressive systemic involvement such as mast cell leukemia. Mastocytosis can present from birth to adult- hood. In children, mastocytosis is usually benign, and there is a good chance of spontaneous regression at puberty, unlike adult-onset disease, which is generally systemic and more severe. Moreover, individuals with systemic mastocytosis may be at risk of developing hematologic malignancies. We describe a girl who presented to us with a solitary mastocytoma at age 5 and later developed maculopapular cutaneous mastocytosis. At age 23, after an episode of anaphylactic shock, a bone marrow examination revealed mast cell leukemia. She ultimately died despite aggressive chemotherapy and bone marrow transplantation. Mastocytosis is characterized by the abnormal common forms of CM in childhood. The excoriation growth and infiltration of mast cells (MC) in various of lesions causes hives and perilesional erythema, tissues and is classified into two broad categories: which characterizes Darier’s sign (Fig. 3). SM is cutaneous mastocytosis (CM) and systemic mastocy- characterized by multifocal MC infiltrates with or tosis (SM) (1). -

Compressive Myelopathy Caused by Isolated Epidural Myeloid Sarcoma with Systemic Mastocytosis
Clinical Notes Compressive myelopathy caused by isolated epidural myeloid sarcoma with systemic mastocytosis. Rare presentation of a hematological malignancy Cyril J. Kurian, MBBS, Indira Madhavan, MBBS, MD, Prabhalakshmi K. Krishnankutty, MBBS, MD, Mekkattukunnel A. Andrews, MD, DM. eurological manifestations of acute leukemia are Ndue to direct involvement by meningeal infiltration and myeloid sarcoma; and indirect involvement by immunosuppression and treatment related side effects. It is rare for myeloid sarcoma to present without bone marrow involvement (isolated myeloid sarcoma or primary granulocytic sarcoma).1 It is even rarer for an isolated myeloid sarcoma to present in the epidural space. We evaluated a case of paraplegia admitted to our department. He had several atypical features that we would like to present in this report. A 39-year-old gentleman with a body weight of Figure 1 - Magnetic resonance imaging of thoracic spine T1W sagittal 58 kg presented with paresthesia and heaviness of view, arrow showing extradural mass at T6 level. both lower limbs of 4 days duration. He was found to have spastic paraplegia with bladder involvement and sensory level at T6. The clinical diagnosis of acute peripheral blood picture showed dimorphic anemia, transverse myelitis was made. Table 1 summarizes the occasional large cells with granular cytoplasm and nucleus with condensed chromatin, and no blast cells. laboratory investigations. The MRI study of the dorsal Ultrasound of the abdomen showed mild splenomegaly. spine (Figure 1) shows that a moderate sized enhancing Urine Bence Jones protein was absent. No M band was posterior epidural component was compressing the seen on serum protein electrophoresis. Bone marrow thecal sac and spinal cord. -

Molecular Profiling of Myeloid Progenitor Cells in Multi-Mutated Advanced Systemic Mastocytosis Identifies KIT D816V As a Distin
Leukemia (2015) 29, 1115–1122 © 2015 Macmillan Publishers Limited All rights reserved 0887-6924/15 www.nature.com/leu ORIGINAL ARTICLE Molecular profiling of myeloid progenitor cells in multi-mutated advanced systemic mastocytosis identifies KIT D816V as a distinct and late event M Jawhar1,8, J Schwaab1,8, S Schnittger2, K Sotlar3, H-P Horny3, G Metzgeroth1, N Müller1, S Schneider4, N Naumann1, C Walz3, T Haferlach2, P Valent5, W-K Hofmann1, NCP Cross6,7, A Fabarius1 and A Reiter1 To explore the molecular profile and its prognostic implication in systemic mastocytosis (SM), we analyzed the mutation status of granulocyte–macrophage colony-forming progenitor cells (CFU-GM) in patients with KIT D816V+ indolent SM (ISM, n = 4), smoldering SM (SSM, n = 2), aggressive SM (ASM, n = 1), SM with associated clonal hematologic non-mast cell lineage disorder (SM-AHNMD, n = 5) and ASM-AHNMD (n = 7). All patients with (A)SM-AHNMD (n = 12) carried 1–4 (median 3) additional mutations in 11 genes tested, most frequently TET2, SRSF2, ASXL1, CBL and EZH2. In multi-mutated (A)SM-AHNMD, KIT D816V+ single-cell-derived CFU-GM colonies were identified in 8/12 patients (median 60%, range 0–95). Additional mutations were identified in CFU-GM colonies in all patients, and logical hierarchy analysis indicated that mutations in TET2, SRSF2 and ASXL1 preceded KIT D816V. In ISM/SSM, no additional mutations were detected and CFU-GM colonies were exclusively KIT D816V−. These data indicate that (a) (A)SM-AHNMD is a multi-mutated neoplasm, (b) mutations in TET2, SRSF2 or ASXL1 precede KIT D816V in ASM-AHNMD, (c) KIT D816V is thus a phenotype modifier toward SM and (d) KIT D816V or other mutations are rare in CFU-GM colonies of ISM/SSM patients, which might explain at least in part their better prognosis. -

Clinical and Etiological Profile of Thrombocytopenia in Adults
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by UKM Journal Article Repository Research Article Clinical and etiological profile of thrombocytopenia in adults: A tertiary-care hospital-based cross-sectional study Shruti K Bhalara, Smita Shah, Hansa Goswami, RN Gonsai Department of Pathology, B.J. Medical College, Ahmedabad, Gujarat, India. Correspondence to: Shruti K Bhalara, E-mail: [email protected] Received September 6, 2014. Accepted September 13, 2014 Abstract Background: The etiologies of thrombocytopenia are diverse. Various studies on thrombocytopenia are done in the past have related to specific etiologies. Objectives: This study attempts to determine the common etiologies of thrombocytopenia in adult patients admitted to Civil Hospital, Ahmedabad. Material and Methods: A cross-sectional study was carried out at Civil Hospital, Ahmedabad. Patients with thrombo- cytopenia more than 18 years of age at admission between 1 October and 31 October 2013 were followed up during their stay in hospital, diagnosis were made, and bleeding manifestations and requirement of platelet transfusion were recorded. Results: From the 412 patients studied, dengue was diagnosed in 28.6% of patients followed by malaria in 22.8%, chronic liver disease in 15.2%, hypersplenism in 12.3%, septicemia in 6.3%, gestational thrombocytopenia and disseminated intravascular coagulation in 5.5%, immune thrombocytopenic purpura (ITP) in 3.1%, megaloblastic anemia in 1.9%, human immunodeficiency virus in 1.4%, drug-induced thrombocytopenia in 1.2%, leukemia in 0.7%, and aplastic anemia in 0.48%. Bleeding secondary to thrombocytopenia was seen in 46 (11.2%) patients; of them, 28 were diagnosed with dengue fever, 4 with chronic liver disease, 3 with sepsis, 2 with hematological malignancies, and 9 with ITP. -

Complications of Laparoscopic Splenectomy
ORIGINAL ARTICLE Complications of Laparoscopic Splenectomy Eduardo M. Targarona, MD, PhD; Juan Jose´ Espert, MD; Ernest Bombuy, MD; Oscar Vidal, MD; Gemma Cerda´n, MD; Vicente Artigas, MD, PhD; Manuel Trı´as, MD, PhD Hypothesis: Analysis of the type and characteristics of Results: One hundred thirteen laparoscopic splenectomies complications after laparoscopic splenectomy may per- were completed (conversion rate, 7.4%). Twenty patients mit the identification of clinical factors with predictive (18%) developed 23 complications. All were Clavien type value for the development of complications. I or II, without mortality. One complication was intraop- erative (diaphragmatic perforation), and 22 were postop- Design: Univariate and multivariate analysis of factors erative: 6 pulmonary (26%), 3 fever (13%), 8 hemorrhagic related to complications in a prospective series of lapa- (35%) (5 episodes of postoperative bleeding and 3 abdomi- roscopic splenectomies. nal wall hematomas), and 6 others (26%). Ten (43%) of the 23 were technically related. Univariate analysis showed Setting: A large tertiary referral university–teaching gen- that complications were only related to age (mean±SD, eral hospital. 55±15 vs 39±17 years; P,.008) or transfusion (50% vs 11%; P,.001). Multivariate analysis showed that the learn- Patients: One hundred twenty-two nonselected con- ing curve (P,.005; 95% confidence interval, 2.46), age secutive patients, in whom laparoscopic splenectomy was (P,.001; 95% confidence interval, 1.04), spleen weight attempted between February 1993 and July 1999. (P,.009; 95% confidence interval, 1.00), and malignant neoplasmdiagnosis(P,.007;95%confidenceinterval,3.82) Intervention: Laparoscopic splenectomy. were independent predictors of complications. Main Outcome Measures: Immediate complica- Conclusions: Laparoscopic splenectomy is feasible, and tions classified according to the Clavien score. -

CASE REPORT Sensorineural Hearing Loss and Tinnitus As Presenting Symptoms of Polycythemia Vera
Int. Adv. Otol. 2012; 8:(2) 317-320 CASE REPORT Sensorineural Hearing Loss and Tinnitus as Presenting Symptoms of Polycythemia Vera Ki-Hong Chang, Eun-Ju Jeon Department of Otolaryngology-HNS, The Catholic University of Korea, Seoul, Korea (KHC, EJ) Abstract: Polycythemia vera (PV) is a blood disorder in which the bone marrow makes too many red blood cells. Commonly encountered neurologic symptoms include transient ischemic attack, dementia, dizziness, tinnitus, and visual disturbances which are thought to result from thrombosis and hemorrhage. Although hearing impairment is one of the neurologic symptoms of PV, tinnitus or hearing impairment as a presenting symptom of PV is very rare. We report a patient with polycythemia vera whose first sign and symptom were bilateral tinnitus and hearing loss. Unfortunately, the hearing was not recovered after treatment including aspirin and phlebotomy while blood level returned to near normal range. Submitted : 16 June 2011 Accepted : 7 November 2011 Introduction hearing loss and tinnitus had developed in his right ear. Polycythemia vera (PV) is characterized by an At that time, he visited another hospital for the hearing erythrocytosis variably associated with leukocytosis loss and was treated with some medication on the and thrombocytosis. PV is a rare disease with an impression of idiopathic sudden hearing loss. However, incidence rate of approximately 1.9-2.3 new cases per as his hearing was not recovered and his tinnitus was 100,000/year in Europe and the United States. The aggravated, he quit taking the medication. After 6 incidence of PV is slightly higher in men than women months, tinnitus gradually developed in his left ear and (2.8 vs. -
Hematologic Disorders
www.downstatesurgery.org Hematologic Disorders Sophia L Fu, MD SUNY Downstate Medical Center, Brooklyn, NY Chief Resident Grand Rounds March 29, 2012 Hematologic Disorderswww.downstatesurgery.org Overview Splenic Peripheral Blood Bone marrow Genetic Disorder Myeloproliferative Hematologic Disorderswww.downstatesurgery.org True or False ??? Therapeutic splenectomy cures the underlying hematologic disorder Hematologic Disorderswww.downstatesurgery.org Goals of Splenectomy Ameliorate the pathologic effects of splenic sequestration and symptomatic splenomegaly Correct the hematologic abnormality Aid in diagnosis and staging Rare www.downstatesurgery.org Autoimmune/Idiopathic Disorders Hematologic Disorderswww.downstatesurgery.org What is the most common indication for splenectomy in the US? A) Felty Syndrome B) Thrombotic Thrombocytopenic Purpura C) Autoimmune Hemolytic Anemia D) Idiopathic Thrombocytopenic Purpura E) Sarcoidosis www.downstatesurgery.org Idiopathic Thrombocytopenic Purpura Hematologic Disorderswww.downstatesurgery.org A 43-year-old man has thrombocytopenia, ecchymoses, and a history of melena. His primary doctor suspects that he might have idiopathic thrombocytopenia purpura (ITP). Which of the following is true about this condition? A It is characterized by a low platelet count, mucosal hemorrhage, normal bone marrow, and an enlarged spleen. B It is caused by splenic overproduction of IgM, which attacks the platelet membrane and causes platelet destruction. C The bone marrow often hypertrophies to counteract the increased platelet destruction. D It affects young men more commonly than women. E Diagnosis requires exclusion of other causes of thrombocytopenia. Hematologic Disorderswww.downstatesurgery.org The patient previously described undergoes a complete work- up and ITP is diagnosed. Which of the following about the treatment of ITP is true? A Platelet transfusions are best given before ligation of the splenic artery. -

©Ferrata Storti Foundation
ORIGINAL ARTICLES Synergistic growth-inhibitory effects of two tyrosine kinase inhibitors, dasatinib and PKC412, on neoplastic mast cells expressing the D816V-mutated oncogenic variant of KIT Karoline V. Gleixner, Matthias Mayerhofer, Karoline Sonneck, Alexander Gruze, Puchit Samorapoompichit, Christian Baumgartner, Francis Y. Lee, Karl J. Aichberger, Paul W. Manley, Doriano Fabbro, Winfried F. Pickl, Christian Sillaber, Peter Valent ABSTRACT From the Department of Internal Background and Objectives Medicine I, Division of Hematology & Hemostaseology (KVG, KS, CB, In a majority of all patients with systemic mastocytosis (SM) including those with KJA, CS, PV); Institute of Immunology mast cell leukemia (MCL), neoplastic mast cells (MC) display the D816V-mutated vari- (AG, WFP), Clinical Institute of ant of KIT. The respective oncoprotein, KIT D816V, exhibits constitutive tyrosine Medical and Chemical Laboratory kinase (TK) activity and has been implicated in malignant cell growth. Therefore, sev- Diagnostics (MM); Center of Anatomy eral attempts have been made to identify KIT D816V-targeting drugs. and Cell Biology, Medical University of Vienna, Austria (PS); Oncology Design and Methods Drug Discovery, Bristol-Myers Squibb, We examined the effects of the novel TK-inhibitor dasatinib alone and in combination Princeton, NJ, USA (FYL); Novartis Pharma AG, Basel, Switzerland with other targeted drugs on growth of neoplastic MC. (PWM, DF). Results Funding: this study was supported by Confirming previous studies, dasatinib was found to inhibit the TK activity of wild type the Fonds zur Förderung der (wt) KIT and KIT-D816V as well as growth and survival of neoplastic MC and of the Wissenschaftlichen Forschung in MCL cell line, HMC-1. The growth-inhibitory effects of dasatinib in HMC-1 cells were Österreich (FWF) grant #P-17205- found to be associated with a decrease in expression of CD2 and CD63. -

Mast Cell Sarcoma: a Rare and Potentially Under
Modern Pathology (2013) 26, 533–543 & 2013 USCAP, Inc. All rights reserved 0893-3952/13 $32.00 533 Mast cell sarcoma: a rare and potentially under-recognized diagnostic entity with specific therapeutic implications Russell JH Ryan1, Cem Akin2,3, Mariana Castells2,3, Marcia Wills4, Martin K Selig1, G Petur Nielsen1, Judith A Ferry1 and Jason L Hornick2,5 1Pathology Service, Massachusetts General Hospital, and Harvard Medical School, Boston, MA, USA; 2Mastocytosis Center, Harvard Medical School, Boston, MA, USA; 3Department of Medicine, Harvard Medical School, Boston, MA, USA; 4Seacoast Pathology / Aurora Diagnostics, Exeter, NH and 5Department of Pathology, Brigham and Women’s Hospital, and Harvard Medical School, Boston, MA, USA Mast cell sarcoma is a rare, aggressive neoplasm composed of cytologically malignant mast cells presenting as a solitary mass. Previous descriptions of mast cell sarcoma have been limited to single case reports, and the pathologic features of this entity are not well known. Here, we report three new cases of mast cell sarcoma and review previously reported cases. Mast cell sarcoma has a characteristic morphology of medium-sized to large epithelioid cells, including bizarre multinucleated cells, and does not closely resemble either normal mast cells or the spindle cells of systemic mastocytosis. One of our three cases arose in a patient with a remote history of infantile cutaneous mastocytosis, an association also noted in one previous case report. None of our three cases were correctly diagnosed as mast cell neoplasms on initial pathological evaluation, suggesting that this entity may be under-recognized. Molecular testing of mast cell sarcoma has not thus far detected the imatinib- resistant KIT D816V mutation, suggesting that recognition of these cases may facilitate specific targeted therapy. -

7/7/2019 1 the CBC And
7/7/2019 The CBC and Me: Identifying and Evaluating Abnormalities Bradley DeNardo, MD Assistant Professor of Pediatrics Division of Pediatric Hematology/Oncology The Warren Alpert Medical School of Brown University Disclosure • No conflicts of interest to disclose. Learning Objectives 1. Describe the diagnostic testing and clinical approach to pediatric anemia. 2. Identify WBC abnormalities suspicious for hematologic disease. 3. Recognize common platelet disorders that result in thrombocytopenia or thrombocytosis. 1 7/7/2019 Blood Basics • Adult blood: • Components of Blood: • Blood volume: 5-6L • Formed elements: blood cells • 7% body weight • Erythrocytes • Circulates the entire body in 20-60 • Leukocytes seconds • Platelets • Plasma • Childhood blood: • 90% water • 10% solutes • Total blood volume: body weight • Neonate: 85 ml/kg • 1 month: 105 ml/kg • >2 months: 70-80 ml/kg • Serum = plasma without clotting factors Blood Basics • Hematopoiesis: • Continuous production of blood cell population. • Bone marrow cavities and canals. • Mediated: • Growth factors • Hematopoietic stem cells Blood Basics 2 7/7/2019 Blood Basics Blood Basics: The CBC • Other values: • Red Blood Cell Indices: • MCV • MCH • MCHC • RDW • MPV Blood Basics: The CBC Manual Automated 3 7/7/2019 Blood Basics: The Red Blood Cell • Biconcave disc • 7.8 μm diameter • Highly flexible membrane • 100-120 day lifespan • 3.9-6 million cells/μl • Produce 2.4 million RBCs/second • Simple interior: • Lack of nucleus • Lack of organelles • Enzymes for glycolysis • Hemoglobin Blood Basics: Hemoglobin • Iron-containing metalloprotein. • Structure • Responsible for O transport. • Heme Group: 2 • Protoporphyrin IX • 35% of total RBC content. • Single atom of Iron • 96% by dry content • Globin: • Polypeptide chain • Heme + Globin = Hemoglobin Chain: • 16,000 g/mol • Variety of different chains • Hemoglobin Protein: • 4 loosely bound hemoglobin chains Blood Basics: Hemoglobin 4 7/7/2019 Blood Basics: The Newborn Screen Pediatric Anemia • Defining Anemia: • Reduction in RBC mass.